


Abstract
Background/Aim: Exercise training usually complements pharmacological therapy of type 1 diabetes mellitus, however, little is known about its impact on cardiac autonomic neuropathy. Our aim was to evaluate the impact of exercise on electrocardiographic parameters and heart rate variability in diabetic rats. Materials and Methods: Wistar rats were randomly assigned to four groups (n=12): Sedentary control (SC), sedentary diabetic (SD), exercise control (EC), and exercise diabetic (ED). Diabetes was induced by a single intraperitoneal injection of streptozotocin (45 mg/kg). Exercise groups underwent 8 weeks of training on a treadmill. At the end of the study, echocardiography was performed and continuous electrocardiographic recording was obtained by intra-abdominally implanted telemetric devices. Diabetes induction significantly reduced the heart rate and increased the blood glucose level (p<0.001) and R-wave amplitude (p<0.05). Frequency-domain spectral variables were also analyzed. The SD group had a significantly lower absolute high-frequency component (p<0.05) and higher normalized low-frequency component, as well as low-frequency power divided by the high-frequency power ratio when compared to the SC and EC groups (p<0.05). All these diabetes-related adverse changes in heart rate variability parameters were significantly reversed by exercise training (p<0.05). Overall, our study shows that early initiation of systemic exercise training prevents the development of cardiac autonomic neuropathy in rats with type 1 diabetes mellitus, by favorable change in the balance between parasympathetic and sympathetic activity.
Diabetes mellitus (DM) is a severe, multifaceted disease with growing prevalence worldwide and detrimental economic impact on health systems (1). Among cardiovascular complications, cardiac autonomic neuropathy (CAN) has been associated with increased morbidity and mortality in the diabetic population (2). Patients with CAN have vagal impairment, which may shift sympathovagal balance towards predominant sympathetic nervous activity. Heart rate variability (HRV) provides a non-invasive, feasible and reproducible measure of autonomic nervous system function, early detector of autonomic abnormalities. Most recently, HRV has been recognized as an index of CAN in patients with type 1 diabetes mellitus (T1DM) (3). Reduced HRV in the diabetic population is correlated with high rates of arrhythmia, sudden cardiac death and morbidity (4). Diabetes-associated CAN has been associated with left ventricular systolic and particularly diastolic dysfunction, for which interstitial myocardial fibrosis and microangiopathic or metabolic derangements may be predominantly responsible (5).
Regarding electrocardiographic (ECG) parameters, QT and QTc intervals are valid predictors of heart disease and fatal ventricular arrhythmia (6). The prevalence of a prolonged QTc interval is higher in people with diabetes as compared to non-diabetic individuals (7). In DM, CAN is proposed to be related to QT interval prolongation and thus increased mortality rate (8). Moreover, QRS duration and R-wave amplitude (RWA) are early indicators of evolving cardiovascular disease and increased cardiovascular risk (9).
Exercise training constitutes an adjunct of pharmacological therapy of DM and its complications (10-12). Across physiological and pathological conditions, exercise training seems to increase HRV and improve autonomic function (13-15). Previous studies have shown diminished DM-linked bradycardia in exercise-treated animal models (16, 17). Further studies have consistently demonstrated the association of exercise-induced improvement of parasympathetic function and sympathetic outflow (neurohormonal), with reduced cardiovascular mortality (18, 19). However, little is known about the impact of exercise on CAN and electrical conductivity in patients with T1DM.
In the present study, the changes in heart rate (HR), ECG parameters and autonomic control of the cardiovascular system induced by exercise training were evaluated in a streptozotocin-induced diabetic Wistar rat model. This rat model is routinely used to investigate diabetes and its related complications. There are few data in the literature about the effects of exercise on cardiac autonomic, electrophysiologic and hemodynamic function in experimental T1DM. Our study aimed to address this gap in the current literature.
Materials and Methods
Animals and overall protocol. A total of 48 male Wistar rats (Charles Rivers Laboratories, Milan, Italy) were entered into the experimental protocol at the age of 12 weeks (mean weight=270-340 g). The rats were randomly assigned to the following equivalent (n=12) groups: i) Sedentary control (SC), ii) sedentary diabetic (SD), iii) exercise control (EC), and iv) exercise diabetic (ED). Animal housing was under specific-pathogen-free conditions. Tap water in drinking bottles and pelleted rat chow were provided ad libitum. Food and water consumption were monitored daily. Rat weight was also recorded daily in order to detect any rapid unexpected weight loss.
