


Abstract
Background/Aim: The anticancer immune response has been reported to contribute to the success of chemotherapy. The aim of this study was to evaluate the significance of the measurement of tumor-infiltrating lymphocytes (TILs) in the primary tumor using the method proposed by the International TILs Working Group as a prognostic marker of chemotherapeutic outcomes in patients with stage IV colorectal cancer (CRC). Patients and Methods: A total of 57 patients with stage IV CRC who underwent palliative chemotherapy after resection of the primary tumor were enrolled. Hematoxylin and eosin (H-E)-stained tumor sections were used for the evaluation of TILs. The density of TILs was assessed by measuring the area occupied by mononuclear inflammatory cells over the total stromal area at the invasive margin. Immunohistochemistry for CD8 was also performed, and the number of immunoreactive cytotoxic T-lymphocytes (CTLs) at the invasive margin was counted. Results: Thirty patients were classified into the high-TILs group, and 27 patients were classified into the low-TILs group. The high-TILs group had a significantly higher chemotherapeutic response rate (79.3% vs. 48.1%, p=0.025) and better progression-free survival (median survival time: 10.1 m vs. 7.3 m, p=0.0133) than the low-TILs group. Furthermore, the high-TILs group had a significantly better overall survival than the low-TILs group (median survival time: 35.5 m vs. 22.4 m, p=0.0221). The density of TILs evaluated using the H-E-stained sections showed a strong association with the number of CTLs (p<0.001). Conclusion: The measurement of TILs in the primary tumor using the method proposed by the International TILs Working Group can be used as a prognostic marker of the clinical effectiveness of palliative chemotherapy in patients with stage IV CRC.
Colorectal cancer (CRC) is one of the most common causes of cancer-related death worldwide (1). About 20-25% of patients with newly diagnosed CRC present with distant metastases (2-4), and only a small population of these patients can undergo curative operation (5). For patients with unresectable metastatic tumors, the standard treatment is systemic chemotherapy. As mentioned in the ESMO clinical practice guidelines (4), an individualized approach to clinical decision-making should be adopted according to the patient's stratification. Therefore, numerous attempts have been made to identify useful prognostic markers for accurate patient stratification.
Anticancer immunity is known to affect cancer progression (6). Tumor-infiltrating lymphocytes (TILs), which reflect the immune status of the host (7), have been reported to correlate with the clinical outcome, including the chemotherapeutic outcome in patients with various types of cancer (8-10). However, the method of measuring TILs has differed among previous reports (11-15). Recently, a new method of measuring TILs in breast cancer was proposed by the International TILs Working Group, using H-E-stained sections (16). In the current study, we applied this method to CRC.
The aim of the present study was to evaluate the significance of the TILs in the primary tumor as a marker for predicting the chemotherapeutic outcome in patients with stage IV CRC using the method proposed by the International TILs Working Group.
Patients and Methods
Patients. We retrospectively reviewed a database of 57 patients who underwent palliative combination chemotherapy for unresectable metastatic colorectal cancer after resection of the primary tumor at the Department of Surgical Oncology of Osaka City University between 2005 and 2010.

Representative pictures of intratumoral inflammatory cell infiltration by Hematoxylin-Eosin staining (×400). (A) High density of inflammatory cell infiltration. (B) Low density of inflammatory cell infiltration.
Evaluation of TILs using H-E-stained sections. The density of TILs in the H-E-stained sections was evaluated in accordance with the method outlined in a previous report (16). Briefly, the density of TILs was assessed by measuring the area occupied by mononuclear inflammatory cells over the total stromal area at the invasive margin (Figure 1). With this method, only the stromal area should be evaluated, and the areas occupied by cancer cells should be excluded from the evaluation. A full assessment of the average density of TILs should be used, and hotspots should not receive focused attention. We set 50% as the cut-off value for the evaluation of TILs using the H-E-stained sections in accordance with the verification experiment of the methodology proposed by the International TILs Working Group (17). We then classified the patients into a high-TILs group and a low-TILs group based on this cut-off value.
