


Abstract
Background/Aim: The JAMAR-Dynamometer and the Martin-Vigorimeter are frequently used tools in a hand surgeon's daily routine. This survey is primarily concerned with the establishment of valid conversion factors for measured values of both instruments, as well as the investigation of influence of anatomical characteristics and age and sex on maximal measured grip strength. Patients and Methods: We registered anamnestic data and specific anatomical conditions in 339 patients, maximal grip strength was measured using all notches of both instruments. Results: We found moderate to very high correlation comparing all 28 settings in both instruments. The influence of the hand's anatomy on the grip strength was greater using the JAMAR-Dynamometer than it was using the Martin-Vigorimeter. Conclusion: The high reproducibility allowed us to calculate multiplying factors for the conversion of measured data for all settings of both tools. Therefore, the amount of data for meta-analyses relating to hand surgical issues can be significantly increased.
Grip strength measurements are routinely used in clinical settings. They are an indicator for the efficacy of hand surgical therapies and serve as outcome control (1-4). The most commonly used instruments for measuring grip strength are the JAMAR-Dynamometer and the Martin-Vigorimeter. The former is a hydraulic instrument measuring the isometric strength in kilograms, the latter measures the force of compression in kilo pascal by means of a compressible rubber ball (5, 6). Numerous studies have investigated the reliability of both instruments in different populations (2, 4, 7-11). However, to the best of our knowledge, only a few studies directly compare these two instruments. Sipers et al. compared the applicability and the test-retest reliability of both instruments in geriatric patients and found no significant difference in test-retest reliability. Handgrip strength showed a strong correlation between the first and second measurement in both instruments (1). Molenaar et al. examined reliability and accuracy of both instruments in 104 children under 12. Their results indicate that both instruments are reliable for measuring grip strength within this population. The Lode dynamometer (equivalent to JAMAR-Dynamometer) detected small differences in grip strength more accurately (12). Desrosiers et al. analyzed a population of 360 randomly selected healthy, elderly patients and while they found a good correlation between the respective results of both instruments, they did not determine a conversion factor (13).
To recap, most scientific studies have only used one of the two methods. Moreover, measuring has mostly been limited to one level or one size of balloon, respectively (4, 14-16). Using just one level per instrument to determine grip strength impairs optimal comparability of the results given that a couple of studies have found a correlation between morphological parameters of the hand and lower arm and maximum grip strength, depending on the level of the instrument or the size of the balloon used (17-19). Until recently, it has been impossible to compare results of studies that use just one of the two instruments in any setting with results of studies using the other. Therefore, the primary aim of this study was to determine conversion factors for the values of both instruments for all levels or sizes and to enable the comparison of the results of numerous studies, and thereby enlarging the amount of data available for meta-analyses within the field of hand surgery. We also aimed to show anatomical influences on the results in order to make informed recommendations about which settings to use on which instrument regarding specific hand sizes, and to determine the influence of age and sex on the results.
Patients and Methods
This survey was authorised by the local ethics committee (Nr. 1498-2012). Each patient in our study group signed a written consent form.
Patients. We randomly included all patients between the ages of 14-90 years with healthy and symptom free hands, who were treated in the Department of Traumatology over a period of three months. We excluded patients with injuries, deformities, degenerative or inflammatory functional limitations of the upper extremities as well as patients with dementia to minimise any bias that could influence correlation. Since the study design contained many subgroup analyses and focused on a correlation between the two machines, we desisted from conducting a power analysis and chose a sample size following the study of Desrosiers et al. (13).