The whole duration of the study was 8 weeks. At the end of the study (20 weeks of age), the rats were anesthetized using isoflurane (Forenium; Abbott, Athens, Greece). During the anesthesia procedure, oxygen was continuously delivered via a rodent face mask with flow rate of 1.5 l/min. Echocardiography (ECG) and intraperitoneal (i.p.) implantation of transmitter were performed as described below. Rats were left for 48 hours in their cages to recover from the surgical procedure then serial ECG measurements from transmitters were obtained. Finally, all rats were euthanized under deep anesthesia. The study complied with the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health. The protocol was approved by the Ethics Committee for Animal Experimentation of the Biomedical Research Foundation (no 4553), Academy of Athens, Greece and the competent Veterinary Service (no VS983).
Diabetes. Diabetes was induced in the experimental groups at the beginning of the study by a single i.p. injection of streptozotocin (Sigma, St. Louis, MO, USA) at 45 mg/kg dissolved in sodium citrate buffer (0.1 M, pH 4.5). This is a valid animal model of T1DM (20). Hyperglycemia was confirmed 3 days after the injection by blood sampling (as non-fasting glucose >300 mg/dl or fasting glucose >220 mg/dl). In the control animals, an equal volume of 0.1 M sodium citrate buffer (pH 4.5) was injected i.p.
Throughout the experiment, there was continuous monitoring of diabetes induction by measurement of the glucose level in blood from the tail of each rat using Accu-Chek Advantage glucometer (Boehringer Mannheim Corporation, Indianapolis, IN, USA) every 2 weeks. The diabetic state of the rats was also confirmed by cardinal symptoms, such as weight loss, polydipsia, polyuria, and polyphagia. Fasting blood samples were obtained under isoflurane anesthesia at the beginning, via tail vein puncture, and at the end of the study, via cardiac puncture before euthanasia. Blood samples were centrifuged at 1,000 × g for 5 min and the serum was separated. Fasting plasma glucose was determined using an automated enzymatic technique (Chemwell 2910; Awareness Technology Inc., Palm City, FL, USA).
Exercise protocol. Exercise training was performed on a motorized rodent treadmill with electrical shock-plate incentive (Exer-6M Open Treadmill; Columbus Instruments, Columbus, OH, USA) for 8 weeks, 5 days a week. During the first 4 weeks, the duration of exercise and the speed were gradually increased from 30 to 60 min/day and from 18 m/min to 24 m/min, respectively, while the incline remained stable throughout the study at 10°. There was a 2-min rest interval at the middle of each session. The latter exercise training parameters remained unaltered until the end of the study. Sedentary rats were placed on a stationary treadmill without training.
Echocardiography. Two-dimensional ECG was performed in anesthetized rats using a commercially available 12-MHz linear array transducer system (Logiq e-vet, 12L-RS probe, 5-13 MHz; GE, New York, USA). The animals were placed in the left lateral decubitus position. Left ventricular end-diastolic (LVEDd) and end-systolic (LVESd) diameters were measured. Septal and posterior wall thicknesses were measured from the leading edge. The left ventricular ejection fraction (LVEF) was calculated.
Transmitter implantation. After local anti-septic procedures and anesthesia, a telemetric device (TA10ETA-F20, DSI) was implanted in the abdominal cavity of each animal. Through subcutaneous tunnels, one lead of the device was fixed at the right clavicle, while the other lead was positioned at the left part of the thorax. The leads were sutured in place with a Vicryl 3-0. The electrodes from the transmitter were arranged in the Einthoven bipolar lead II configuration.
Telemetry. Heart biopotentials were monitored using a biotelemetry system (Data Sciences International Corp., St Paul, MN, USA). The system comprised the receiver plates (RPC-1), a data-exchange matrix (consolidation matrix; 20CH), and specialized software (Dataquest LabPro Version 4.0) for system configuration, control, acquisition and storage in a personal computer. Each cage with the rat subject was placed over the receiver plate. HR values and ECG curves were recorded for 30 minutes, 2 days after implantation.