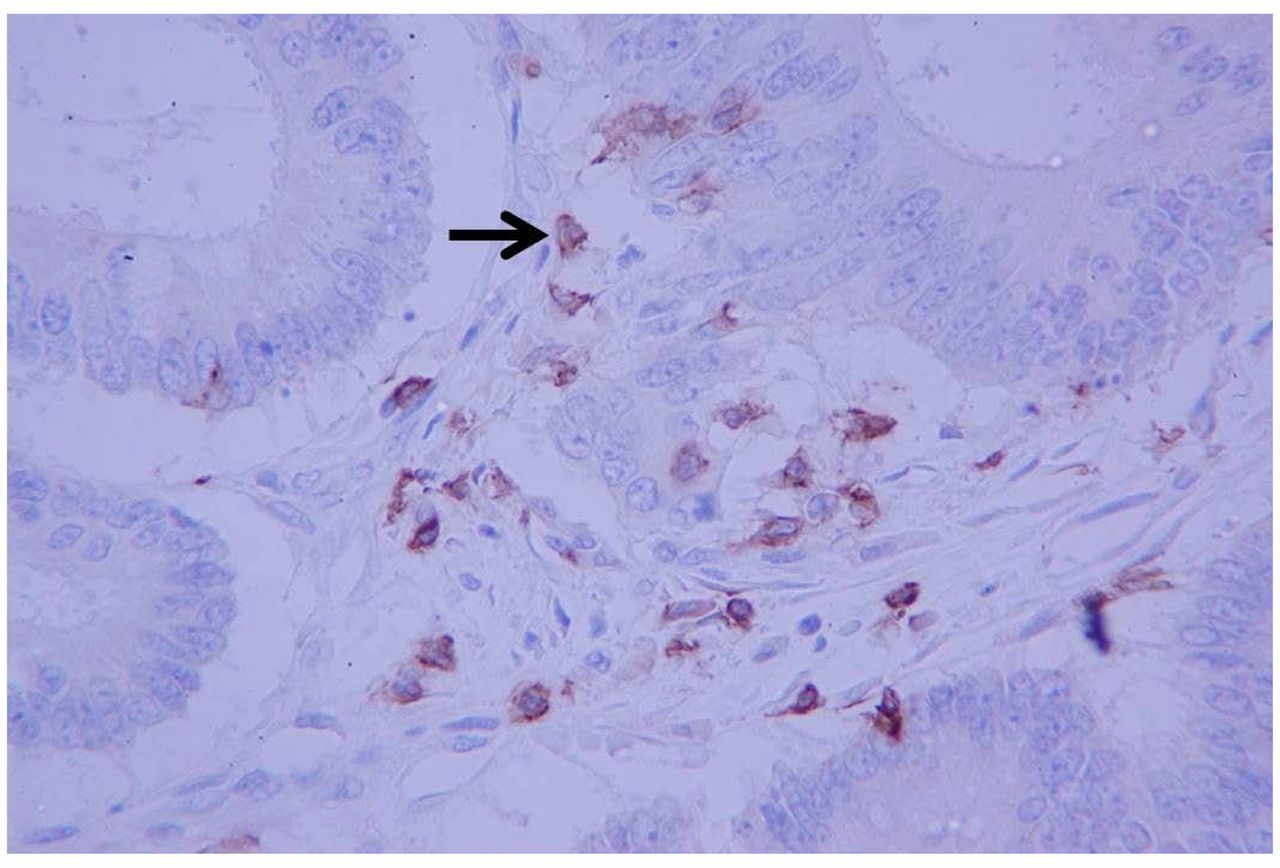
Immunohistochemistry. We performed immunohistochemistry to evaluate the cytotoxic T-lymphocytes (CTLs). Surgically resected specimens were retrieved to perform the immunohistochemistry. Sections 4 μm thin were deparaffined and rehydrated and then subjected to endogenous peroxidase blocking in 1% H2O2 solution in methanol for 15 min. Antigen retrieval was performed by autoclaving the sections at 105°C for 10 min in Dako Target Retrieval Solution (Dako, Glostrup, Denmark). Serum blocking was performed with antibody 10% normal rabbit serum (Nichirei, Tokyo, Japan) for 10 minutes. After H2O2 and serum blocking, the slides were incubated with primary mouse monoclonal anti-CD8 antibody (1:100 dilution; Dako) at room temperature for 30 min. The secondary antibody was biotin-labeled rabbit anti-mouse IgG (1:500; Nichirei, Tokyo, Japan). Detection was performed with a DAB kit (Histofine simple stain kit; Nichirei). The sections were counterstained with hematoxylin.

