


Abstract
Background: We assessed the change in LUTS after prostate brachytherapy to reveal factors for prolonged urination disorder. Materials and Methods: Four hundred and four patients received prostate brachytherapy at our institution and were followed-up for at least 2 years. We evaluated the correlation of mean IPSS changes and clinical factors. Using multivariate analysis, we also evaluated clinical factors with potential to delay IPSS resolution. Results: In cases with prostate volume more than 30 cm3, radiation dose to 90% of prostate volume (D90) more than 160 Gy, and radiation dose to 30% of the urethral volume (UD30) more than 240 Gy, mean IPSS levels were significantly higher, even 30 months after treatment. On multivariate analysis, baseline IPSS more than 8 points and D90 more than 160 Gy were significant predictors for delayed IPSS resolution. Conclusion: Our data suggest that higher baseline IPSS and higher D90 were predictors for prolonged urination disorder.
The use of permanent radioactive implants to treat clinically-localized prostate cancer patients has been increasing rapidly all over the world for the past 20 years. In Japan, prostate brachytherapy (PBT) became an insurance adaptation in 2003 and has become one of the most common treatments for clinically-localized prostate cancer (1) National Comprehensive Cancer Network Clinical Practice Guidelines recommend PBT not only for low- and intermediate-risk groups but also for high- and very high-risk groups in combination with androgen deprivation therapy (ADT) and external beam radiotherapy (EBRT) (2). It is reported that high-dose radiotherapy using low-dose-rate PBT in combination with EBRT and short-term ADT has shown excellent outcomes in high-risk and very high-risk cancer (3, 4).
PBT can cause some adverse events. Lower urinary tract symptoms (LUTS) are major complications for men following PBT (5-10). For some patients, International Prostate Symptom Scores (IPSS) quickly return to pre-treatment levels, while others require more time. We assessed the change in LUTS after brachytherapy to reveal predictive factors for prolonged urination disorder.
To our knowledge, no study has analyzed predictive factors using time-dependent multivariate analysis.
Patients and Methods
Patient characteristics. Between July 2004 and December 2014, 404 patients received low-dose-rate PBT at Tokushima University Hospital in Japan and were followed-up for at least 2 years. Clinical characteristics of patients are shown in Table I.
Brachytherapy procedure. Pre-planning involved analyzing the prostate in detail by transrectal ultrasonography about 4 weeks before brachytherapy to calculate prostate volume (PV) and plan seed implantation. Brachytherapy was performed using ultrasound-guided, transperineal prostate implantation planned using Interplant software (CMS, St. Louis, MO, USA). For post-planning, about 4 weeks after seed implantation, computed tomography, and radiography of the chest kidneys, ureters, and bladder were performed to calculate the radiation dose to 90% of the prostate volume (D90) and to evaluate seed migration in all patients.
Follow-up. All patients were asked to return at 1, 3, and 6 months after seed implantation, and every 6 months thereafter. Patient IPSS was assessed at each visit. PV was measured every 12 months using ultrasonography. Follow-up time was calculated from treatment completion to the last available date of follow-up or date of death. Median duration of follow-up after seed implantation was 77.5 months (range=26-126 months), and no patient was lost during follow-up.
