


Abstract
Aim: A single-institution, retrospective study was performed to investigate potential techniques to minimize radiation exposure to the testicles during heterotopic ossification (HO) prophylaxis. We report the impact of split-beam technique (SBT) and different photon energies on the total dose of radiation received by the testicles during prophylaxis of HO. Materials and Methods: Between 2008 and 2010, we identified 64 patients with traumatic acetabular fractures who underwent surgery followed by radiation therapy (RT) without testicular shielding. Postoperative RT was delivered within 72 h in a single fraction of 700 cGy using 6-18 MV photons, without testicular shielding due to patient refusal. All patients underwent 3-D RT planning in which the testicles were contoured as a region of interest and dose-volume histograms (DVH) were generated. Additional treatment planning trials were created for each patient by utilizing a SBT medially and by using different photon energies (6, 10 and 18 MV) to study the effects of these maneuvers on the delivered dose to the testicles. Results: In reviewing the DVH, it was noted that the mean dose delivered to the testicles was 10 cGy (range=3-40). The maximum dose was 31 cGy (range=7-430). When SBT was utilized, a significant reduction in the mean (44%) and maximum (47%) doses delivered to the testicles was noted. Further reductions in the mean (26%) and maximum (14%) doses were achieved by using higher-energy (10-18 MV) beams. The radiation doses to the testicles from the CT simulation and the two portal images were estimated to be 4 and 1.5 cGy, respectively. Conclusion: Low-dose prophylactic RT to prevent HO around the hip causes a low, but likely biologically meaningful, radiation dose to be delivered to the testicles. This dose could be further reduced by using a medial SBT and photon energies above 6 MV. Testicular shielding should be offered to all male patients receiving such RT. In addition, all patients should be informed about the consequences of testicular radiation as part of their informed consent.
- Radiation therapy (RT)
- acetabular fracture
- heterotopic ossification (HO)
- megavoltage photon
- split-beam technique
- testicular dose
- radiation prophylaxis
- indomethacin
Heterotopic ossification (HO) is the pathological process of bone formation in non-osseous tissues following trauma and/or surgical intervention. Following traumatic injury, cellular and hormonal signals from the site of injury, a supply of mesenchymal cells and the appropriate tissue microenvironment are all among the potential factors that could contribute to development of HO in injured tissues (1). Prophylactic radiation therapy (RT) is commonly used to reduce the risk of HO after open reduction and internal fixation (ORIF) of traumatic acetabular fractures (TAFs); heterotopic ossification after operative treatment of the hip using a posterior surgical approach has been reported in up to 50% of such patients (2). Radiation therapy presumably decreases the risk of HO by inhibiting the proliferation of pluripotential mesenchymal cells that could potentially differentiate into osteoblastic stem cells and is usually administered postoperatively, within 72 h of surgery (3-5). However, preoperative RT has also been used in these situations (6-8). In a recent meta-analysis reporting the incidence of HO after TAF status post ORIF, it was reported that the incidence of HO formation after RT prophylaxis alone was 27%, 37% after indomethacin prophylaxis alone and 12% after both RT combined with indomethacin. The incidence of HO was 58% in the control arm (i.e., patients who did not receive any form of prophylaxis) (4, 9). Most patients who develop HO are males with a TAF. The testes, given their proximity to the pelvis, are always exposed to scatter radiation from RT, which has the potential to alter sperm count and morphology. Since sperm abnormalities have been reported with doses of only 15 cGy, all males should be counseled and treated with a testicular shield (10, 11) in place (12, 13). Here we report our testicular dose estimates and discuss techniques that can optimize coverage while delivering the smallest testicular dose.
Materials and Methods
Study objective and schema. For this analysis, we conducted a retrospective study to assess the RT doses to the scrotum/testicles during single-fraction treatment for HO prevention and investigated techniques that could reduce the dose to the scrotum/testes in patients who decline, for whatever reason, to allow the use of a testicular shield. We hypothesized that the scattered dose to the scrotum/testicles would be minimized by utilizing a split-beam technique (SBT) medially and, by using higher photon energies (10 and 18 MV), we could consequently diminish most RT-induced scattered dose.
