


Abstract
Background: Surgical resection is currently considered the only potentially curative option as a treatment strategy of colorectal liver metastases (CRLM). However, the criteria for selection of resectable CRLM are not clear. The aim of this study was to confirm a new prognostic indicator of CRLM after hepatic resection. Patients and Methods: One hundred thirty nine patients who underwent initial surgical resection from 1994 to 2015 were investigated retrospectively. Prognostic factors of overall survival including the product of maximum diameter and number of metastases (MDN) were analyzed. Results: Primary tumor differentiation, vessel invasion, lymph node (LN) metastasis, non-optimally resectable metastases, H score, grade of liver metastases, resection with non-curative intent and MDN were found to be prognostic factors of overall survival (OS). In multivariate analyses of clinicopathological features associated with OS, MDN and non-curative intent were independent prognostic factors. Patients with MDN ≥30 had shown significantly poorer prognosis than patients with MDN <30 in OS and relapse-free survival (RFS). Conclusion: MDN ≥30 is an independent prognostic factor of survival in patients with CRLM and optimal surgical criterion of hepatectomy for CRLM.
The liver is the most common site of metastasis in patients with colorectal cancer (CRC) (1), with 15-25% of patients presenting synchronous colorectal liver metastases (CRLM) (2). In addition, another 25-50% of patients develop subsequent metachronous metastases during the course of the disease (2, 3). Surgical resection is currently considered the only potentially curative option for patients with metastatic CRC confined to the liver (4, 5), and is associated with a 5-year overall survival (OS) rate of 37-58% (6). However, only 15-30% of patients with liver metastases may be initially resectable (7, 8), but the criteria for selection of resectable CRLM remain unclear.
According to Nordlinger et al., patients with CRLM have been classified into three clinical categories: (i) patients with resectable metastatic disease; (ii) patients with metastatic disease that is not optimally resectable (tumor size >5 cm, >4 metastases, synchronous CRLM, primary lymph node (LN)-positive, positive tumor markers and/or technically difficult) and (iii) patients unlikely to ever become resectable (9). Neoadjuvant chemotherapy was recommended for patients with resectable and unresectable CRLM, whereas first-line surgical resection was recommended only for patients with solitary metastases ≤2 cm and good prognostic features (10). In the European Society for Medical Oncology (ESMO) consensus guidelines for the management of patients with CRLM, patients were categorized by technical and oncological criteria. Oncological categories include (i) concomitant extrahepatic disease; (ii) number of lesions ≥5; (iii) tumor progression, with no mention of tumor size (11). However, clear criteria of surgical resection for CRLM have never been established.
On the other hand, in hepatocellular carcinoma, the Milan criteria are used for a simple selection for liver transplantation around the world. The adaptation of liver transplantation was limited to one lesion smaller than 5 cm or up to 3 lesions smaller than 3 cm, and it is representing an approximate volume of tumor. In CRLM, simple criteria, using tumor number and size are required.
Perioperative or neoadjuvant chemotherapy with various agents, alone or in combination, is the standard of care for most patients with CRLM (12, 13). Neoadjuvant chemotherapy in patients with initially unresectable CRLM can reduce metastasis sizes, converting initially unresectable to resectable lesions (conversion treatment) (9), making systemic chemotherapy in combination with liver resection an accepted standard of care in patients with CRLM (10, 14). However, there are currently no particular criteria for resectability of CRLM, especially focusing on tumor volume in the liver.
The aim of this study was to confirm a new prognostic indicator of CRLM after hepatic resection.
Patients and Methods
Patients. This study was performed in accordance with the Helsinki Declaration of the World Medical Association. This retrospective study enrolled 246 patients with CRLM treated at Tokushima University Hospital from 1994 to 2015. Of these, 139 patients who underwent initial surgical resection with curative intent and without any preceding chemotherapy were included in this study. The remaining patients included 22 who received best supportive care and 85 who received systemic chemotherapy. Our treatment strategy for CRLM is curative hepatectomy whenever possible on all patients with CRLM if their remnant liver volume was ≥40%, even after chemotherapy or hepatectomy.
Patients were evaluated preoperatively by abdominal ultrasound (US), helical computed tomography (CT) scan, and/or magnetic resonance imaging (MRI). All with CRC and synchronous or metachronous liver metastases were diagnosed histologically. Maximum tumor diameter and number of tumors were determined by CT and resected specimen. Resection status (curative vs. non-curative) was evaluated by histopathological assessment of excised metastases together with the operation notes.
The 139 patients included 85 men and 54 women with mean age 66±0.95 years (range=33-92 years). The median patient follow-up for all patients was 48.7 months (range=4.4-162.1 months). Perioperative mortality was defined as death within 3 months of operation. In all 139 patients who underwent initial hepatic resection, the perioperative mortality was 0%.
Methods. Staging and curability were defined according to the criteria of the Japanese Society for Cancer of the Colon and Rectum. Liver metastasis was classified as H1–3, with H1 defined as four or fewer tumors with a maximum diameter <5 cm; H3 as >5 tumors of size >5 cm; and H2 as anything intermediate. Liver metastasis grade was defined as A-C, with H1 and ≤3 regional LN metastases classified as grade A; H2 with ≤3 regional LN metastases or H1 with ≥4 LN metastases classified as grade B, and all other conditions classified as grade C.
Statistical analysis. Univariate analysis of differences between groups was determined by log-rank tests and multivariate analysis by chi-squared tests. The endpoints were overall survival (OS) and relapse-free survival (RFS). Survival curves were plotted using the Kaplan–Meier method and 5-year OS and RFS rates were analyzed. Two-sided p-values <0.05 were considered statistically significant. All statistical analyses were performed using JMP version 13 statistical software (SAS, Campus Drive Cary, NC, USA).