ECG parameters were estimated using a MATLAB image digitizing system (MATLAB 7.8, R2009a, Natick, MA, USA) by an observer without prior knowledge of or references to the results of the experiment. The QRS interval was measured first, which is the time from the Q-point to the S-point of the QRS complex and represents the electrical forces generated by ventricular depolarization. Subsequently, the QT interval, which represents the total time taken for depolarization and repolarization of the ventricles, was measured from the onset of the QRS complex to the end of the T-wave, i.e. return to TP isoelectric baseline. The average of three consecutive QRS and QT intervals was considered. QT intervals were corrected for HR using Bazett's formula (QTc=QT/√RR) (20). The R-wave is the initial positive or upward deflection of the QRS complex in the electrocardiogram and the amplitude was measured in millivolts from the PQ segment to the top of the R-wave and averaged over three consecutive beats. The orientation of the T-wave in lead II, which represents the repolarization of the ventricles, is normally positive and its amplitude was measured from the isoelectric baseline to the peak of the T-wave.
Animal characteristics at baseline and at the end of the study. The results are expressed as mean±SE.
The irregularly time-sampled inter-beat (RR) interval signal was then calculated. In the frequency-domain analysis, power spectral density (PSD) of the RR series was calculated using two methods: (i) Nonparametric, using fast Fourier transform, and (ii) parametric, based on autoregressive models. The PSD was analyzed by calculating powers and peak frequencies for different frequency bands. The commonly used frequency bands are very low frequency (VLF, 0-0.5 Hz), low frequency (LF, 0.5-0.8 Hz), and high frequency (HF, >0.8 Hz). The most common frequency-domain parameters include the powers of VLF, LF, and HF bands in absolute (aVLF, aLF, aHF) and relative values (pVLF, pLF, pHF), the normalized power of LF and HF bands (nLF, nHF), and the LF/HF ratio. These normalized values represent the relative value of each power component in proportion to the total power minus the VLF component and eliminates possible artifacts. A detailed description of that procedure has been previously reported (22). In our study, the fast Fourier transform PSD was calculated using the Welch periodogram, by dividing the time series into a constant number of segments, overlapping by 50%. After application of a Hanning window and subtracting the mean value, the segment periodogram was calculated and the power spectra of all segments were averaged.
Statistical analysis. Data are expressed as mean±standard error (SE). Normality of distribution was assessed with Kolmogorov–Smirnov test. Comparison between groups was performed using one-way analysis of variance (ANOVA) with post-hoc Tukey test. Paired-sample t-test evaluated the differences of variables within groups. Differences were considered statistically significant at a p-value less than 0.05. For the statistical analysis, SPSS software package (version 16.0; SPSS Inc, Chicago, IL, USA) was used.
Results and Discussion
General characteristics of animals. Animal characteristics and cardiac function parameters are summarized in Table I. Body weights were similar in all experimental groups at baseline. Weekly mean body weights are plotted in Figure 1A. In the diabetic groups, SD and ED, body weight was significantly reduced while water and food intake was increased compared to controls (p<0.05) (Figure 1). Interestingly, the weight difference by study end in the exercising animals, ED and EC, was smaller compared to their control counterparts, SD and SC (ΔWED=−9.42±8 g vs. ΔWSD=−23.8±8.7 g and ΔWEC=50.68±5.96 g vs. ΔWSC=107.6±2.9 g). However, these differences were statistically significant only in the case of the control animals (p<0.05). Exercise training did not significantly affect glucose levels of diabetic (p=0.204) and non-diabetic (p=0.997) groups (Figure 2).
The streptozotocin-induced diabetic Wistar rat model has been previously used in studies related to T1DM (23, 24). Indeed, herein, we verify that all diabetic rats exhibited significant 5- to 6-fold increase in blood glucose level and loss of body weight, despite polydipsia and polyphagia (Table I). Our exercise protocol partially attenuated hyperglycemia and diabetes-induced weight loss. Although these results may indicate an improvement in the metabolic state, they outline the inadequate efficiency of systemic exercise in completely reversing the detrimental metabolic effects of T1DM. However, even those modest effects are of clinical relevance and patients with T1DM should be encouraged to follow exercise instructions.