Patient population. This study represents a single-institution; retrospective investigation performed at the University of Mississippi Medical Center, Jackson, MS, USA, and was fully approved by our Institutional Review Board.
Patient eligibility and design. Between 2008 and 2010, 64 male patients who had been treated in standard operative fashion for TAF at the Department of Orthopedic Surgery were then referred to the Department of Radiation Oncology for prophylaxis of HO with RT. All patients had experienced a TAF that required ORIF. RT prophylaxis was delivered with or without indomethacin. For all patients, the following data were tabulated (Table I): age, types and causes of fracture, surgical approach used, RT and usage of indomethacin.
Surgical treatment. All surgical procedures were performed by fellowship trained, orthopedic trauma surgeons. All patients underwent ORIF via a posteriorly approached (Kocher-Langenbeck) surgical exposure with the patient in either lateral or prone position (15, 16). Early postoperative patient mobilization, with toe-touch weight bearing as tolerated, was initiated for all patients.
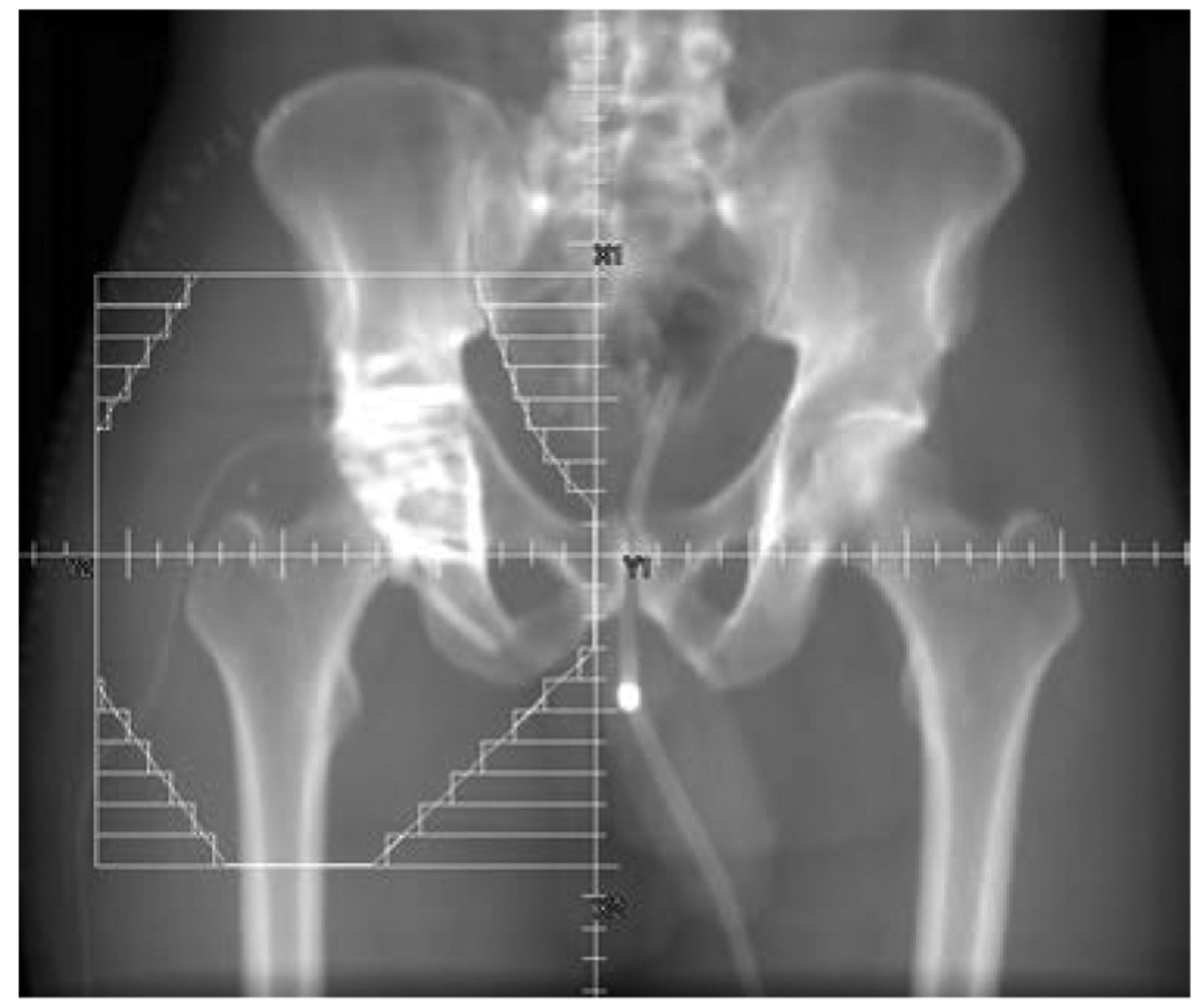
Radiation treatment. RT was used prophylactically for all the patients and delivered within 72 h after the ORIF. Seven hundred cGy was delivered in a single fraction to the mid-plane, using 6-18 MV photons. Treatment fields included the soft tissues around the proximal femur and acetabulum without bone