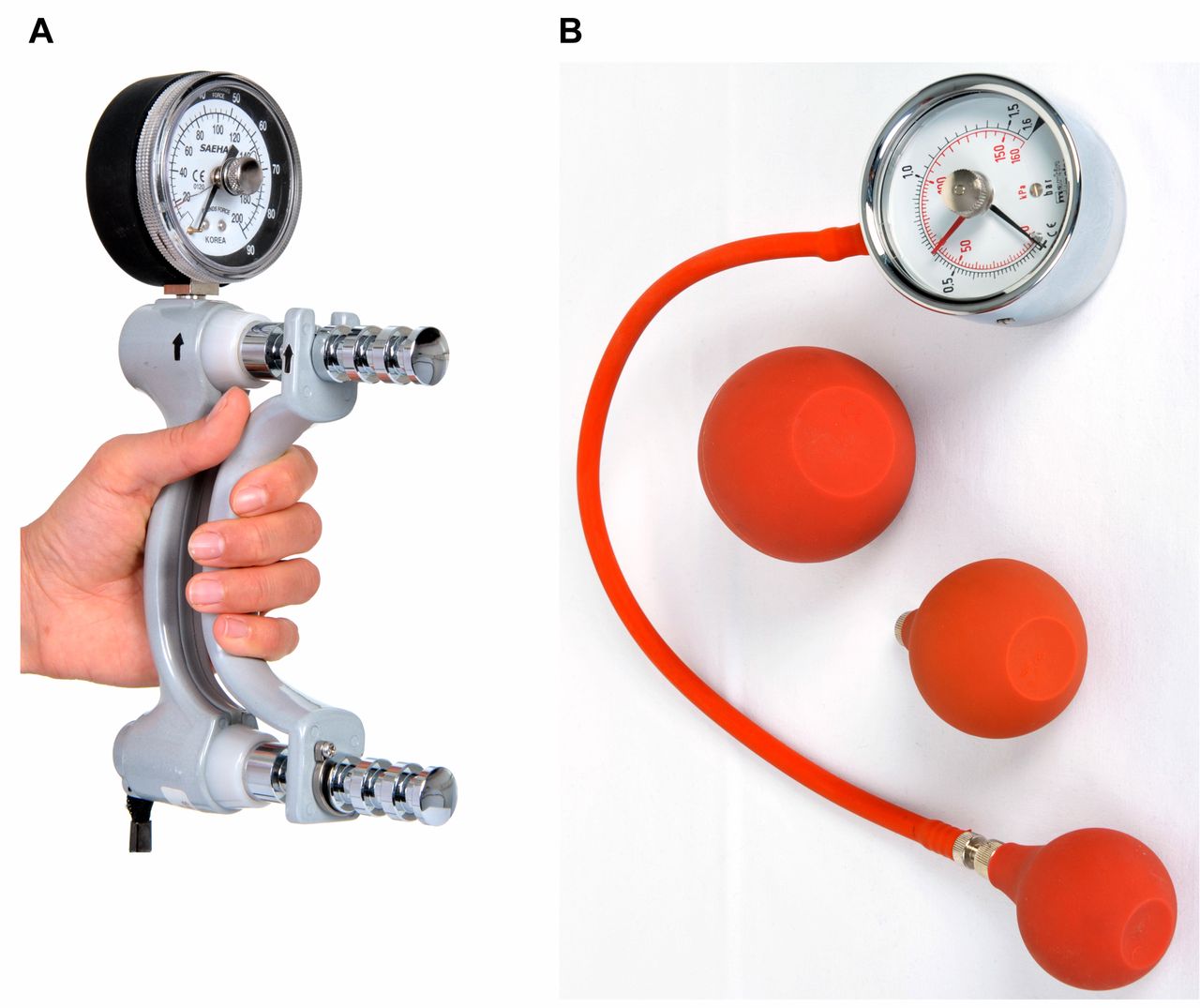
Grip strength analysis. We registered anamnestic data that could influence our measurements such as: age, sex, handedness and current occupation. Patients were divided into five different age categories (<20/20-40/41-60/61-80/>80 years). Specific anatomical conditions were measured in all patients: circumference of the forearm 15 cm distal of the radial epicondyle, length of the palm (from the palmar fold of the wrist to the fold of the metacarpophalangeal joint of the middle finger), length of the hand (from the palmar fold of the wrist to the tip of the middle finger), the hand's circumference without the thumb and the width of the palm (from the ulnar margin of the metacarpophalangeal joint of the thumb to the ulnar border of the palm). The measurements of the grip strength were determined by means of the JAMAR-Dynamometer (J A Preston Corporation, New York, USA) using all five notches and by means of the Martin-Balloon-Vigorimeter (Firma Gebrüder Martin, Tuttlingen, Germany) using all three ball sizes (Figure 1). All of the instruments were checked for damages, inspected for proper function and calibrated. Each patient was shown the correct handling and positioning of the instruments: Patients were asked to sit straight, with the upper arm in a neutral position and a 90° flexion of the elbow. The forearm was held in neutral position and the wrist at a 0 to 30° extension. The instrument was held freely: neither the hand nor the forearm was allowed to rest on a surface. To minimise signs of fatigue we included resting periods after each trial. Additionally, to avoid systematic errors we randomised the sequence in which we carried out the trials. Sequence one: JAMAR notch 1 – Martin balloon 2 – JAMAR notch 2 – Martin balloon 3 – JAMAR notch 3 – Martin balloon 5 – JAMAR notch 4 – JAMAR notch 5. Sequence two: Martin balloon 2 – JAMAR notch 1 – Martin balloon 3 – JAMAR notch 2 – JAMAR notch 3 – Martin balloon 5 – JAMAR notch 4 – JAMAR notch 5. Afterwards, we randomised the side to be tested first. All measurements were repeated three times on each side.
