


Abstract
Background/Aim: Patients affected by liver cirrhosis are at high risk for developing hepatocellular carcinoma (HCC). The aim of this study was to evaluate the feasibility of PIVKA-II (protein induced by vitamin K absence or antagonist-II) alone or in combination with α-1 fetoprotein (AFP), as a screening marker for development of HCC. Materials and Methods: A case-control study was conducted in 2 hospital wards in Naples. All anti-HCV-positive patients affected by HCC were considered as cases, while consecutive anti-HCV-positive patients without HCC were considered as controls. Results: Overall, 160 patients were enrolled, 56 cases and 104 controls. At the set cut-off of 36 mAU/ml, PIVKA-II was more sensitive (78.6% vs. 60%), but less specific than AFP at the set cut-off of 12 ng/ml (66.3% vs. 77.2%). The negative predictive value of PIVKA in combination with AFP was 93.2%. Conclusion: PIVKA II, when combined with AFP, may be considered as a screening test for HCC due to its high negative predictive value.
Hepatitis C virus (HCV) infection affects more than 185 million people worldwide and is estimated to cause about 350,000 deaths every year (1).
HCV can cause both acute and chronic hepatitis. In 55-85% of cases, acute HCV infection becomes chronic. Chronic hepatitis C infection progresses towards cirrhosis in 15-30% of cases in about 20 years and about 2-4% of patients with cirrhosis develop hepatocellular carcinoma (HCC) each year (1, 2). HCC is the fifth most common cancer in males and the seventh in females, causing up to 700,000 deaths each year (3). Because of the high risk of developing HCC, per authoritative guidelines, patients with cirrhosis should undergo periodic screening with abdominal ultrasound to detect HCC at an early stage.
Both the American Association for the Study of Liver Diseases (AASLD), and the European Association for the Study of the Liver/European Organization for Research and Treatment of Cancer (EASL-EORTC) produced guidelines on the diagnosis, management and surveillance protocols of HCC (2, 4). Both guidelines, with due differences, agree on screening of at-risk patients at least every six months with abdominal ultrasonography. There is no consensus on the use of serum biomarkers.
The most commonly utilized biomarker in clinical practice for HCC is α-1 fetoprotein (AFP). AFP may be used as a diagnostic and prognostic marker. Serum AFP levels also correlate with tumor size, tumor doubling time and post-treatment relapse (2, 5-8). However, it is not recommended for routine screening because it lacks specificity. AFP may be elevated in other malignancies (e.g. gastric, embryonic cancer, intrahepatic cholangiocarcinoma), as well as in many benign conditions, both hepatic (e.g. cirrhosis, necrosis, acute hepatitis), and extrahepatic (e.g. pneumonia). Finally, AFP lacks sensitivity; serum AFP levels are high in only 40-60% of HCC cases and only 10-20% of early HCC (5). For these reasons, more sensitive and specific HCC markers are required.
PIVKA-II (protein induced by vitamin K absence or antagonist II), also known as des-gamma-carboxyprothrombin (DCP), is an immature form of prothrombin without any coagulative function. It is synthesized in the presence of acquired defects of precursor carboxylation found in patients with HCC (5, 10). PIVKA-II may have a role in HCC progression by acting as an autologous growth factor (11-13). Moreover, high serum levels of PIVKA-II are associated with HCC size, microvascular invasion, metastatic dissemination and HCC relapse after liver transplantation and/or HCC nodule ablation (8, 14-17). PIVKA-II is a specific marker for HCC, it is poorly related to AFP and exhibits higher sensitivity and specificity than AFP in diagnosing HCC. PIVKA II is not elevated in benign hepatic diseases (e.g. cirrhosis, necrosis) (10, 18), while it is elevated in HCC at early stage as well as in HCC nodules of all sizes (8, 18, 19).
For these reasons, some authors, and especially Japanese guidelines on HCC management proposed the use of PIVKA-II for routine follow-up in patients with high risk for developing HCC (5, 20), as well as a prognostic biomarker before surgery to predict microvascular invasion, relapse and overall poor prognosis (14-17). In detail, Japanese guidelines have suggested to consider as a diagnostic marker of HCC high elevation of tumor markers, namely AFP ≥200 ng/ml and PIVKA-II ≥40 mAU/ml.