shielding (15-17). Five different treatment plans were generated after CT simulation (the process used to determine the exact location, shape and size of the targeted area to be treated) to investigate the testicular doses. The first plan was generated by placing the isocenter in the middle of the field, the second plan by applying a SBT (e.g. half-beam block) wherein the isocenter was placed at the fractured acetabulum (Figure 1). Subsequently, three different plans were generated for each isocenter using 6, 10 and 18 MV photons for comparison. Dose-volume histograms (DVHs) were generated for evaluation of the computed scattered dose delivered to the testicles (Figure 2).
Patient characteristics.
Medical treatment. Forty percent (25/64 patients) of the whole cohort received RT with indomethacin. Indomethacin was prescribed at the discretion of the surgeon at the dosage of 25 mg three times per day after meals, beginning on postoperative Day 1 and continued for 6 weeks thereafter; however, patient compliance with daily intake was not verified.
Follow-up. Patients had follow-up appointments at 2 weeks, 1 month, 3 months, 6 months and 1 year from the day of discharge. Standard hip X-rays (AP, PA and oblique) were obtained for evaluation of HO per the Brooker classification (18), avascular necrosis of the femoral head or loosening, malunion or non-union of the fracture. Computed tomography of the pelvis was obtained where considered clinically appropriate. All patient medical records and X-rays were reviewed to determine the efficacy of the RT in preventing HO.