Immunohistochemical detection of CD8-positive T cells (×400). The arrows indicate positive cells.
Immunohistochemical evaluation. The immunohistochemical evaluation was carried out by two independent pathologists who were blinded to the clinical information. The number of immunoreactive lymphocytes at the invasive margin was counted with a light microscope in a randomly selected field at a magnification of ×400 (Figure 2). The mean of the values obtained in five different areas was used for the data analysis.
Statistical analyses. The significance of the correlations between the TILs and the clinicopathological characteristics was analyzed using the χ2 test, Fisher's exact test, and the t-test. The duration of the survival was calculated according to the Kaplan-Meier method. Differences in the survival curves were assessed using the log-rank test. A multivariate analysis was performed according to the Cox proportional hazard model. The correlations between the density of TILs in the primary tumor evaluated using the H-E-stained sections and the number of CTLs in the primary tumor were examined using the Mann-Whitney test. All of the statistical analyses were conducted using the SPSS software package for Windows (SPSS Japan, Tokyo, Japan). p-Values of <0.05 were considered to indicate statistical significance.
Ethical considerations. This research conformed to the provisions of the Declaration of Helsinki. All patients were informed of the investigational nature of this study and provided their written informed consent. This retrospective study was approved by the ethics committee of Osaka City University (approved No. 926).
Results
Characteristics of the patients. The characteristics of the patients who underwent palliative chemotherapy are listed in Table I. The patient population consisted of 25 males and 32 females, with a median age of 63 years (range=40-83 years). The distribution of metastatic sites was as follows: liver, 44; lung, 16; peritoneum, 16; and distant lymph node, 12. As a first-line chemotherapy, all of the patients underwent combination chemotherapy with oxaliplatin, irinotecan plus 5-fluorouracil/leucovorin, or a prodrug of 5-fluorouracil. All regimens used for the patients in this study were considered to have the same efficacy (18-20). The distribution of the regimen of chemotherapy was as follows: 5-fluorouracil+leucovorin+oxaliplatin (FOLFOX), 35; capecitabine+oxaliplatin (CapeOX), 14; 5-fluorouracil+leucovorin+irinotecan (FOLFIRI), 7; and received S-1+oxaliplatin (SOX), 1. Twenty-six (45.6%) patients underwent chemotherapy combined with molecular-targeted therapy.