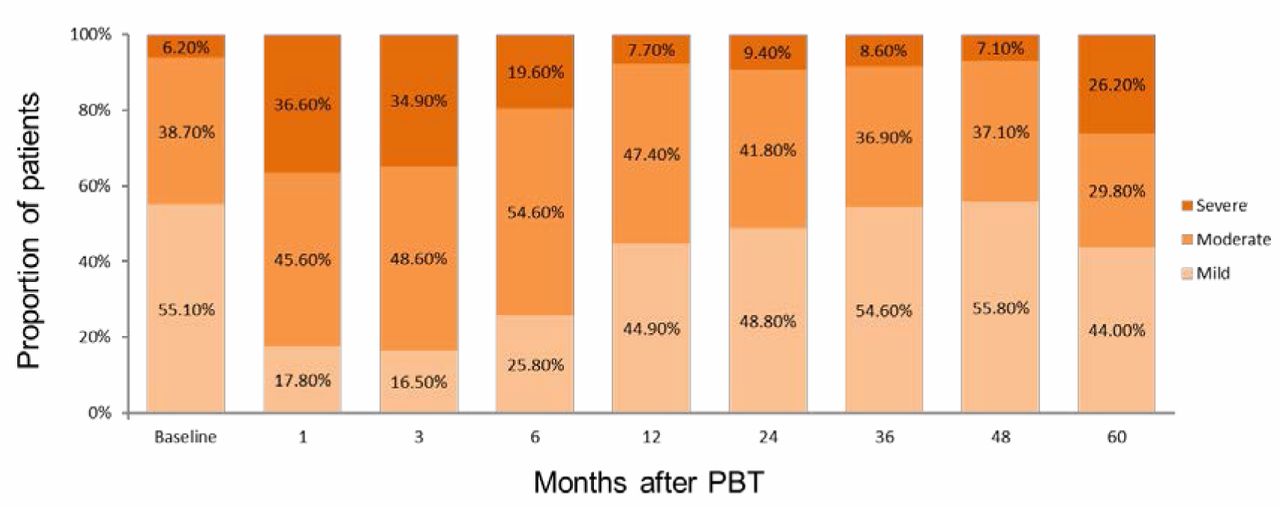
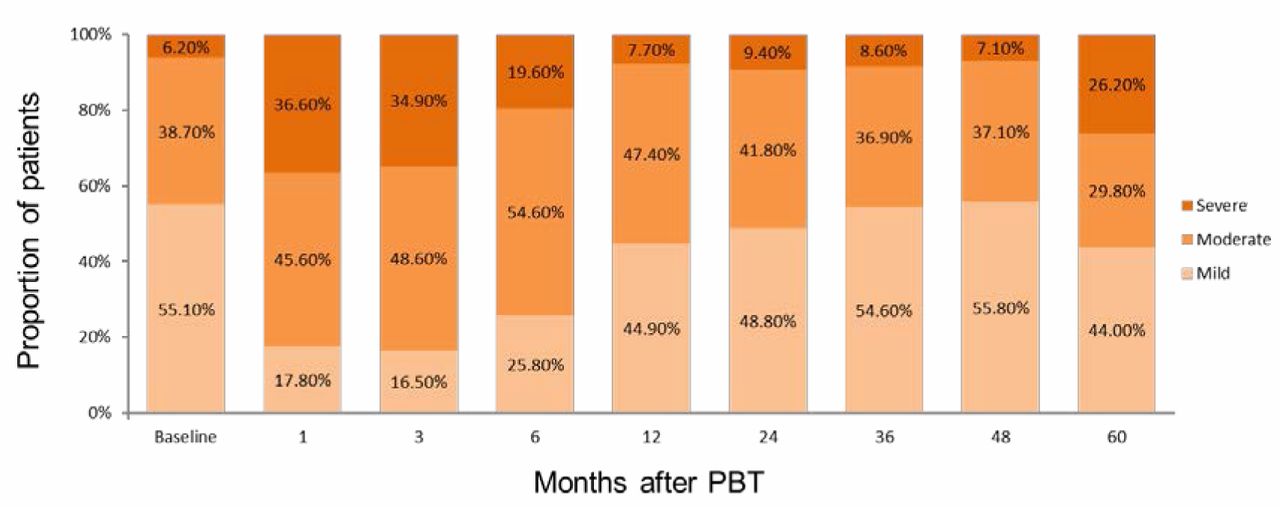
Symptomatic severity classified by total International Prostate Symptom Score resolution rate over time after prostate brachytherapy (PBT).
Patient characteristics.
Statistical analysis. All analyses were performed using IBM SPSS Statistics Version 20 (IBM Corp., Armonk, NY, USA). We evaluated the correlation of mean IPSS changes and clinical factors regarding PV, ADT, D90, and radiation dose to 30% of the urethral volume (UD30). Mean IPSS differences for both groups at each follow-up visit were examined using Student t-test with values of p<0.05 taken as significant.
Using univariate and multivariate logistic-regression analyses, we also evaluated clinical factors with the potential to delay IPSS resolution to baseline score, including age, pretreatment IPSS, clinical stage, ADT, PV, D90, and UD30, to predict prolonged urination disorders after PBT.
IPSS resolution was defined as a return of the total IPSS to within 2 points of the baseline score (11-13).
International Prostate Symptom Score (IPSS) resolution rate over time after prostate brachytherapy (PBT).
