


Abstract
Background/Aim: In colon surgery, the anastomotic method is generally selected by surgeon's preferences or by local conditions. In this study, we retrospectively analyzed anastomotic complications to assess safe methods of anastomosis in colonic resection. Patients and Methods: We retrospectively analyzed a total of 684 cases, performed between July 2003 and June 2013 in our Hospital. Anastomosis complications, such as leakage, stricture and bleeding, were analyzed in relation to the three methods of anastomosis, hand-sewn (HS), functional end-to-end (FEEA) and triangulating anastomosis (TRI). Results: Univariate analysis indicated that the incidence of leakage was significantly lower in laparoscopic surgeries (p=0.034) and TRI (p=0.047). The results of the multivariable analysis indicated that anastomotic leakage was significantly less with TRI (p=0.029). Conclusion: In colon surgery, TRI seems to be associated with a low risk of anastomotic leakage compared to HS and FEEA.
Several types of intestinal anastomoses following colonic resection have been devised in the past. While the types of intestinal anastomoses can be classified into hand-sewn (HS) and stapled anastomosis, the latter has been the mainstream in recent years due to simplicity and being less time-consuming (1-3) of which functional end-to-end anastomosis (FEEA) has been used widely (4). This technique has been proven especially useful for intestinal anastomosis with discrepancy in diameter (5), with a number of studies reporting that FEEA is an easy and safe technique compared with the conventional HS procedure (6, 7). On the other hand, Venkatesh et al., in 1993, reported a stapled intestinal anastomosis called triangulating anastomosis (TRI) (8). For colon surgery, TRI is a simple end-to-end anastomosis and more physiological than FEEA for which only a few studies have been undertaken (9, 10). In colon surgery, there is no golden standard of anastomotic techniques, which is generally selected by surgeon's preferences or by local conditions. In this study, we retrospectively conducted a comparative analysis to report the outcome of colon resection to evaluate the safety of anastomotic techniques.
Patients and Methods
Patients. From July 2003 to June 2013, 1,324 patients underwent colorectal surgery with primary intestinal reconstruction at the Jikei University Hospital, Tokyo, Japan. A retrospective comparative investigation was carried out to study the influence of the methods of intestinal anastomosis on anastomotic complications using the data from 684 cases, after exclusion of the following cases, some with multiple overlaps: emergency surgery (29 cases), rectal anastomosis (594 cases), use of a circular stapler (627 cases) and creation of a defunctioning stoma (113 cases). The patients were classified into three groups by the type of anastomosis as follows: HS (n=93), FEEA (n=255) and TRI (n=336) (Table I). Methods of intestinal anastomoses were selected by the preference of each surgeon. The diagnosis of anastomotic leakage was defined based on imaging studies and clinical signs, such as fever >38.5°C, leukocytosis, elevated serum C-reactive protein, drainage of intestinal content from the drain or computed tomography findings of abscess formation around the anastomosis. The diagnosis of anastomotic stricture was defined based on imaging studies demonstrating intestinal distension starting from oral side of the anastomotic site. Anastomotic bleeding was defined by melena or endoscopic findings within seven days after surgery.
As patient's factors, we classified tumor locations into two groups: right-sided colon (cecum, ascending colon and right transverse colon) vs. left-sided colon (left transverse colon, descending colon and sigmoid colon).
We investigated the relation between anastomotic complications (anastomotic leakage, stricture and bleeding) and clinical factors, such as age, gender, etiology (benign or malignant), location (right-sided colon or left-sided colon), anastomosis (ileo-colostomy or colo-colostomy), approach (open or laparoscopic), operation time, estimate of blood loss and anastomotic method (HS, FEEA or TRI). This study was approved by the Institutional Review Board (27-2s83 8168).