Hypothesis and study end-points. In this study, we hypothesized that by utilizing a SBT medially and using higher photon energies (10 and 18 MV) we could minimize the scattered dose to the scrotum/testicles and, thereby, minimize RT-induced testicular damage.
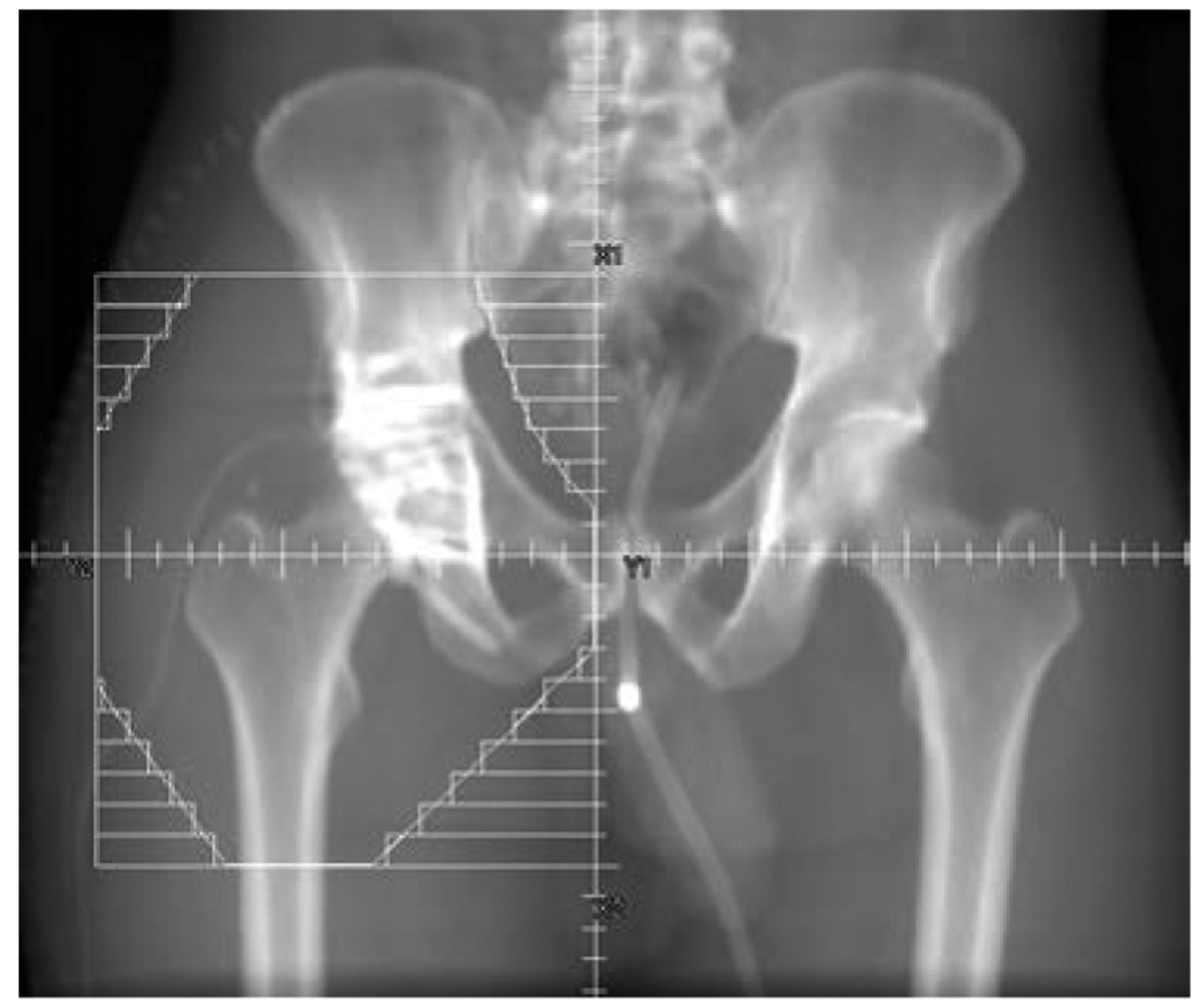
Split-beam technique (SBT, e.g. half-beam block.
The impact of beam-split technique (BST) and different photon energies (6, 10, 18 MV) on testicular dose.
Statistical methods. Univariate and multivariate regression analyses were used to compare testicular doses received in the different groups, after adjusting for all other factors that could potentially affect HO formation (Body mass index (BMI), tissue separation, type of fracture and surgical approach to fracture exposure).
Results
The median patient age was 33 years (range=16-65). Motor vehicle crashes (MVC) (100%) was the cause of the fractures in all our patients. The median BMI was 28 (range=20-46). Posterior acetabular wall and combined posterior wall and T-shaped fractures were the types of injury seen in the majority of patients. All patients were males and all underwent ORIF via the Kocher-Langenbeck approach; thereafter, all underwent CT-based simulation and 3-D RT planning. At a median follow-up of 3 years for the whole cohort, the incidence of HO in all patients was only 5% (3/64) with RT with/without indomethacin.