Statistical analysis. The data were processed with Excel 2011 (Microsoft Corporation, Redmond, USA) and GraphPad Prism 6.0 (GraphPad Software, Inc., La Jolla, USA). We calculated the median values and the interquartile range (25th – 75th percentile) as data proved to be non-parametric. We calculated the conversion factors by forming the quotients of the measured values for all notches and determined mean values and standard deviations. The influence of anatomical characteristics on the grip strength was determined using a Spearman rank correlation to minimise the effect of outlying data and non-parametric distribution. The level of significance was placed at p<0.05. The interpretation of the correlation coefficient followed Mukaka (20), who distinguished low (r<0.5), moderate (r<0.7), high (r<0.9) and very high (r>0.9) correlation.
Results
Subject characteristics. Three hundred and thirty-nine patients (132 women/207 men) aged between 14-88 years (mean 49±18.4 years) were included. Our study group primarily comprised age groups 41-60 years (n=129), 61-80 years (n=103) and 20-40 years (n=85). 91.45% of all patients were right-handed, 6.19% were left-handed and 2.36% had no dominant hand (Table I).
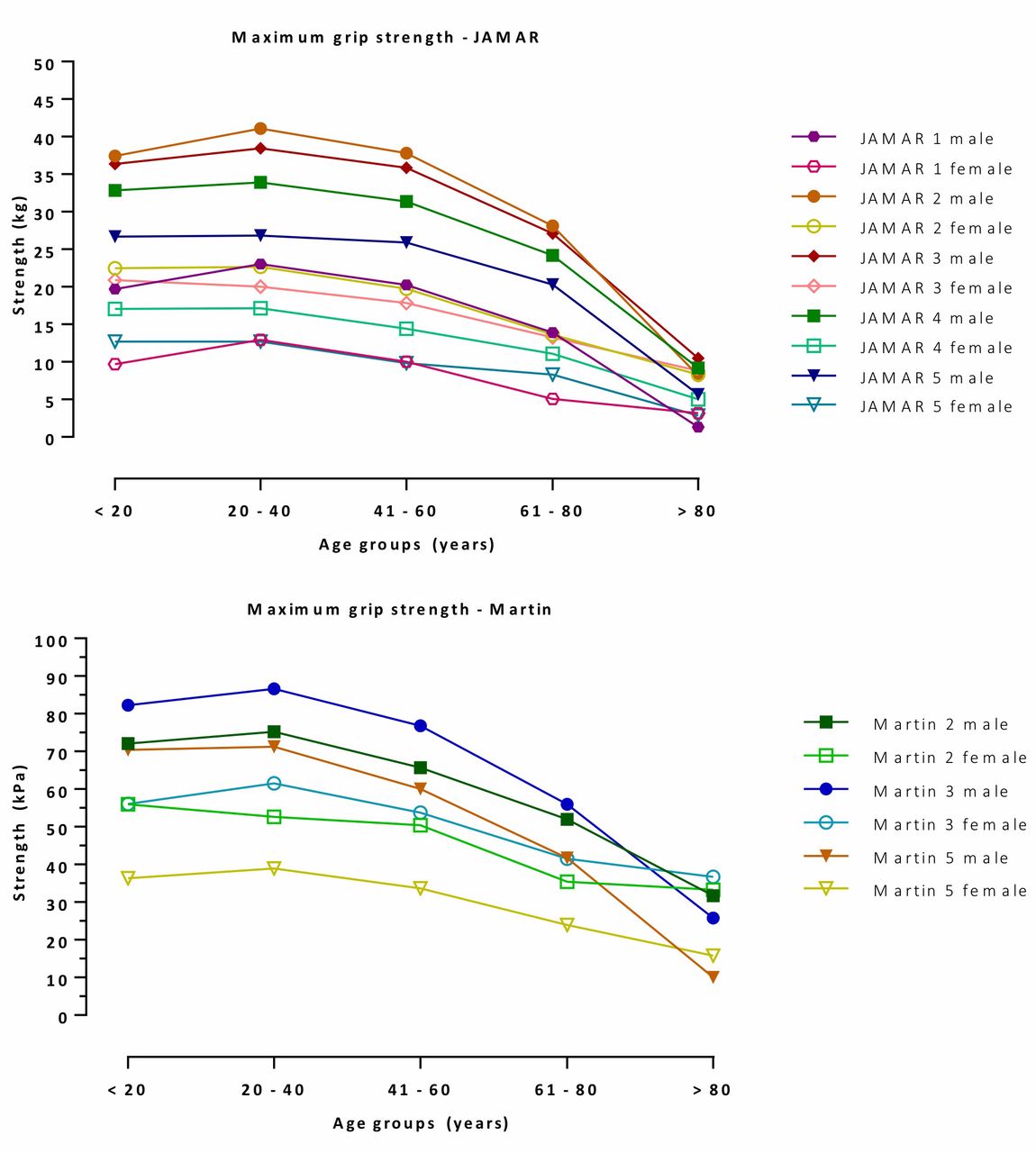
Grip strength results. The median maximum grip strength in men was 79% greater than in women using the JAMAR-Dynamometer, and it was 38% greater using the Martin-Vigorimeter (19.7 kg women/35.3 kg men and 53.3 kPa women/73.3 kPa men). Overall, we found very high correlations between the measured grip strength of the dominant hand using notch 2 of the JAMAR-Dynamometer and balloon 5 of the Martin-Vigorimeter (r=0.86), as well as between notch 3 of the JAMAR-Dynamometer