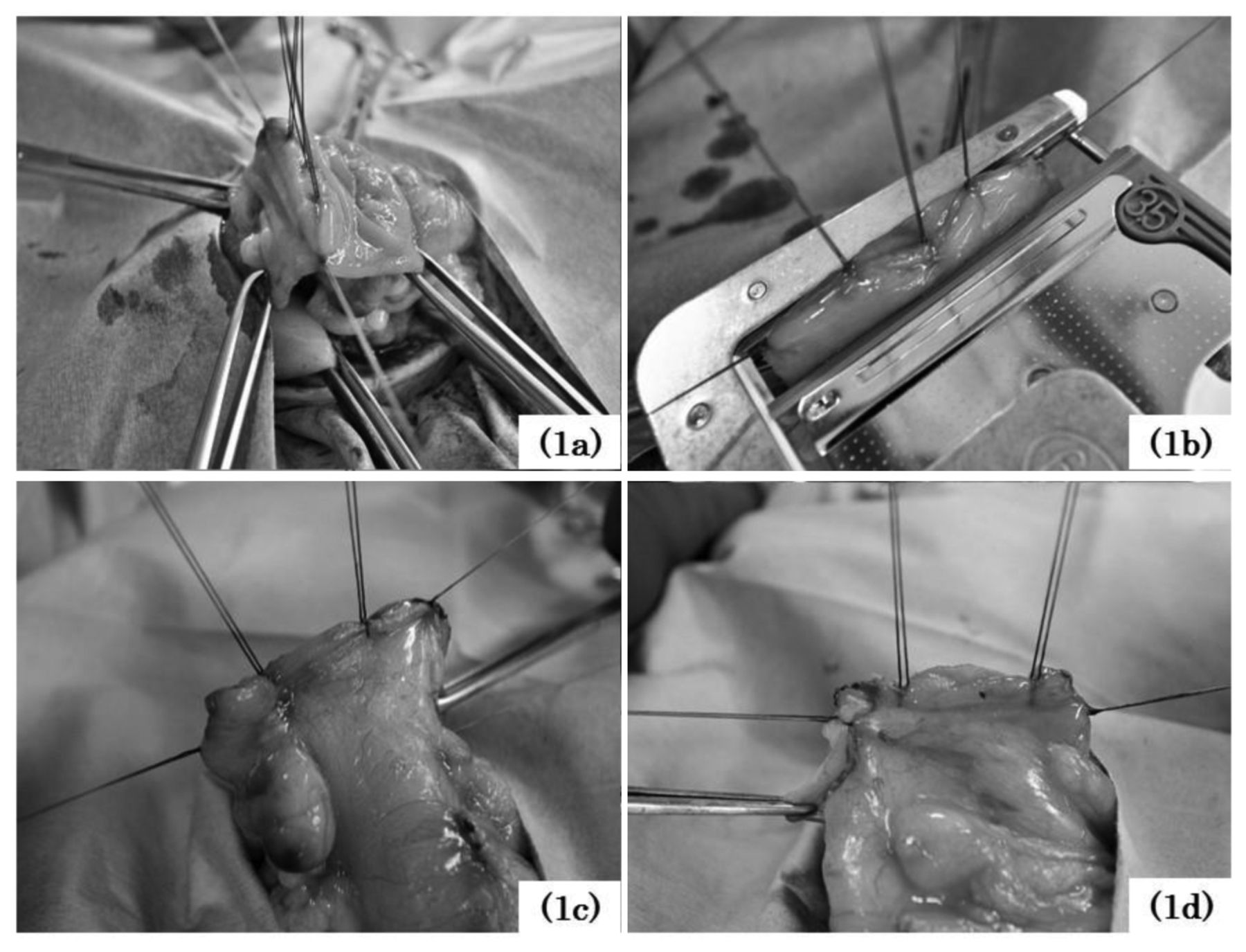
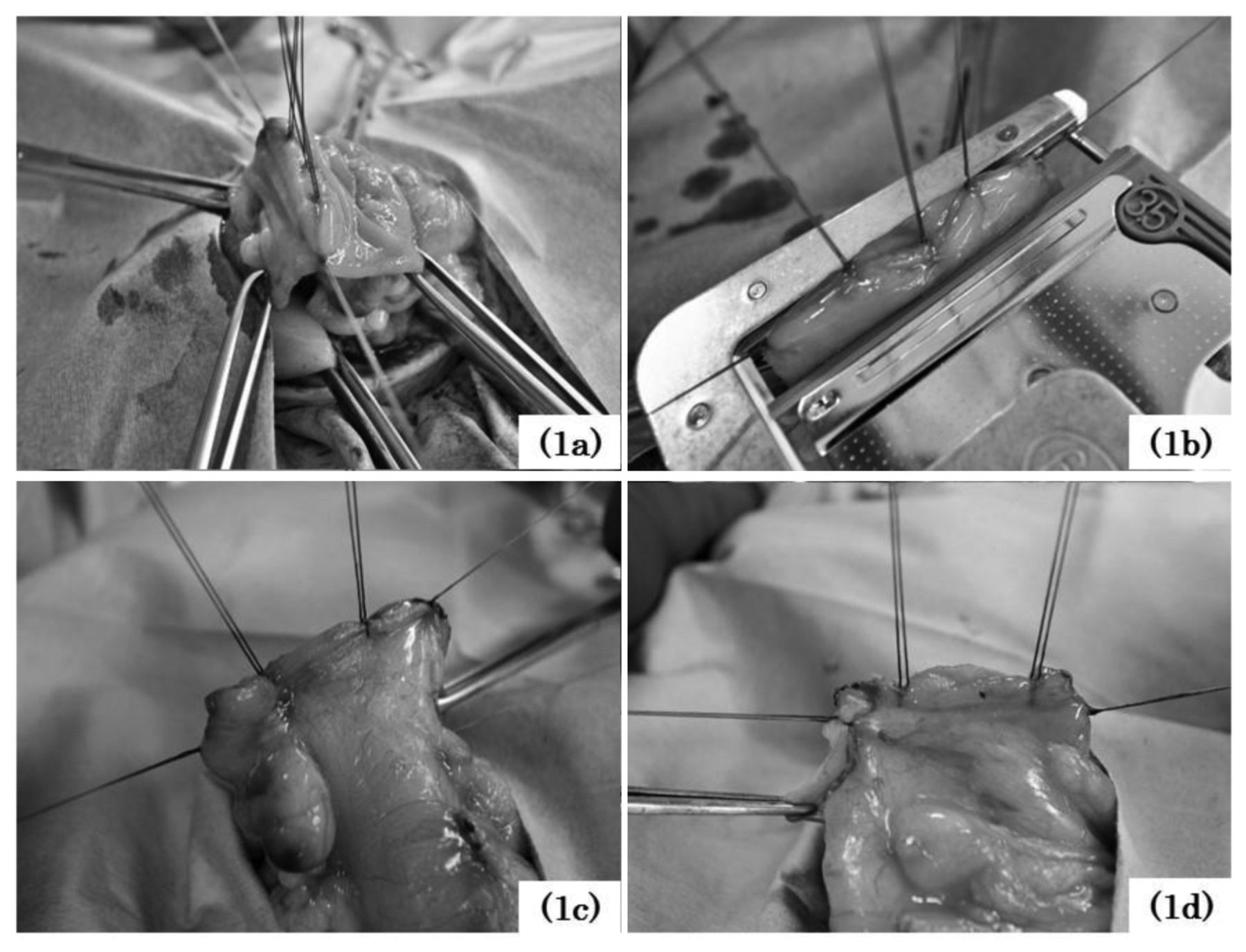
Surgical techniques. (i) TRI: In case of ileo-colostomy, antimesenteric intestinal wall was incised vertically from the wall edge to compensate for the difference in diameter after colectomy. Since 2008, the incision of the intestinal wall edge in colo-colostomy has been carried out to enlarge the anastomosis diameter. The circumference of the walls of the intestinal tract was divided into three parts and a linear stapler (TA™ 60-3.5 with DST Series™ Technology; Medtronic Inc., Minneapolis, MN, USA or PROXIMATE® Reloadable Linear Stapler (TX) 60; Ethicon Inc., Somerville, NJ, USA) was used three times to anastomose each part. At the posterior one-third of the circumference of the mesentery (posterior wall) side, transmural stay sutures were placed in an inverted manner in five sites (Figure 1a). By pulling up stay sutures, the posterior wall was anastomosed from the mucosal side, including the five stay sutures using a linear cutter (one-third of the circumference) (Figure 1b). Then, corner stay sutures were placed on both ends of the first anastomosis to evert both sides of the anastomosis and, then, another whole-layer stay suture was placed in the center of the residual two-third of the circumference. Two more sutures were similarly added in an everted manner between these sutures (Figure 1c). Subsequently, one-half of the residual two-third of the circumference was anastomosed in two steps with a linear stapler. Finally, the remaining one-third of the circumference was also anastomosed in an everted manner (Figure 1d). The intersection of staple lines was not reinforced by seromuscular sutures.