However, data on its performance as a diagnostic marker are still incomplete. The aims of the study were to evaluate: i) the diagnostic accuracy of PIVKA-II in the diagnosis of HCC in HCV-related liver cirrhosis; ii) the comparative diagnostic accuracy of PIVKA-II and AFP in the diagnosis of HCC; iii) the diagnostic accuracy of a novel marker derived from the association of AFP and PIVKA-II.
Materials and Methods
We conducted a case-control study performed in 2 hospital wards, the Infectious Disease Unit of the ‘A.O.U. Federico II” of Naples and the Hepatobiliary Surgery Unit of the “Fondazione G. Pascale” National Cancer Institute.
Study population. All patients aged 18 and above admitted to the participating hospital wards that met the following inclusion criteria were enrolled in the study;
Cases: proven HCV infection (positive anti-HCV and detectable serum HCV-RNA) plus radiological, histological or cytological evidence of hepatocellular carcinoma as assessed in AASLD hepatocellular carcinoma guidelines (2). Exclusion criteria were consent refusal, previous pharmacological or local HCC therapy and anticoagulant therapy.
Controls: infection with HCV (positive anti-HCV and detectable serum HCV-RNA), negative history for HCC and absence of nodular hepatic lesions under abdominal ultrasonography.
All patients underwent history-taking, physical examination, routine laboratory examinations, serological testing for HCV and HBV infections and abdominal imaging either by abdominal ultrasonography, contrast-enhanced CT- scanning or contrast-enhanced MRI according to the clinical judgment. Cases were also categorized according to CLIP (The Cancer of the Liver Italian Program) staging score. Blood samples for AFP and PIVKA-II assays were also collected from all the enrolled patients, regardless if they belonged in the case or in the control group. PIVKA-II assay was performed using Lumipulse® G1200 (Fujirebio Inc., Malvern, PA, USA), an enzyme-linked immunoassay based on chemiluminescence principles (CLEIA – chemiluminescent enzyme immunoassay). Tests were performed at the Laboratory Medicine unit of the “Fondazione G. Pascale” National Cancer Institute.
Ethical aspects. The study was conducted in accordance with Good Clinical Practices and was regulated by the latest revision of the Helsinki Declaration. Data handling was in accordance with the Italian law on privacy. All enrolled patients were requested to sign a written consent after being informed about the study aims. The patients were managed per best routine clinical practice. The study was first approved by the Ethical Committee of the coordinating clinical unit Ethical Committee of University of Naples “Federico II”.
Statistical analysis. All patients enrolled were included in the analyses. Continuous variables were reported as mean±SD (standard deviation) or as median and interquartile range (IQR) when appropriate. Between-group comparisons were made using T-student test and Mann-Whitney U-test when appropriate. Categorical variables were reported as percentages. Among-group comparisons were made using the chi-squared test or the Fisher's exact test when appropriate. The cut-off for statistical significance was set at 5% in two-tailed test. The diagnostic accuracy was assessed using ROC curve. Correlation of selected variables was evaluated using Pearson's correlation coefficient.
We categorized PIVKA-II and AFP serum levels to obtain a sensitivity rate of 80% and we also performed a composite score between PIVKA-II (categorized to 36 mAU/ml) and AFP (categorized to 12 ng/mL) and we tested diagnostic accuracy of this score in the diagnosis of HCC.
Statistical analysis was performed using software package SPSS 18.0: PASW Statistic (SPSS, Inc, Chicago, IL, USA).