Results
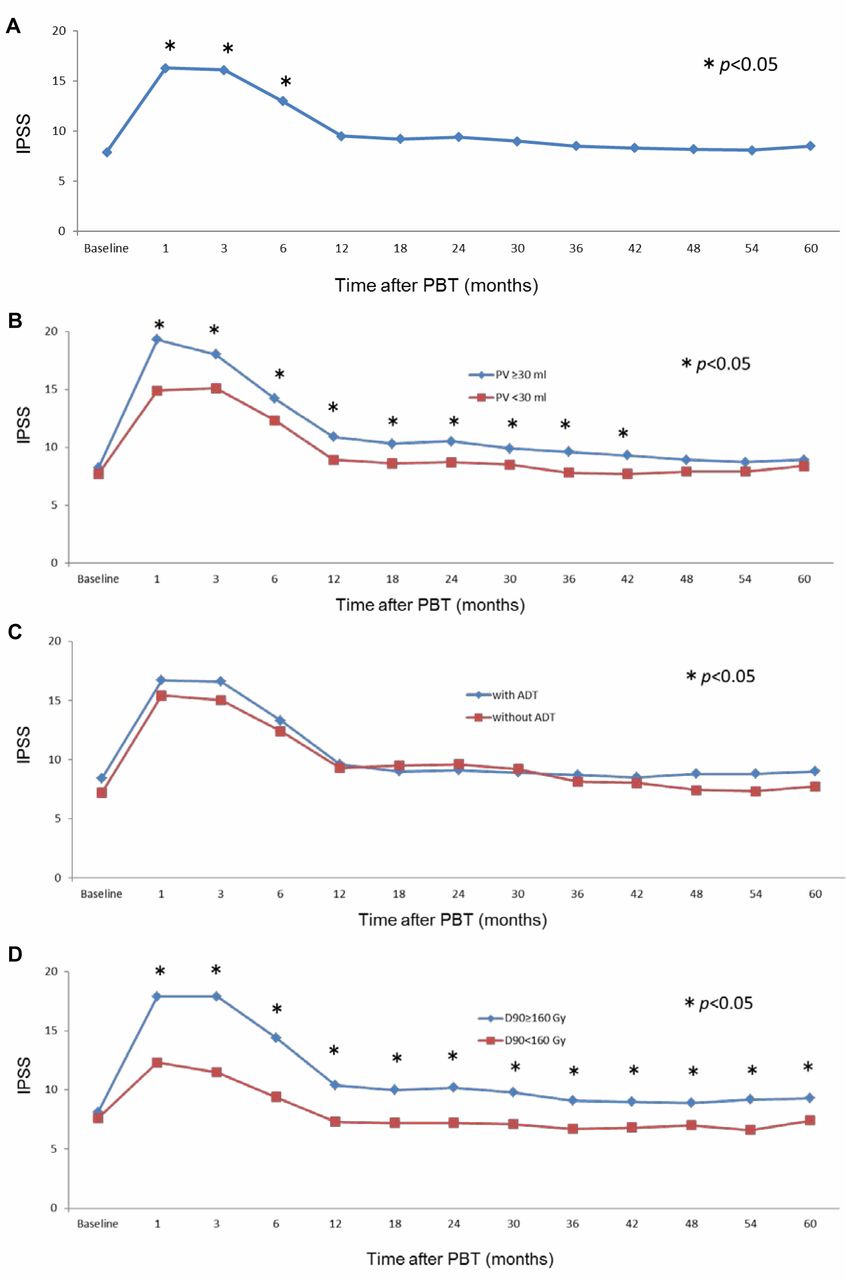
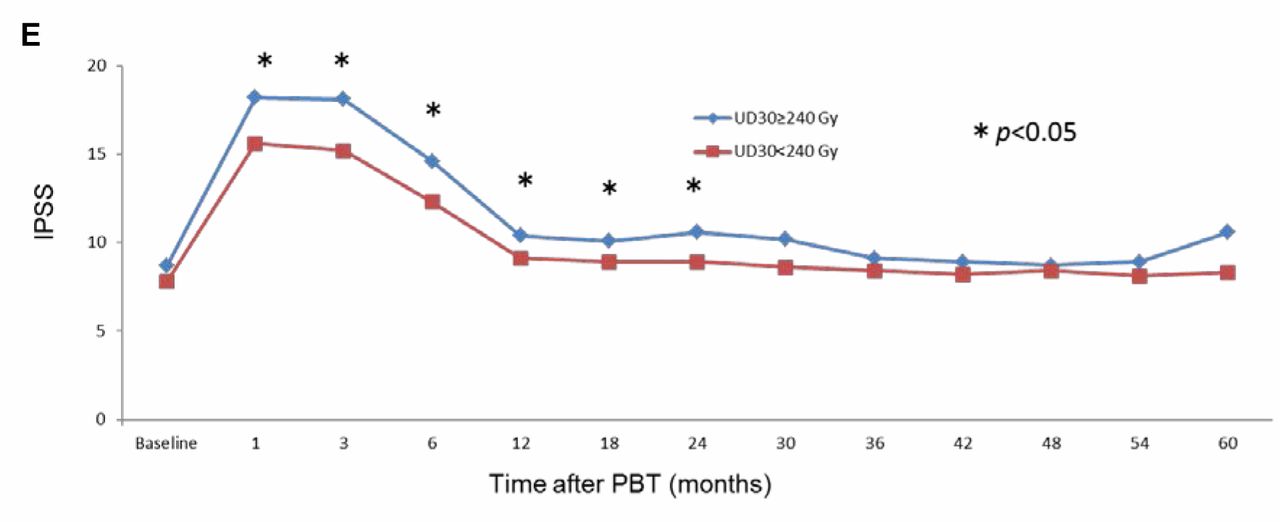
Of IPSS severity categories, the mild-severity group comprised of more than half of all patients before seed implantation, however, this proportion dropped to less than 20% by 1 month after implantation (Figure 1). Symptomatic severity was worst at 1 month after treatment, and recovered to almost pre-treatment levels after more than 3 years. The mean pre-implant IPSS was 7.9, with the greatest mean score of 16.3 at 1 month after seed implantation (Figure 2A). At 3, 6, 12, 24, 36, 48 and 60 months, the mean IPSS had decreased to 16.1, 13.0, 9.5, 9.4, 8.5, 8.2 and 8.5, respectively. In cases with PV of more than 30 cm3, D90 more than 160 Gy, and UD30 more than 240 Gy, the mean IPSS levels were significantly higher, even 30 months after treatment, while combination with ADT had no impact on IPSS change (Figure 2B-E).
Clinical factors with potential to delay International Prostate Symptom Score (IPSS) resolution after prostate brachytherapy (PBT) were evaluated using univariate and multivariate logistic-regression analysis.
Box plot of PV change showed significant decrease from baseline 1 year after treatment (Figure 3).
IPSS resolution was highest at 60 months after seed implantation and was achieved in 70.1% (171/244) (Table II).
On univariate logistic-regression analysis, baseline IPSS more than 8 points was a significant predictor for prolonged IPSS resolution after seed implantation from 6 to 60 months, and D90 more than 160 Gy was significant from 6 to 36 months. PV more than 30 ml was significant predictor from 36 to 48 months, and UD30 more than 240 Gy was significant from 6 to 12 months (Table III). On multivariate logistic-regression analysis, baseline IPSS more than 8 points was a significant predictor for prolonged IPSS resolution after PBT from 12 to 60 months, and D90 more than 160 Gy was significant from 6 to 36 months (Table III).