(ii) FEEA: The anastomotic technique was basically adapted by the method originally described by Steichen (11) with minor modifications advocated by Chassin et al. (12). The sites of division of the colon or ileum were selected and the mesentery was divided. Proximal and distal intestines were separated using a linear stapler (DST Series™ GIA™ Stapler, Endo GIA™ Ultra Universal Short Stapler; Medtronic Inc. and Proximate® Linear Cutter 75 or ECHELON FLEX™ ENDOPATH® Stapler 60mm; Ethicon Inc.) or a knife at the division sites. For the use of a linear stapler, a small hole, large enough for insertion of the fork of the stapling device, was made in the wall at the antimesenteric border of each intestine. The forks were inserted in full length and fired along the antimesenteric border to perform a side-to-side anastomosis. After the stapling instrument was removed, the stump of the intestinal tract was grasped with Allis clamps in an everted manner while avoiding overlapping of the staple line edges of side-to-side anastomosis and closed using another linear stapler. Finally, two or three reinforcing sutures were placed at the distal end of the longitudinal (first) staple line between the intestines.
(iii) HS: An absorbable suture was used for anastomosis using the Albert-Lembert method or the layer-to-layer method.
Statistical analysis. The retrospective analysis was performed to study postoperative complications at the anastomotic site, i.e. anastomotic leakage, stricture and bleeding. Univariate analysis of complications at the anastomotic site was performed using the Student's t-test or the Chi-squared test. In addition, a backward elimination stepwise approach was utilized for multivariate analysis. In either statistical analysis, p<0.05 was considered statistically significant. The statistical analysis was performed using a statistics analysis SPSS version 22 software (IBM Inc., Chicago, IL, USA).
Patients' characteristics.
Results
Patients' characteristics. Table I shows patients' characteristics. Most operations were for colon cancer and with right-sided predominance.
Comparisons of surgical results. Table II shows surgical results of each group. As to leakage of the four cases of anastomotic leakage following FEEA, three cases required reoperation.
Concerning stricture, the patient following HS showed improvement by conservative treatment with five days of fasting. All four cases of stricture following TRI underwent successful endoscopic balloon dilatation with the diameter ranging from 11 mm to 18 mm of 3 to 12 times (average=5.5).
For bleeding, hemostasis by endoscopy was successful in both cases of TRI, while patients with FEEA did not undergo endoscopic evaluation due to ventilator-dependent sever pneumonia. Conservative treatment, however, resulted in hemostasis.
Univariate analysis. Table III demonstrates the results of univariate analysis on overall anastomotic complications, indicating that the incidence of anastomotic leakage was significantly lower by the laparoscopic approach (p=0.034) and with TRI (p=0.047). Although five cases resulting in anastomotic leakage at colo-colostomy required reoperation, there was no significant difference with ileo-colostomy (p=0.297).
Techniques of triangulating anastomosis.