Results
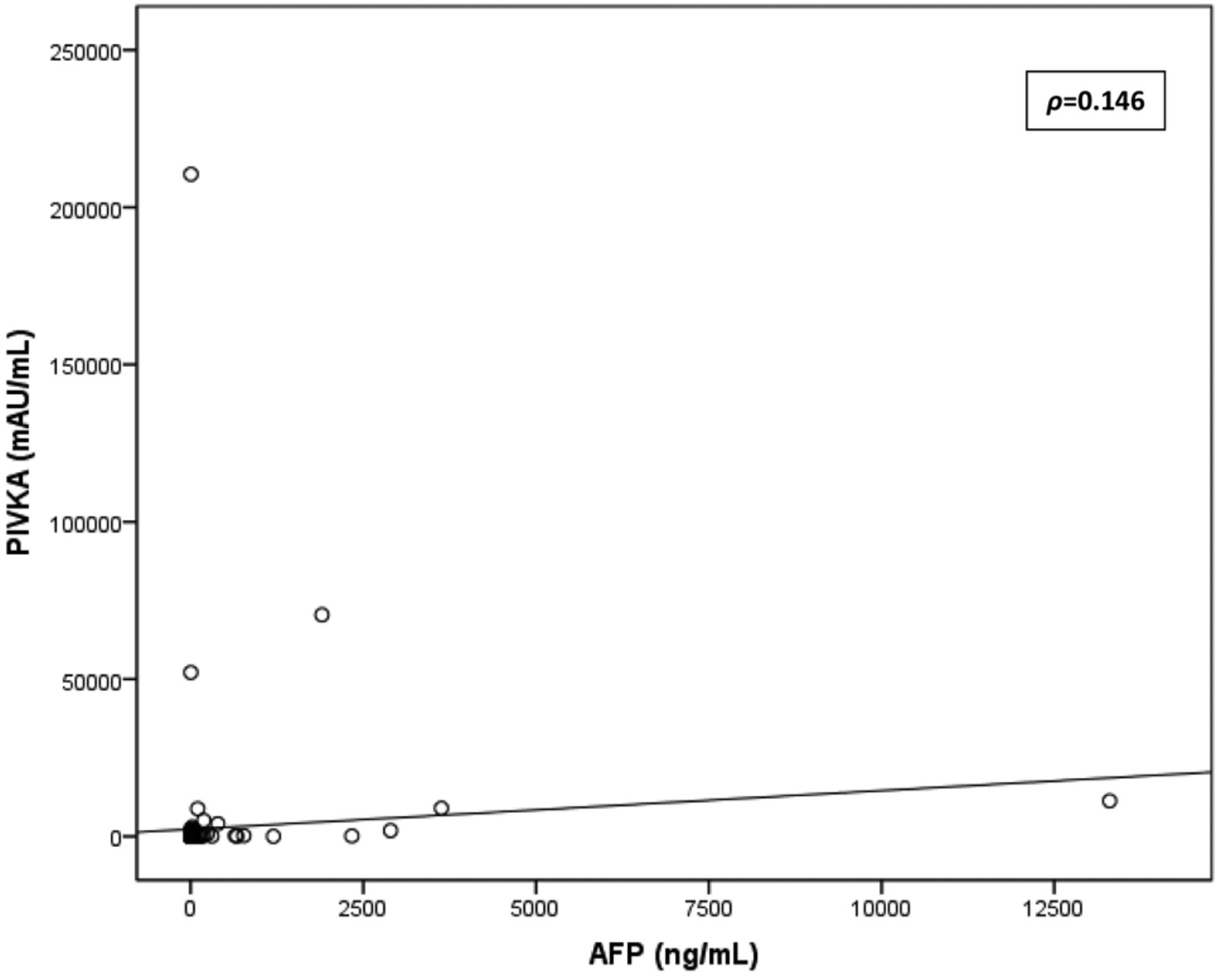
Baseline characteristics of the 160 enrolled patients are shown in Table I. Significant differences in socio-demographic variables between cases and controls were observed for gender (p=0.004) and age (p=0.002). No differences were observed in clinical variables between the two groups. For laboratory variables, significant differences were observed in glucose levels (p<0.001), albumin levels (p=0.003), platelet count (p=0.038) and serum HCV-RNA (p=0.014)). Both serum AFP (17.3 vs. 5.1 ng/ml, p<0.001) and serum PIVKA-II concentrations (146.5 vs. 27.5, p<0.001) were higher in the case group (Table I). Serum levels of AFP and PIVKA-II were not correlated (ρ=0.146) (Figure 1).
The performance of both PIVKA-II and AFP in the diagnosis of HCC were plotted on a ROC curve (Figure 2) showing similar areas under curve for both markers; specifically, areas under curve (AUC) for PIVKA-II (cut-off:36 mAU/ml) and AFP (cut-off:12 ng/ml) were 0.788 (95%CI=0.707-0.868) and 0.756 (95%CI=0.676-0.836) respectively. At the set cut-off value of 36 mAU/ml, PIVKA-II was more sensitive (78.6% vs. 60%) but less specific than AFP at the set cut-off value of 12 ng/ml (66.3% vs. 77.2%). The negative predictive value of PIVKA in combination with AFP was 93.2% and it was higher when compared both to AFP (75.9%) and PIVKA alone (85.2%) (Table II).
Characteristics of patients (n=160).