IPSS resolution rate improved with time course after seed implantation, and was 70.1% at 60 months (Table II).
Discussion
Patients who choose PBT are attracted to the minimally-invasive nature of the procedure, favorable potency preservation rates, shorter hospitalization time, and lower risk of urinary incontinence. However, LUTS are one major complication for men following PBT. Most men will experience at least some change in their voiding pattern after PBT. This suggests permanent changes in urinary function result from radiation implantation (5). Seed implantation may result in chronic inflammation, which has been reported to be significantly associated with higher IPSS and larger prostate volume (14). In a multi-institutional cohort study, it was reported that grade 2 acute urinary toxicities developed within 3 months in 7.36%, while grade 2 late urinary toxicities developed in 5.75% (1). A study investigating LUTS after low-dose rate PBT reported IPSS to be greatest from 1 to 3 months after seed implantation and gradually return to almost baseline levels after 12 to 24 months (10, 15, 16). Stone et al. reported that patients with fewer than 3 years follow-up had a mean increase in IPSS of 2.7 points, whereas those with more than 3 years' follow-up had mean increase of 1.7-points (5). In our study, the mean post-implant IPSS peaked 1 month after seed implantation and gradually returned to the baseline score after 1 year. We found on average an 8.4-point increase in IPSS over baseline at 1 month after treatment. Patients had a mean IPSS increase of 1.6 points from baseline at 1-year follow-up, 1.5 points at 2-year follow-up, 0.6 points at 3-year follow-up, 0.2 points at 4-year follow-up, and 0.4 points at 5-year follow-up. We found mean IPSS increased beyond the 4-year follow-up. The influence of aging can cause symptoms to worsen past the 4-year follow-up point.