and balloon 5 of the Martin-Vigorimeter (r=0.86). Within the measurements of one instrument, we found a very high correlation between measured grip strength using notch 3 and 4 of the JAMAR-Dynamometers (r=0.97), as well as between balloon size 3 and 5 of the Martin-Vigorimeter (r=0.92) (Table II). We calculated multiplying factors for the correlation of all measured data for all settings on both instruments (Table III). With regards to the anatomical characteristics we found a moderate correlation between the maximum grip strength and the hand's circumference without the thumb of the dominant hand using the JAMAR-Dynamometer (r=0.64). We also found a moderate correlation (r=0.65) between the width of the palm and the circumference of the forearm to the maximal grip strength measured with the JAMAR-Dynamometer. Both, the length of the palm and the length of the dominant hand had a moderate correlation with the maximal grip strength using the JAMAR-Dynamometer (r=0.52 and 0.55, respectively). Using the Martin-Vigorimeter, the maximal grip strength showed only a low correlation to the anatomical characteristics (r<0.5). The highest correlation was found with the circumference of the forearm (r=0.49) (Figure 2). At least 64% of patients reached the maximal grip strength when using notch 2 of the JAMAR-Dynamometer irrespective of the sex. At notch 3 of the JAMAR-Dynamometer, 31% of male and 16% of female patients achieved the highest results. Using the Martin-Vigorimeter, the highest results were achieved with balloon size 3 notwithstanding the sex (Figure 3). Overall, the age group 20-40 years showed the highest measured results for the grip strength regardless of the notch/balloon size (Figure 3).