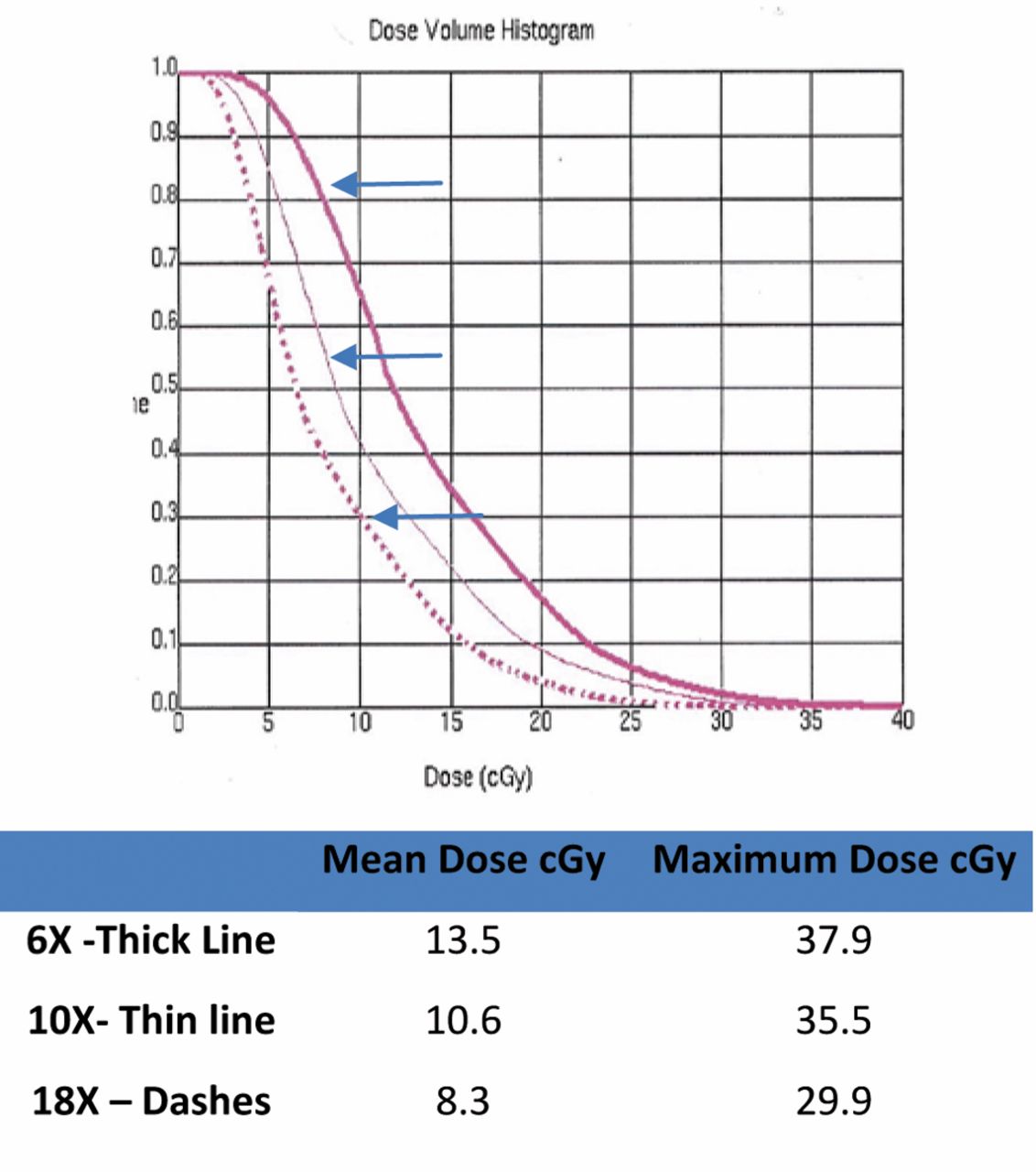
Dose–volume histogram shows the impact of beam-split technique (BST) and different photon energies (6-thick line, 10-thin line, 18-dashes MV) on testicular dose.
The univariate regression test was applied first to test for an association between testicular dose reduction and SBT and different photon energies before adjusting for other factors. There was a significant reduction in the testicular dose (p<0.0001) with SBT. Further, multivariate regression analysis confirmed the significant reduction in testicular dose after adjusting for all other factors (age, BMI, separation, size of the RT field, types of fracture and surgical exposures) that could potentially impact the testicular dose.
In reviewing the DVH for the 64 patients (Figure 2, Table II), it was noted that the mean (Mean dose) delivered to the testicles using the three different beam energies was 10 cGy (range=3-40), while the mean (Maximum dose) from the three beam energies was 31 cGy (range=7-430). When a SBT was applied at the medial edge of the field, a significant reduction in the mean (Mean dose) (44%) and mean (Maximum dose) (47%) dose delivered to the testicles was noted. Moreover, additional dose reductions in the mean(Mean dose) of 26% and mean (Maximum dose) of 14% were achieved by using a higher beam energy (10 or 18 MV), when compared to 6 MV photons. The radiation doses to the testicles from the CT simulation and the two portal images were estimated at 4 and 1.5 cGy, respectively.