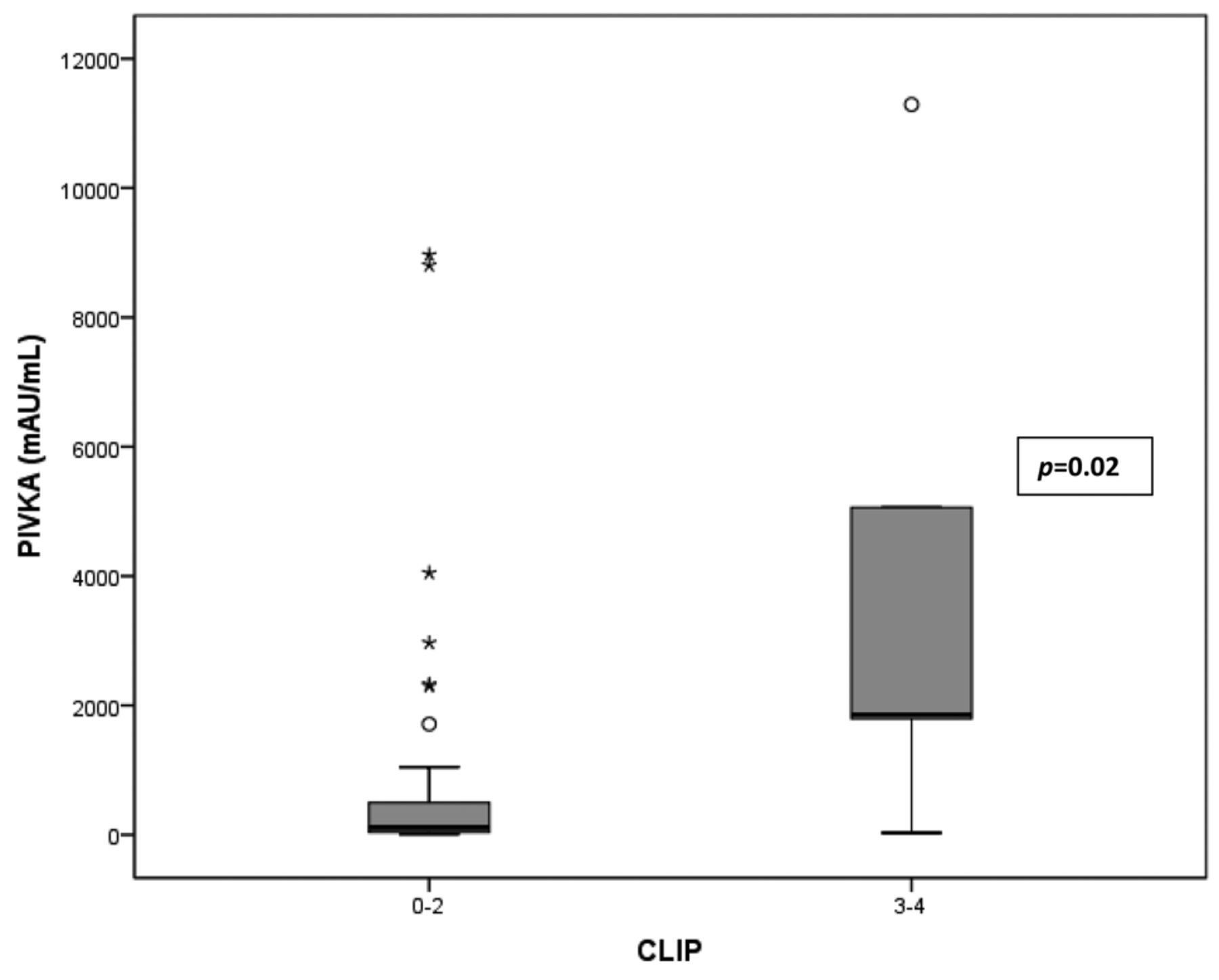
All cases of HCC (n=56) had liver cirrhosis. HCC was graded using CLIP staging score. Most cases (39/56 patients, 70%) had a CLIP score of 0-1. Patients with CLIP score of 2 or 3-4 were 18% (10/56) and 12% (7/56), respectively. Subgroup analysis of cases showed that patients with CLIP score 3-4 (vs. 0-2) had significantly higher serum levels of PIVKA-II (159 vs. 3.458 mAU/ml, p=0.02) (Figure 3). Similarly, patients with CLIP score 3-4 (vs. 0-2) had significantly higher serum levels of AFP (244 vs. 14.6 ng/mL, p=0.023) (Figure 4).