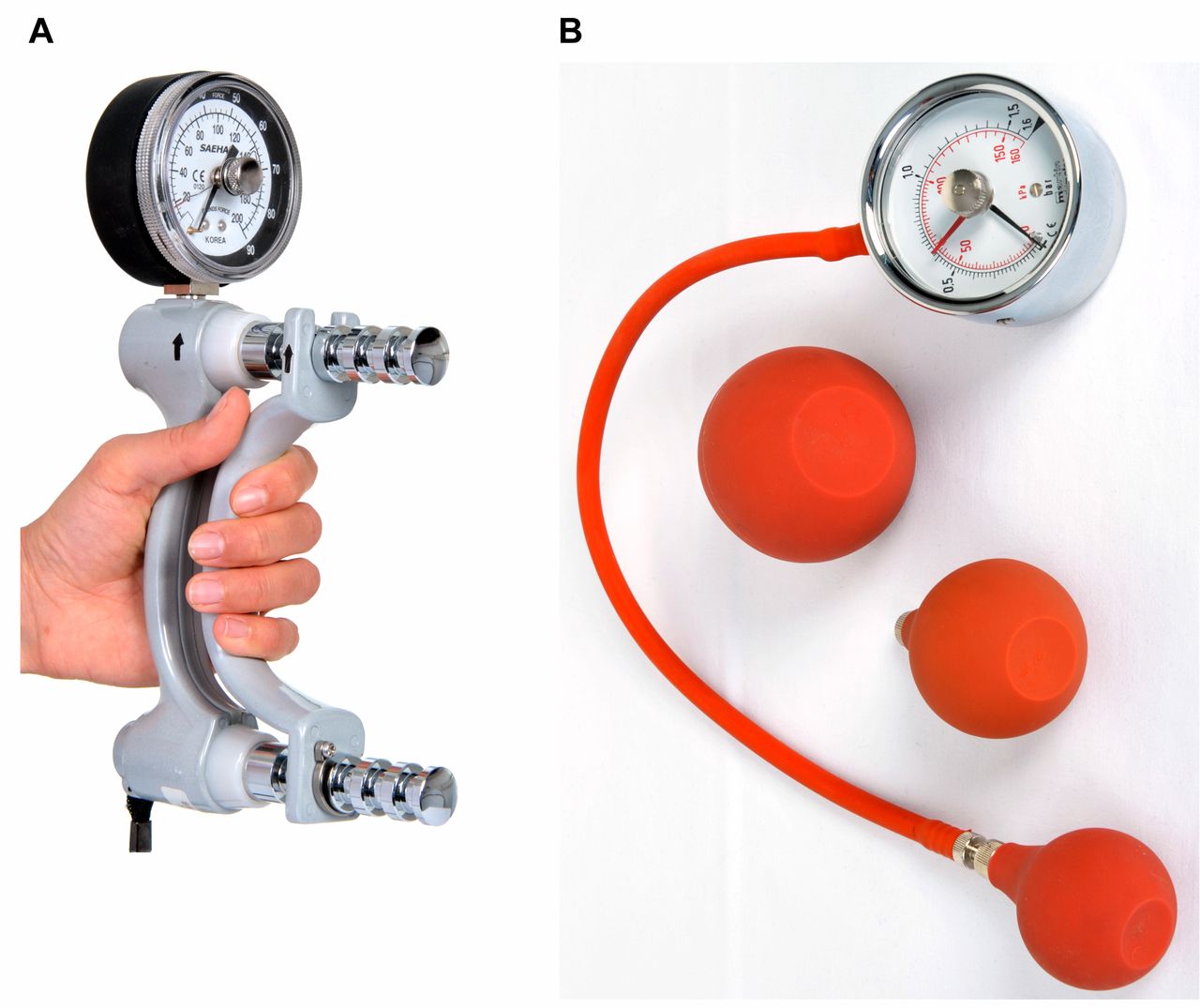
A. The JAMAR-Dynamometer is a hydraulic instrument measuring the isometric strength in kilogram. B. The Martin-Vigorimeter measures the force of compression in kilo pascal by means of a compressible rubber ball.