Discussion
HO is the pathological process of bone formation in non-osseous tissues following trauma and/or surgical intervention. This misplaced growth occurs between muscle planes and not within the muscle fibers themselves (18). HO was first identified and reported in the literature in 1883 by Riedel (20), a German physician. It was later observed by the French physicians Dejerne and Ceillier (21) in patients suffering traumatic paraplegia in World War I. There are several factors that appear critical to HO formation – a traumatic injury, signals from the site of injury, a supply of mesenchymal cells and the appropriate tissue microenvironment – all appear to be factors that may contribute to the development of HO in injured tissues (1). The most common procedures that result in HO are: ORIF of an acetabular fracture or a total hip arthroplasty (THA) (4, 9). Many clinicians recommend prophylactic RT and/or non-steroidal anti-inflammatory medications (NSAIDs) to prevent HO.
Radiation therapy presumably decreases the risk of HO by inhibiting the proliferation of pluripotential mesenchymal cells that could potentially differentiate into osteoblastic stem cells and is usually given postoperatively, within 72 hours of surgery or preoperatively (3-8). We hypothesized that by utilizing a SBT medially and/or by using higher photon energies (10 and 18 MV), we could minimize the scattered dose to the scrotum/testicles and, consequently, diminish the RT-induced testicular damage. In order to achieve minimal dose divergence at the beam edge, a split beam technique, sometimes called a half-beam block, is often used. In this method, the beam is split along the plane containing the central axis inhibiting geometric divergence of the beams at the split line (22). This technique is often employed in matching one field to another. By applying a half-beam block in the medial edge of the pelvic AP/PA fields in HO prophylaxis, much of the dose that can potentially diverge into the testes, bowel and bladder is diverted laterally.
Most patients who develop HO are males after a TAF. The testes, given their proximity to the pelvis, will be exposed to scattered radiation, which has the potential to alter sperm count and morphology. Radiobiological studies have shown that the testicles are very radiosensitive and very low doses of radiation have been shown to alter sperm production and morphology and cause transient or even total azoospermia/sterilization (11). The largest study (53 patients) evaluating testicular dose and sperm function was conducted by the Southwest Oncology Group (27). The median gonadal dose in this study was 79 cGy. Recovery of fertility occurred approximately 1 year after radiation, which was both dose- and time-dependent. Hall et al. (11) have reported a temporary reduction in the number of spermatozoa with radiation doses as low as 10 cGy and temporary sterility at doses of 15 cGy. Moreover, Freund et al. (29) reported on testicular function dysfunction in 8 seminoma patients treated with radiation, where the absorbed gonadal radiation dose ranged from 15 to 157.5 cGy.
In a prospective study by Patel et al., patients were treated with 800 cGy without direct exposure of the testes/scrotum and while using a testicular shield. Thermoluminescent dosimeters were placed inside and outside the shield. The mean dose inside and outside the shield was 10.2 and 20.2 cGy, respectively. The authors concluded that young males should be counseled of the risks of testicular radiation and treated with a testicular shield (10). Bieri et al. have reported that the daily dose to the testes was 1.86 cGy per fraction without gonadal shielding and 0.65 cGy per fraction with gonadal shielding for males with seminoma treated at 1.8 Gy per fraction to a para-aortic field, suggesting that a scrotal shield should be used to reduce the scatter dose to help avoid impairment of spermatogenesis (27). For male patients presenting for RT prophylaxis of HO, it is standard practice to routinely offer testicular shielding for all patients who want to preserve their fertility or the ability to conceive, since the RT field is in close anatomical proximity to the testes (12, 13).
In a study utilizing dose modeling in phantoms, the estimated total gonadal dose and risk of hereditary effects during therapeutic external irradiation was shown to be ~39 cGy using 6 MV photons without the SBT technique; this was associated with a risk for genetic effects in offspring of 23.4×10−4. This is 4 times greater than the risk generated from a typical computed tomography scan of the abdomen, which was estimated to be 6×10−4 in males (14). Generally, most radiation oncologists would agree that side-effects, such as temporary azospermeia and sperm chromosomal abnormalities from scattered dose to the testes, could happen with very low RT doses in the range of 10 to 15 cGy (10). Thus, using a SBT with higher photon energy, as we have reported, has the potential to reduce risk for genetic effects in offspring by two thirds.