Discussion
HCC is the sixth most common cancer in the world and the third most common cause of cancer-related death. The prognosis of HCC worsens as CLIP score increases (21). In our study, patients with HCC were older and more often males than patients without HCC. Male predominance may be explained by greater exposure to toxins, HCV prevalence and hepatocyte androgenic stimulation (22). We also observed higher blood glucose levels and lower levels of albumin and platelets; these results are in accordance with the role of metabolic syndrome and insulin-resistance as risk factors for HCC (6, 23).

Linear correlation between AFP and PIVKA-II. PIVKA: prothrombin induce\d by vitamin K absence-II; AFP: α-fetoprotein; HCC: hepatocellular carcinoma.
Patients with cirrhosis, especially if due to HBV or HCV, are at high risk for developing HCC and, therefore, undergo active surveillance with six-monthly upper abdominal ultrasound. However, researches for the identification of an effective serum marker for screening of HCC are currently ongoing. AFP is widely used for this purpose, even though it is not recommended by neither EASL nor AASLD guidelines because of its low sensitivity and specificity (22). AFP is elevated in only 40-60% of cases of HCC. Sensitivity is even lower in early HCC cases, with serum elevation of AFP in only 10-20% of cases. Moreover, as a non-specific inflammation and regeneration marker, it may also be elevated in liver diseases (e.g. liver cirrhosis and hepatic necrosis), as well as in some extra-hepatic conditions such as pneumonia and embryonal tumors (9).

Receiver operating characteristics (ROC) curve comparing specificity and sensibility of PIVKA-II and AFP in detecting hepatocellular carcinoma in patients affected by HCV chronic liver disease. PIVKA: prothrombin induced by vitamin K absence-II; AFP: α-Fetoprotein; HCC: hepatocellular carcinoma.
Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of AFP, PIVKA-II and the combination of both in detecting HCC.

Box plot showing PIVKA-II levels according to CLIP stage. Patients were divided in two groups: the one who have a CLIP stage of 0-2 and the others who have a CLIP stage of 3-4. PIVKA-II: prothrombin induced by vitamin K absence-II: CLIP score (The Cancer of the Liver Italian Program score).
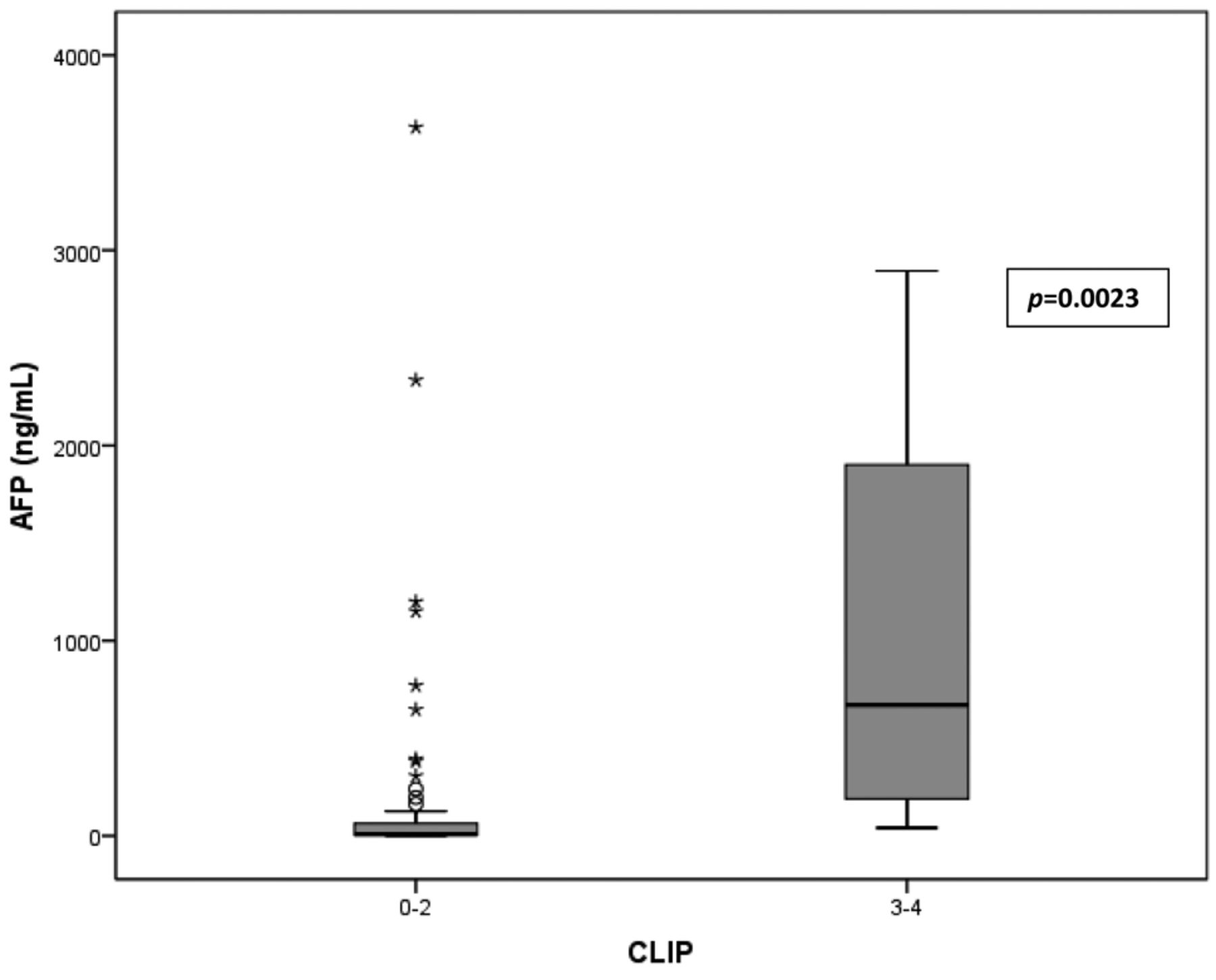
Box plot showing AFP levels according to CLIP stage. Patients were divided in two groups: the one who have a CLIP stage of 0-2 and the others who have a CLIP stage of 3-4. AAFP: α–fetoprotein; CLIP score (The Cancer of the Liver Italian Program score).