Discussion
In this study, we examined 339 randomly selected patients with healthy hands to determine the correlations between all notches and balloon sizes for the Martin-Vigorimeter and the JAMAR-Dynamometer. All 28 comparisons of the notches and balloon sizes showed moderate to very strong correlations. Within the instrument groups, the strongest correlations were found between the measured results of the JAMAR-Dynamometer notch 3 and notch 4 and Martin-Vigorimeter balloon size 3 and 5. Matching the results of both groups, the highest correlations were found between notches 2 and 3 of the JAMAR-Dynamometer and balloon size 5 of the Martin-Vigorimeter. The lowest correlation was found between notch 5 of the JAMAR-Dynamometer and balloon size 2 of the Martin-Vigorimeter. These results can be explained by the large distance of approximately 90 mm between the handles of the JAMAR-Dynamometers at notch 5. We believe that patients with small hands were unable to fully clasp the instrument and therefore could not make use of their full strength while the small balloon of the Martin-Vigorimeter is easily compressed irrespective of hand sizes. These results correspond to the findings of Espana-Romero et al., who showed a very strong correlation between the grip strength and the setting of the JAMAR-Dynamometer and patient hand size (21). Ruiz et al. (22) also recommended determining the position of the notch of the JAMAR-Dynamometer according to a patient's hand size. Therefore, it must be assumed that the correlation coefficient of the individual positional settings of each instrument would be smaller if there was a high anatomical variance of the patients' hands sizes in the study group.
Demographic characteristics, Handedness and profession in all study participants.
Correlation coefficients JAMAR-Martin.
Regarding the weak correlations, the anatomical variance of our patients' study group allowed no prediction of the maximal grip strength using the Martin-Vigorimeter. The results of Desrosiers et al. (13) and Li et al. (17) confirm our observation that the correlation between maximal grip strength and anatomical parameters is lower when using the Martin-Vigorimeter than when using the JAMAR-Dynamometer. In this study, the results of the maximal grip strength that were measured using the JAMAR-Dynamometer showed the highest correlation with the width of the palm and the circumference of the forearm on the dominant side. At this point, our results are consistent with the current literature (13, 19, 23, 24). However, regarding the length of the hand, the literature presents inconsistent results. Our results show moderate correlation between grip strength and length of the hand and correspond to Li et al. (17). In contrast to these findings, the results of Boadella et al. (25) and Trampisch et al. (26) displayed either no correlation or merely a positive trend between grip strength and length of the hands/fingers and width of the hand and recommended standardised instrument settings. Ruiz-Ruiz et al. (27) found a correlation between hand size and strength in the female study group, but not in the male one. The inconsistent and partly contradictory results of the literature and our findings suggest that the influence of the anatomic variables