As far as HR is concerned, in the sedentary groups, diabetic rats appeared to have a lower HR than non-diabetic rats (SC vs. SD, p<0.001) (Table I), in agreement with previous studies (16, 17). Bradycardia might represent autonomic neural dysfunction and sinoatrial node impairment caused by streptozotocin-induced diabetes (17, 18, 24). Exercise lowered HR only in the non-diabetic rats (SC vs. EC, p=0.011). This is consistent with a previous study demonstrating a lower resting HR in normotensive rats after exercise training (26). It is possible that enhanced vagal, or reduced sympathetic cardiac tone, as well as a reduction in the discharge frequency of the sinoatrial node may explain the bradycardic effect of exercise (26-28). Interestingly, exercise training slightly elevated HR in diabetic rats compared to their sedentary counterparts (SD vs. ED, p=0.345) (Table I). In agreement with previous reports, we also observed a trend for higher resting HR in trained diabetic rats, reinforcing the argument that exercise training may attenuate diabetes-induced bradycardia (16, 17, 29, 30). De Angelis et al. suggested that the increase in resting HR in trained diabetic rats may be related to the improvement of intrinsic pacemaker regulation, based on the fact that exercise did not induce any change in sympathetic tonus (16).

Weekly mean animal weight (A), food intake (B) and water intake (C) measurements per rat. Data are presented as the mean±SE for each group of rats: sedentary control (SC), sedentary diabetic (SD), exercise control (EC), and exercise diabetic (ED).
Comparison of ECG findings is shown in Table I. Exercise training tended to increase left ventricular ejection fraction (LVEF) only in non-diabetic animals (SC vs. EC, p=0.111). Our study did not demonstrate a statistically significant change in LVEF in the diabetic rats, in agreement with a previous study (31). This result indicates that in this particular animal model, diabetes leads to preservation of cardiac systolic function, which is not affected by exercise training.
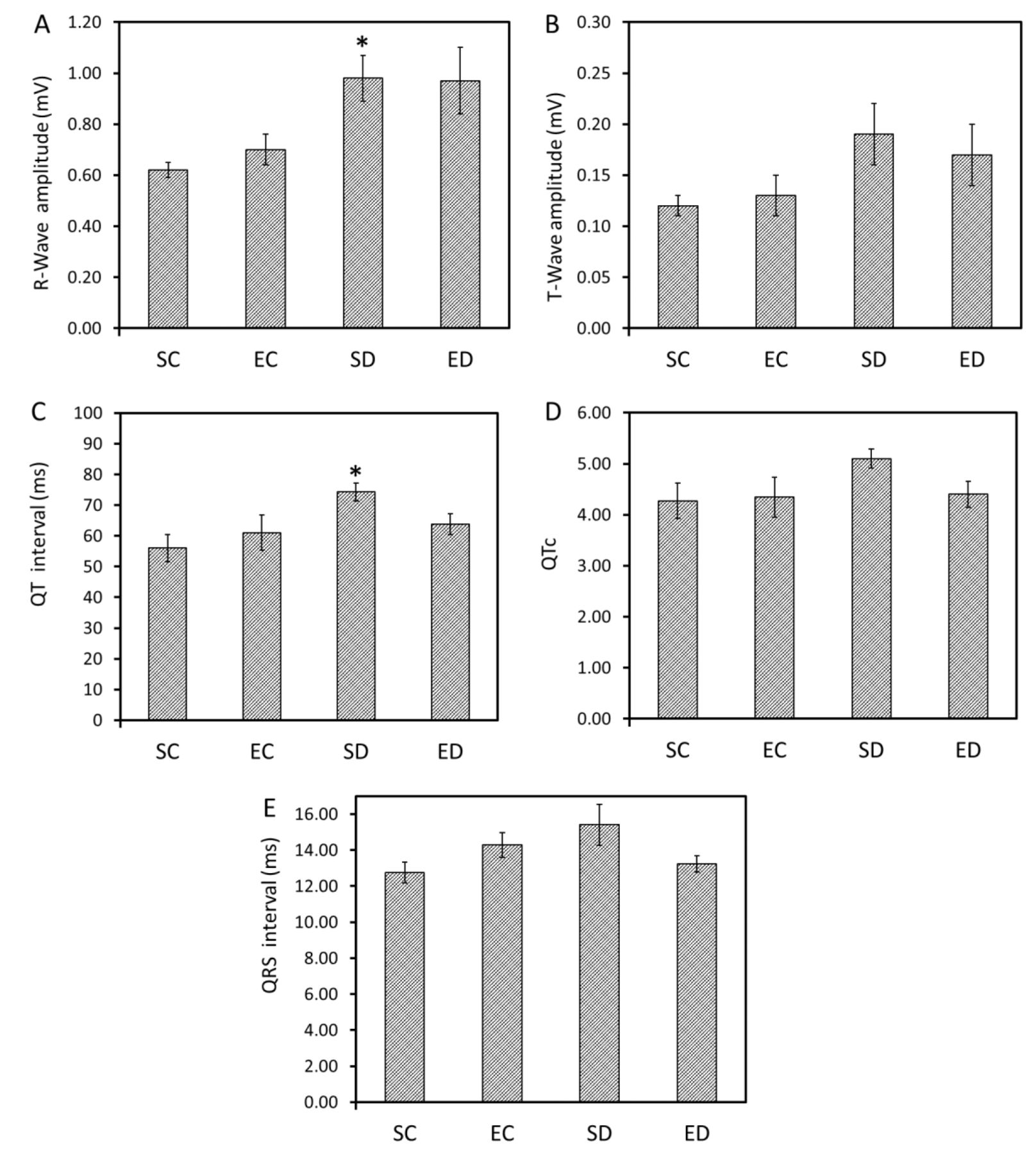
ECG wave amplitude and ECG intervals. We examined the impact of diabetes and exercise training on the R-and T-wave amplitudes. DM induction increased the RWA only in sedentary animals (SD vs. SC, p=0.027) (Figure 3A). This increase of RWA noted in sedentary diabetic rats may indicate heart hypertrophy due to myocardial damage and fibrosis (32-34). Interestingly, exercise training had no significant impact on RWA (p>0.05). Moreover, no significant differences between groups in T-wave amplitude were detected (Figure 3B).