Some male patients specifically decline to use the clam shell testicular shield, as did all the patients in this study. Others may be so obese that the standard shell will not fit comfortably between the excess tissues in the thighs of the patient. For such patients then, we must use non-shield techniques to obtain adequate coverage of the targeted area while providing the least integral dose to the testicles. In the current study, we retrospectively evaluated how one could minimize the RT doses to the scrotum/testicles during single-fraction treatment for HO prevention.
We were able to minimize the testicular dose by applying SBT and higher photon energies. There was a significant reduction (>50%) of testicular dose by utilizing these simple-to-use maneuvers. Using SBT and ≥10 MV photon beams led to a smaller scattered RT dose compared to lower energy 6 MV photons. Higher energies lead to a more consistently forward directed beam and decreased side scattering. The major caveat of using high energy 18 MV photons, however, is the neutron contamination that occurs when beams with >10 MV energy are used. The dose contribution to the testicles from neutron contamination in 15 MV or 18 MV photons is difficult to quantify. For this reason, beams of energy 15 MV and higher should also be avoided due to the increased neutron contamination from beam modifying components of high atomic number, such as the target and jaws (30). In conjunction with a “half-beam blocking” technique, one can also employ a physical shield to protect the testes from scattered radiation during treatment as has been demonstrated by Fraass and colleagues (30). They described the use of testicular shielding for testicular dose reduction in 1985. Shields are commercially available and, while considered to be a standard part of therapy when treating young males in the setting of Hodgkin's disease or seminoma, they have not been used as commonly, during HO prophylaxis.
Mourad et al., in 2010, presented the first radiation-induced sarcoma case in the literature after RT prophylaxis of HO. The possibility of second malignancy after RT, especially in younger patients, is an additional concern and should be discussed with the patients. However, it is a rare side-effect and only 2 cases of radiation-induced sarcoma have been reported in the literature to date (23-26). There are two basic approaches to reduce the RT scatter dose effect on the testes. One approach is to improve the treatment delivery so as to decrease the amount of scattering dose, which can be achieved by using CT simulation, SBT and photon energies greater than 6 MV (27, 22). This effect is mainly a result of the decrease in penumbra and lateral scattering when going from lower to higher energy beams.
In summary, our results suggest that the use of field modification and higher beam energies during RT for HO prophylaxis appears to consistently reduce the radiation dose to the scrotum/testicles by about two- to three-fold of the values obtained using standard blocks and lower beam energy. This could translate into a by two- to three-fold reduction of risk for genetic effects in offspring. We also advocate the routine use of a testicular shield for all male patients receiving radiation for HO prophylaxis. Although, a testicular shield is effective in shielding scatter from external (machine head) sources, it does little to prevent in-scatter into the testicular region from within the patient. Hence, in order to further minimize the gonadal dose while maximizing sufficient target volume coverage, we recommend that CT-based simulation, 3-D treatment planning, a SBT and ≥10 MV photon beams be utilized (28, 32-34).
Conclusion
Although a biologically meaningful radiation dose appears to be delivered to the testicles during low-dose prophylactic RT to prevent HO around the hip, this dose could be further reduced by minimizing the side scattering via the use of a medial SBT and photon energies ≥10 MV. Moreover, testicular shielding should be offered to all young male patients receiving HO prophylaxis using RT. Informed consent of the patient should include possible alteration in sperm production and morphology. Use of CT simulation and 3-D treatment planning will allow more accurate delineation of the tissues to be irradiated and, consequently, improved precision in RT delivery.
Footnotes
This article is freely accessible online.
Presented at the American Society for Therapeutic Radiology and Oncology (ASTRO) 56th Annual Meeting 2014.
Conflicts of Interest
All Authors do not have any conflict of interest. There is no copyrighted information.
- Received February 1, 2017.
- Revision received March 13, 2017.
- Accepted March 14, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}