on the grip strength is not significant and that anatomical factors will only influence the results when patients with small hands use settings with a large distance between the handles. We therefore concluded that anatomical factors alone should not determine the instrument's setting. Our results showed the highest grip strength for the JAMAR-Dynamometer on notch 2 and 3 and balloon size 3 for the Martin-Vigorimeter. These findings, as well as the strong correlation between the instruments indicate that measurements should be carried out on notch 2 and 3 with the JAMAR-Dynamometer and on balloon size 3 on the Martin-Vigorimeter. Settings for patients with either very large or very small hands should be adapted accordingly.
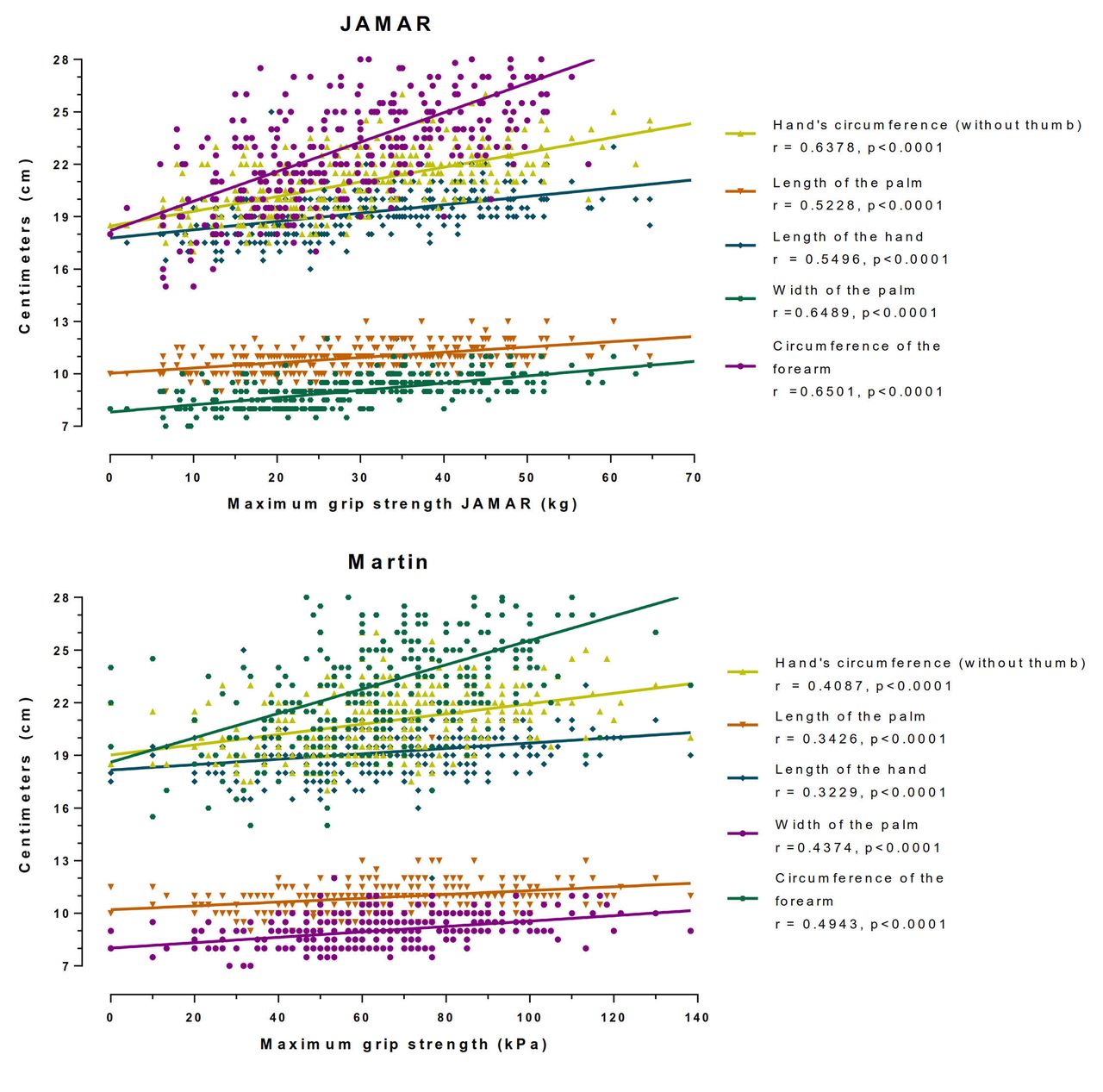
Graph shows the correlation between the influence of anatomical characteristics of the patient's forearm and hand with the maximum grip strength measured with the JAMAR-Dynamometer and the Martin-Vigorimeter.
Conversion table JAMAR-Martin.

Graph shows the correlation between the influence of the patient's age and sex with the maximum grip strength measured with the JAMAR-Dynamometer and the Martin-Vigorimeter.
Similar to our findings of maximum grip strength for female and male patients in the age group of 20-40 years, Mathiowetz et al. (15) observed a peak of grip strength between the ages of 25 and 39 years, which slowly decreased thereafter. In the present study, the lowest strength was found in the group of patients >80 years, regardless of the sex of a patient. Tyler et al. (28) noticed that patients with weak hands had problems or were unable to use the JAMAR-Dynamometer properly. Our study supports these findings since much older patients had difficulties handling this instrument due to its rigidity and weight. This could indicate that false low results could occur in older or sicker patients and that the correlation with the results of the Martin-Vigorimeter, which is easier to handle, decreases as a result.
Limitations to our study include the following: The evaluated instruments are primarily used on patients that have been deliberately excluded from this trial. We tried to minimize any measurement errors concerning the conversion factors by eliminating unpredictable results in an unhealthy population. The majority of the comparisons conducted in our study are already available in the current literature but, to our knowledge, this is the first study that correlates the two instruments in all available settings and determines conversion factors for the results of the JAMAR-Dynamometer and the Martin-Vigorimeter. The conversion factors will allow us to compare studies with similar populations that use either one instrument in any setting and therefore add more data for eventual meta-analyses for hand surgical questions.
Acknowledgements
The Authors would like to express their deepest gratitude to Koko Kwisda, Jasjote Grewal and Courtney Metz for their revision and translation of the manuscript. The Authors also wish to thank Jan Beneke for his assistance in the statistical analysis.
Footnotes
This article is freely accessible online.
- Received July 25, 2017.
- Revision received August 9, 2017.
- Accepted August 10, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.