Correlations between the density of TILs and the clinicopathological factors. The only significant relationship identified was between the density of TILs and gender (p=0.016) (Table II).
Characteristics of the patients who underwent palliative chemotherapy.
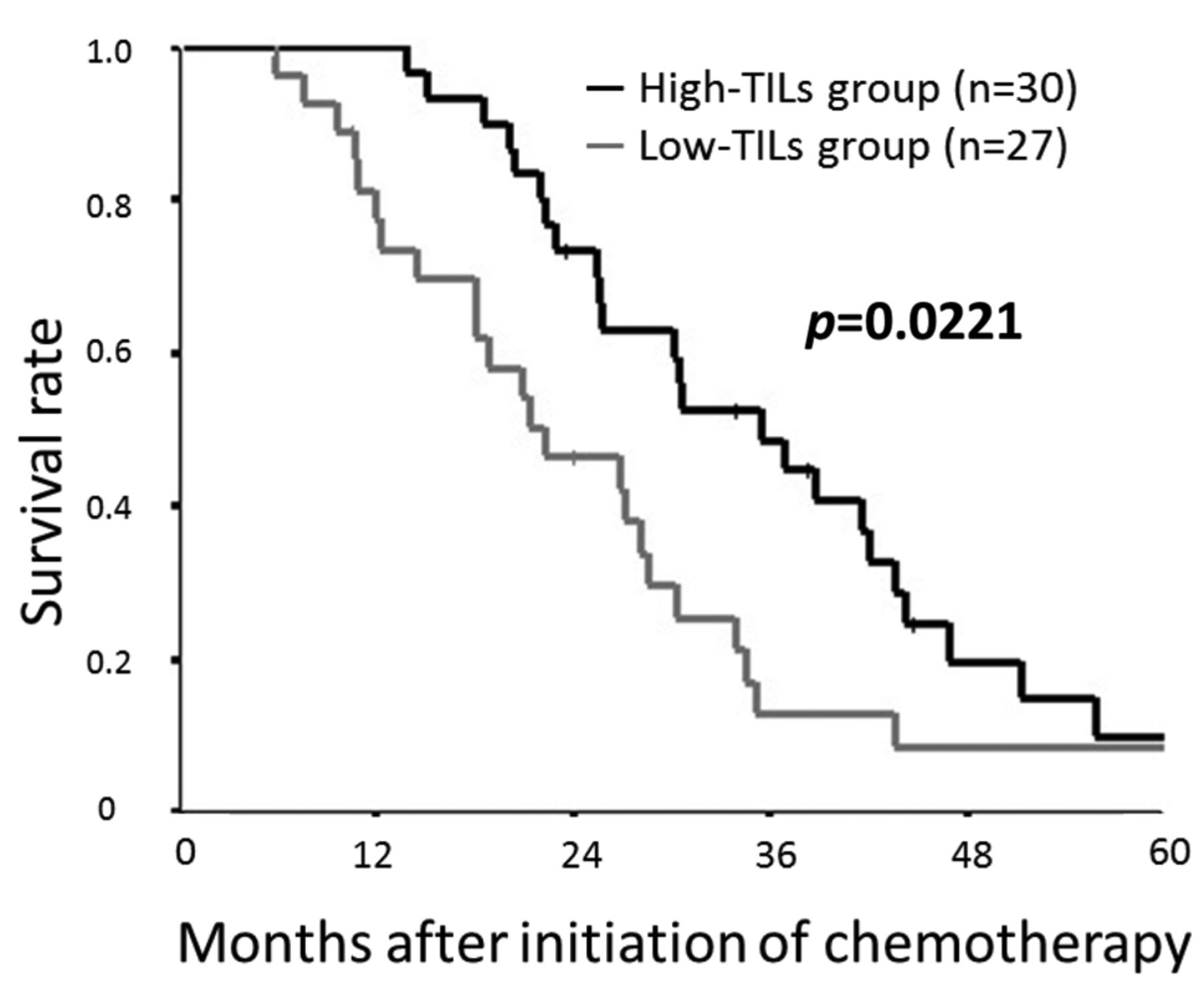
Correlations between the density of TILs in the primary tumor and the chemotherapeutic outcome. The distribution of the chemotherapeutic response with reference to the TILs subgroup is shown in Table III. A high TILs level was associated with a significantly high objective response rate compared to a low TILs level (79.3% vs. 48.1%, p=0.025). The progression-free survival was significantly better in the high-TILs group than in the low-TILs group (median survival time: 10.1 m vs. 7.3 m, p=0.0133) (Figure 3). The overall survival was also significantly better in the high-TILs group than in the low-TILs group (median survival time: 35.5 m vs. 22.4 m, p=0.0221) (Figure 4).
Correlation between the density of TILs evaluated using the H-E-stained sections and the number of CTLs. The number of CTLs in the high-TILs group according to the evaluation using the H-E-stained sections was significantly higher than in the low-TILs group (Figure 5).
Prognostic factors influencing the survival. Clinicopathological variables for prediction of progression-free survival were tested in univariate and multivariate analyses (Table IV). According to the results of a univariate analysis, the progression-free survival showed a significant relationship with the density of TILs (p=0.017) and tended to show a relationship with gender (p=0.070). A multivariate analysis indicated that there were no independent prognostic factors for the progression-free survival.
Correlations between the density of TILs in the primary tumor and clinicopathological factors.
Clinicopathological variables for prediction of overall survival were tested in univariate and multivariate analyses (Table V). According to the results of a univariate analysis, the overall survival showed a significant relationship with the density of TILs (p=0.024) and tended to show a relationship with the number of organs affected by metastases (p=0.062). A multivariate analysis indicated that the density of TILs in the primary tumor (hazard ratio: 0.542; 95% confidence interval: 0.302-0.972; p=0.040) was an independent prognostic factor for the overall survival.

The Kaplan–Meier survival curves for the progression-free survival. The progression-free survival was significantly better in the high-TILs group than in the low-TILs group (p=0.0133).