The QTc interval provides a measure of ventricular repolarization-depolarization associated with electrical events. As shown in Figure 3C and D, in SD animals QT and QTc intervals were wider than in SC animals but only statistically significantly for QT (p=0.012 and p=0.176, respectively). The observed prolongation of the QT interval constitutes an important electrophysiological alteration (35). Among the factors that may lead to this prolongation is the delayed inactivation of the L-type Ca2+ current, and reduction in Ca2+-independent transient outward K+ current and steady-state outward K+ current (36). Exercise training reduced the QT and QTc intervals in diabetic animals, but that effect did not achieve a statistically significant level (p=0.278 and p=0.335, respectively). Widening of the QRS interval, a sign of abnormal intraventricular conduction, was observed only in SD animals, however, it was not statistically significantly increased (SC vs. SD, p=0.120) (Figure 3E).

Blood glucose level at week 0 and 8 of the study. Data are presented as the mean±SE for each group of rats: sedentary control (SC), sedentary diabetic (SD), exercise control (EC), and exercise diabetic (ED).
In our study, exercise training did not significantly affect the cardiac anatomic and electrophysiological parameters investigated herein. Further investigation is required in order to clarify whether exercise training may correct depolarization and repolarization abnormalities. The underlying mechanisms and their clinical output are still obscure.
Heart rate variability. Spectral analysis of continuous ECG recording and HRV components may provide information about sympathetic and parasympathetic nervous system activities (37). HF power is generally defined as a marker of vagal modulation, while LF power, particularly when expressed in normalized units, can be considered a measure of sympathetic modulations or a combination of sympathetic and parasympathetic activity (37). Importantly, the LF/HF ratio illustrates the sympathovagal balance. We therefore calculated the abovementioned properties to investigate the impact of exercise training on cardiac autonomic function in DM.