In our study, we showed that higher serum concentrations of both PIVKA-II and AFP, were significantly-related to diagnosis of HCC. This is in accordance with other authors, who showed the production of PIVKA-II by HCC and its role as an autologous growth, invasive and pro-angiogenetic factor (11-13) as well as its absence in non-neoplastic hepatic diseases (10).
Similarly to other authors (24), we did not observe any correlation between PIVKA-II and AFP serum levels. This allowed us to evaluate the combined performance of both markers in the diagnosis of HCC, as suggested by already available evidence (19, 24). When cut-off values of 36 mAU/ml for PIVKA-II and 12 ng/ml for AFP were selected, we showed that PIVKA-II, had a higher sensitivity but a lower specificity than AFP. Combining both markers further increased overall sensitivity and negative predictive value at the expense of specificity (51.4%). These results slightly differ from a recent French study in which the authors showed that PIVKA-II had a better performance than AFP for early HCC diagnosis with a sensitivity of 77% (vs. 61%), a specificity of 82% (vs. 50%), a positive predictive value (PPV) of 76% (vs. 51%) and a negative predictive value (NPV) of 83% (vs. 62%), at a cut-off values of 42 mAU/ml for PIVKA-II and 5.5 ng/ml for AFP(25).
In our cohort, both markers showed moderate diagnostic accuracy for HCC. Accuracy of PIVKA-II appeared to be slightly superior to AFP albeit without statistical significance. The serum concentrations of both markers increased at higher values of CLIP score.
In conclusion, PIVKA-II did not appear to be superior to AFP in screening for HCC in our cohort of patients. These markers appeared to perform best at cut-off values of 36 mAU/ml for PIVKA-II and 12 ng/mL for AFP. Nevertheless, the combination of PIVKA-II and AFP at the above mentioned cut-offs, may be considered as a screening test for HCC due to its high negative predictive value.
Further studies are needed to confirm our results in larger cohorts, especially in patients affected by liver cirrhosis of different etiologies.
Footnotes
This article is freely accessible online.
- Received May 5, 2017.
- Revision received May 17, 2017.
- Accepted May 18, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Novel Online Calculator Based on Serum Biomarkers to Detect Hepatocellular Carcinoma among Patients with Hepatitis B
- Prognostic Factors for Post-recurrent Survival in Hepatocellular Carcinoma After Curative Resection
- Severe Vitamin D Deficiency Increases Mortality Among Patients With Liver Cirrhosis Regardless of the Presence of HCC
- CYP3A4 Gene Is a Novel Biomarker for Predicting a Poor Prognosis in Hepatocellular Carcinoma