The Kaplan–Meier survival curves for the overall survival. The overall survival was significantly better in the high-TILs group than in the low-TILs group (p=0.0221).
Discussion
In this study, we investigated the prognostic significance of TILs in the primary tumor as a marker for predicting the chemotherapeutic outcome in patients with stage IV CRC who underwent palliative chemotherapy using the method proposed by the International TILs Working Group. To our knowledge, this is the first study to assess the significance of TILs as a marker for predicting the chemotherapeutic effectiveness in patients with stage IV CRC.
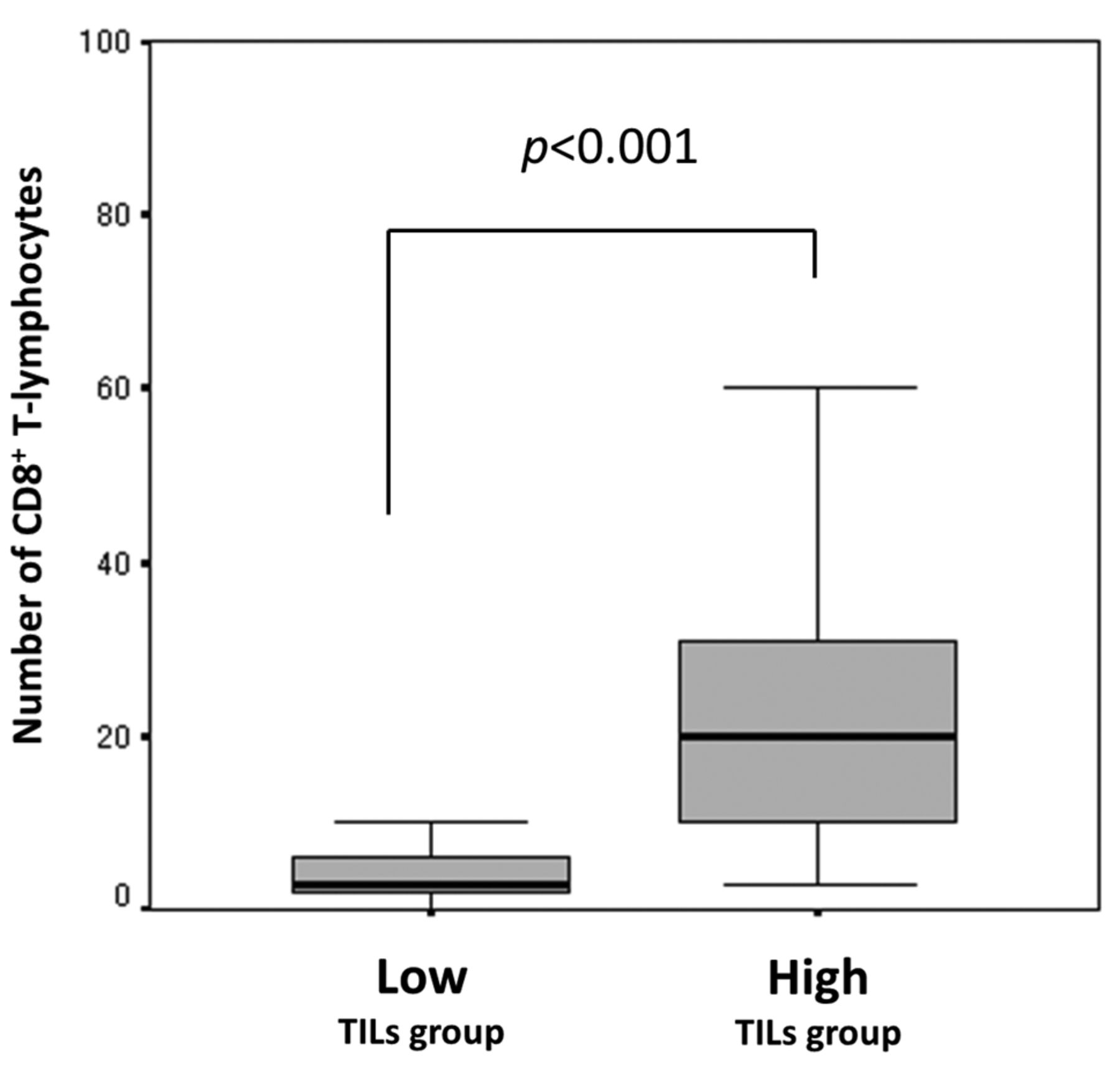
The correlation between the density of TILs evaluated using the H-E-stained sections and the number of cytotoxic T-lymphocytes (CTLs) in the primary tumor. The number of CTLs in the high-TILs group was significantly higher than in the low-TILs group (p<0.001).