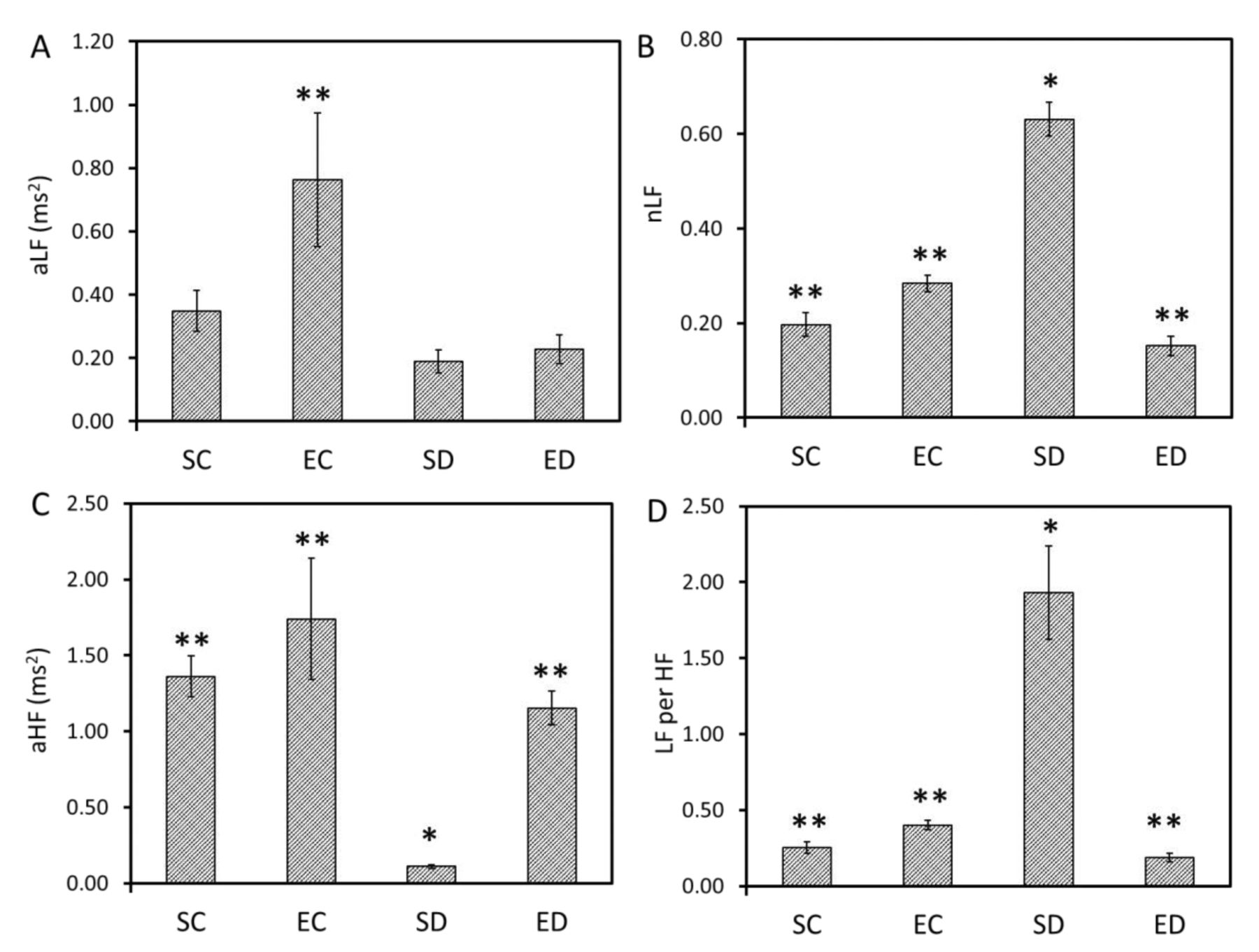
The most common finding in diabetic patients with CAN is reduced power in all spectral bands in frequency HRV analysis (38). Previous data have suggested functional impairment in both parasympathetic and sympathetic branches of the cardiac autonomic nervous system in patients with T1DM compared to healthy controls (39-41). In our study, we confirmed an autonomic imbalance in our diabetic rats, since the SD animals exhibited a decrease in HRV PSD at high frequencies and an increase of both nLF and LF/HF ratio compared to controls (p<0.05) (Figure 4). These results implicate vagal depression and a distinct sympathetic predominance.
The impact of exercise training on HRV has been widely investigated (42-46). In non-diabetic rats, exercise training did not significantly influence the abovementioned parameters of HRV (nLF, LF/HF, aHF) (p>0.05), in agreement with previous study (30). However, one of the most striking findings of our study was the favorable attenuation of autonomic cardiac dysfunction as depicted by the regression of HRV disorders (decreased aHF and increased nLF and LF/HF ratio) after 2-month aerobic exercise training (p<0.05). Thereby, at the end of our study, diabetes-related HRV impairment was almost reversed, returning HRV values to levels of non-diabetic rats.