Mean International Prostate Symptom Score (IPSS) resolution rate over time after prostate brachytherapy (PBT) (A), and according to prostate volume (PV) (B), androgen deprivation therapy (ADT) (C), radiation dose to 90% of the prostate volume (D90) (D) and radiation dose to 30% of the urethral volume (UD30) (E). A: *The mean IPSS was significantly higher from 1 to 6 months after PBT in comparison that at with baseline. B-E: *Significant difference between the two groups at the indicated time point.
Although the realization of urination pattern deterioration after seed implantation is unavoidable, patient quality of life will be good if urination quickly recovers to pre-implant levels. Mira et al. reported that in their 712-patient cohort, the IPSS resolution rate was 40% at 12 months, 70% at 24 months, 80% at 36 months, and 90% at 72 months after treatment (11). In our study, the IPSS in 61.1% of patients recovered to baseline level at 12 months, 64.2% at 24 months, 66.9% at 36 months, and 70.1% at 60 months. Compared to Mira et al., our study cohort included a higher median baseline IPSS (6 vs. 5) and higher median age (67 vs. 65.5 years). As a result, IPSS resolution rate after 24 months was lower, with a final resolution rate difference of more than 10% between the cohorts.
Teishima et al. reported that the presence of LUTS, including IPSS more than 8 points before implantation, does not prolong urinary morbidity after permanent PBT (15). However, in their report, IPSS resolution was not defined precisely, while we precisely defined IPSS resolution as a return of the total IPSS to within 2 points of baseline score (11-13). In this study, the presence of pre-implant IPSS higher than 8 points significantly delayed IPSS resolution from 12 to 60 months after seed implantation and D90 more than 160 Gy significantly delayed IPSS resolution from 6 to 36 months, suggesting that higher baseline IPSS might have an impact on inhibiting recovery from urination disorder for a long period of time, while higher D90 might inhibit recovery from urination disorder within a relatively short period of time.

Box plot of prostate volume (PV) change after prostate brachytherapy (PBT) relative to baseline. *Significantly different from baseline value.
Keyes et al. reported that higher D90 is associated with higher late urinary toxicity and slowed IPSS resolution time (8). Tanaka et al. reported that on multivariate analysis, not D90 but UD30 was a predictive parameter for IPSS recovery at 12 months after seed implantation (17). In our study, higher D90 significantly delayed IPSS resolution from 6 to 36 months after seed implantation on both univariate and multivariate analyses, while higher UD30 delayed IPSS resolution from 6 to 12 months only on univariate analysis. This may suggest that higher UD30 has an earlier impact on prolonged IPSS resolution compared with higher D90.
Alpha 1-adrenoceptor antagonists are well known to provide relief from LUTS after seed implantation (18-20). LUTS resulting from PBT improve continuously after 3 months, so it is recommended to use alpha 1-adrenoceptor antagonists at an early stage of post treatment (17). We use alpha 1-adrenoceptor antagonists for 1 month after treatment and check IPSS at the first outpatient appointment. We stop using alpha 1-adrenoceptor blocker if patients are satisfied with their urination pattern at 1 month, otherwise we continue it in accordance with the patient's condition.
To remove uneasiness after brachytherapy, patients must be given sufficient information regarding predictable progression of urinary symptoms. This study provides important and useful information for selecting the optimal treatment for patients with clinically-localized prostate cancer.
Footnotes
This article is freely accessible online.
- Received April 20, 2017.
- Revision received June 5, 2017.
- Accepted June 6, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}