Distribution of the chemotherapeutic response with reference to the TILs subgroup.
Increasing evidence suggests that the balance between the immune cells of the host and the cancer cells plays an important role in tumor progression (21, 22). The presence of TILs within the tumor microenvironment is considered to reflect the immune response of the host to the tumor (23). Because immune cells eliminate the tumor cells and suppress the tumor growth, patients with a strong lymphocyte reaction, i.e. those with high-TILs, have a better prognosis than those with a weaker reaction. Furthermore, the density of TILs has been reported to correlate with the efficacy of chemotherapy and radiotherapy (9, 10, 24). Although some problems remain, such as the unification of methods for the evaluation and elucidation of the functions for each subset, TILs are now receiving a great deal of attention as potential new biomarkers.
Prognostic factors influencing the progression-free survival.
Prognostic factors influencing the overall survival.
In this study, the density of TILs in the primary tumor was revealed to correlate with the chemotherapeutic outcome. Several studies have suggested possible mechanical linkage between anti-cancer immunity of the host and the effectiveness of chemotherapy. The destruction of tumor cells by chemotherapy causes the release of tumor antigens. This may trigger an immune response directed against the tumor cells, which will be particularly strong in patients whose immune status was activated before treatment (9). Given that chemotherapy enhances the anti-tumor immunity via the activation of CTLs, conventional cytotoxic chemotherapy serves as a form of immunotherapy (25). As described above, a greater immune reaction to cancer before treatment is associated with greater efficacy of chemotherapy. Therefore, the pretreatment density of TILs is thought to be a useful prognostic marker for chemotherapeutic effectiveness.
Although TILs have been recognized to have an important role in anticancer immunity (16, 26), the method of evaluating TILs has differed among previous reports, and there is no established methodology for evaluating TILs (11-15). The methodology using the H-E-stained sections proposed by the International TILs Working Group is simple and easy because it does not involve immunohistochemistry. However, in the evaluation using the H-E-stained sections, the subset of the lymphocytes is not considered, although the International TILs Working Group emphasized that the evaluation was possible regardless of the subset of the lymphocytes (16). In the current study, the density of TILs evaluated by H-E-stained sections was found to be associated with the number of tumor-infiltrating CTLs, which play a key role in anti-cancer immunity (27). This result indicates that the methodology using H-E-stained sections is based on an immunological mechanism.
Although the density of TILs in the primary tumor was found to be associated with the chemotherapeutic outcome in this study, the correlation between the density of TILs in the metastatic tumor, which is a target for chemotherapy, and the chemotherapeutic outcome is unclear. A previous report described a strong correlation between the density of TILs in the primary tumor and that in metastatic tumors (28). Therefore, the evaluation of TILs in the primary tumor may serve as a substitution for the evaluation of TILs in metastatic tumors.
Several limitations associated with the present study warrant mentioning. First, we evaluated a relatively small number of patients, and the study design was retrospective. Second, potential heterogeneity of TILs may remain, although we used a full assessment of the average density of TILs in order to minimize the margin of the measurement error due to heterogeneity. A large prospective study should, therefore, be performed to confirm our findings.
Conclusion
The measurement of TILs in the primary tumor using the method proposed by the International TILs Working Group can be used as a prognostic marker of the clinical effectiveness of palliative chemotherapy in patients with stage IV CRC.
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no competing interests.
- Received July 20, 2017.
- Revision received October 17, 2017.
- Accepted October 18, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Tumour immune microenvironment biomarkers predicting cytotoxic chemotherapy efficacy in colorectal cancer
- Evaluating reproducibility of AI algorithms in digital pathology with DAPPER
- Tumor-infiltrating Immune Cells in H&E-stained Sections of Colorectal Cancer Tissue as a Reasonable Immunological Biomarker