Our results implicate the high efficiency of early exercise initiation to prevent the development of diabetic CAN. A recent study showed aerobic exercise in both type 1 and 2 diabetes to significantly improve HRV and cardiac autonomic function, in favor of parasympathetic dominance, independently of body mass index, glycemic control and duration of diabetes (47). It is possible that the high predisposition to neural dysfunction associated with diabetes is a prerequisite for exercise treatment to enhance vagal modulation and create a parasympathetic predominance, which could provide electrical stabilzation of the heart.
Considering the underlying mechanisms, the sympathetic and parasympathetic dysfunction observed in the streptozotocin-induced model of diabetes can be correlated with biochemical and morphological changes in adrenergic and cholinergic systems. Previous investigators suggested either a reduced acetylcholinesterase level or increased number of muscarinic receptors in atria of streptozotoc-induced diabetic rats (48, 49). The bradycardic response to muscarinic stimulation may be enhanced in streptozotoc-induced diabetic rats. All this suggests receptor hypersensitivity, while exercise training might have restored parasympathetic activity through still not well-known mechanisms. This could be of clinical significance since exercise training has been demonstrated to reduce cardiovascular mortality and sudden cardiac death by reducing the risk of frequently lethal ventricular arrhythmias through enhanced vagal cardiac modulation (42). Mostarda et al. demonstrated that exercise training improved survival rate by 84% in diabetic rats compared with sedentary ones (17). Undoubtedly, more research is required to substantiate these speculations.
Study limitations. This study has some limitations we must acknowledge. Despite the absence of assays of skeletal muscle activity, such as citrate synthase activity, the observed HR responses are by themselves good indicators of the effectiveness of the training program. Moreover, in order to correctly assess the significance of the different regions of the power spectrum of HRV, respiration should be measured or controlled breathing performed. Nevertheless, in the present study, such a measurement was not possible. Another possible limitation of the present study is that the pattern of development of autonomic neuropathy is probably dependent on the rat strain used and animal age when streptozotocin is administered and thus any conclusions should be made with caution and based on the conditions of the employed protocol. In the ECG measurements, factors such as electrical axis deviations, altered electrode positions, and differences in chest wall thickness may alter RWA.

A: T-Wave amplitude, B: R-wave amplitude, C: QT, D: QTc and E: QRS interval for the different groups (8-11 animals per group). SC: Sedentary control; SD: sedentary diabetic; EC: exercise control; E: exercise diabetic. Data are presented as the mean±SE for each group. *Significantly different from SC at p<0.05.

Heart rate variability data for the different study groups (6-9 animals per group): A: aLF (absolute low frequency), B: nLF (normalized power of low frequency bands), C: aHF (absolute high frequency) and (d) LF/HF (low to high frequency ratio). SC: Sedentary control; SD: sedentary diabetic; EC: exercise control; E: exercise diabetic. Data are presented as the mean±SE for each group Significantly different from *SC and **SD at p<0.05. No significant differences were detected between SC, EC and ED for any of the parameters.
Conclusion
To conclude, our training program significantly ameliorated parameters of low HRV (nLF, LF/HF ratio, aHF) in diabetic rats. On the other hand, exercise training conferred only slight, not significant changes in other pro-arrhythmic parameters, such as QT, QTc, QRS duration, as well as R-wave amplitude. Those effects of exercise training on T1DM-related CAN are of particular importance. Another important contribution of the present study is that it provides information about the singular effects of exercise training on T1DM. This is of particular importance since most patients that regularly exercise also make a variety of other healthy lifestyle choices.
Finally, the present study reinforces the notion that exercise training can be used as a non-pharmacological approach to improve cardiovascular autonomic function in an experimental model of T1DM. The early implementation of exercise therapy may alleviate DM-induced low HRV and abnormalities in ECG by increasing vagal modulation and reducing sympathetic dominance. Moreover, our results outline the necessity for sustained recommendation of exercise training at the earliest stage of T1DM, prior to or at initial stages of CAN development. Further research is needed to identify the exact exercise regimen (i.e. duration and intensity) that leads to optimal improvements in HRV.
Acknowledgements
Financial support was provided to Nikolaos P.E. Kadoglou by the Hellenic Cardiological Society.
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors declare that there is no conflict of interests regarding the publication of this article.
- Received July 7, 2018.
- Revision received September 25, 2018.
- Accepted September 27, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.