Anastomotic stricture developed significantly more frequently after colo-colostomy (p=0.003). For colo-colostomy, following the fourth case of anastomotic stricture in 2008, we routinely made the anastomotic diameter larger by incising the colon. After this, the occurrence of stricture symptoms was no longer present (Table IV).
Although a total of three cases of anastomotic hemorrhage occurred, univariate analysis did not reveal participation of any significant factor.
Multivariate analysis. Table V shows the results of multivariate analysis on complications of the anastomosis. Anastomotic method was the only significant factor in relation to leakage, which was the lowest in TRI (p=0.029). Otherwise, no significant differences were identified in anastomotic stricture or bleeding.
Discussion
It is still controversial which anastomosis technique is safer in colon surgery. Amri et al. made a comparison between HS and stapled anastomosis in colon cancer surgery (13). They reported that duration of operations using stapler was significantly shorter than HS, with complication rates not differing significantly between the groups. In the complications of colon cancer surgery, anastomotic leakage after colon cancer surgery not only increased duration of hospital day and mortality rate, but also worsened the long-term oncological outcome (14). Typically, the percentage of anastomotic leakage in colon surgery has been reported to be below 8% (9, 10, 13, 15, 16). In this study, the incidence of anastomotic leakage was 2.2% for HS, 1.6% for FEEA and none for TRI, indicating a relatively low percentage when compared to past reports. Anastomotic leakage has not been reported in TRI for the last decade in our Institution. Additionally, according to a report by Fukunaga et al. (10), the percentages of anastomotic leakage were 3.0% for HS, 2.8% for FEEA and 0.6% for TRI. Also, in their report, a significant decrease was found in TRI as compared to HS but not as compared with FEEA.
Comparisons of surgical results.
Univariate analysis for complications of anastomosis.
Next, as far as the anastomotic strictures are concerned, although the results of univariate analysis indicate that the anastomotic intestine (colo-colostomy) was the only significant independent factor, four of the five cases of the stricture were anastomosed by TRI. Regarding the absence of anastomotic stricture after colo-coloctomy with extension of the anastomotic diameter, although many previous reports link anastomotic stricture to ischemia, anastomotic leakage, radiation therapy and stapled anastomosis (17-19), our experience indicates that the diameter of the anastomosis in colo-colostomy is also important. As far as the treatment of anastomotic stricture in this study is concerned, endoscopic balloon dilatation to allow passage of the endoscope with a diameter of 12 mm appears successful.
Concerning the absence of significant independent factors for anastomotic bleeding, the results are comparable to previous reports (9, 10), which seem to indicate stapled anastomosis as a risk factor.
In recent years, colon surgery is undergoing a transition from laparotomy to laparoscopic procedures in developed countries. In laparoscopic surgery, intestinal anastomosis is frequently performed extracorporeally due to difficulty with intracorporeal anastomosis connected to technical reasons (15). However, a broader intestinal mobilization and dissection are required for extracorporeal anastomosis in laparoscopic surgery. In fact, with FEEA, the intestine is anastomosed side-to-side, requiring a longer dissection of the intestine than the conventional end-to-end anastomosis, which is a draw-back for FEEA in laparoscopic colectomy. In comparison with FEEA, which is widely performed in advanced countries, TRI requires a shorter intestinal tract length to anastomose and the form of anastomosis is similar to a physiological end-to-end anastomosis. In addition, TRI is more cost effective than FEEA (9) as it is considered to be an appropriate anastomosis for laparoscopic surgery. However, as this is a retrospective single Institution series, a large-scale randomized trial is required to validate our results.
Historical analysis for stricture following triangulating anastomosis (TRI).
Multivariate analysis for complications of anastomosis.
Conclusion
In colon surgery, TRI seems to be a safe anastomotic technique that is less likely to result in anastomotic leakage compared to HS or FEEA.
Footnotes
This article is freely accessible online.
- Received May 2, 2017.
- Revision received May 16, 2017.
- Accepted May 17, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}