Results
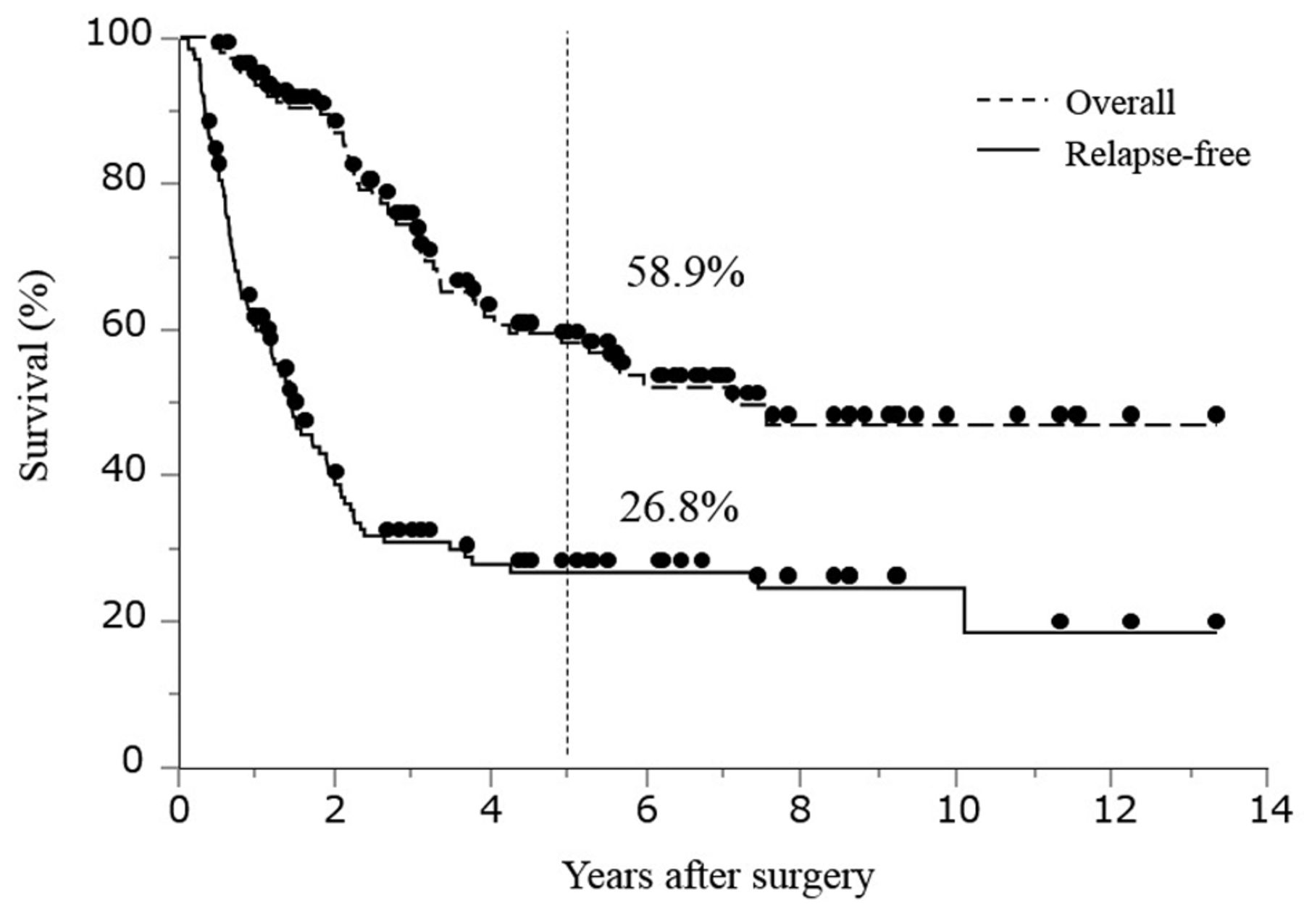
Overall and relapse-free survival. Survival curves of the 139 patients were plotted by the Kaplan–Meier method. The 5-year OS and RFS rates were 58.9% and 26.8%, respectively (Figure 1). Median overall survival was 89.26 months (SD=2.92).

Overall and relapse-free survival curves of 139 patients with colorectal liver metastases who underwent initial surgical resection.
Univariate and multivariate analysis of clinicopathological features associated with overall survival. The product of maximum diameter and number (MDN) was newly defined as an indicator of tumor volume (or amount) in the liver. Table I shows univariate analyses of clinicopathological features associated with OS. Primary tumor differentiation (p<0.0001), vessel invasion (p=0.0458) and LN metastasis (p=0.0089) were significantly prognostic of 5-year OS. Moreover, non-optimally resectable metastases (p=0.0236), H score (p=0.0265), grade of liver metastases (p=0.0005), resection with non-curative intent (p=0.0017), and MDN (p=0.0006) were metastatic factors significantly prognostic for OS. Table II shows multivariate analyses of clinicopathological features associated with OS. MDN (p=0.0145) and non-curative intent (p=0.0451) were independently prognostic of survival in this patient cohort.
Relationships of MDN to OS and RFS rates. Figure 2a shows the Kaplan-Meier OS and RFS curves for these patients after initial hepatic resection. Patients with MDN ≥30 had significantly poorer prognosis than those with MDN <30, with 5-year OS rates of 23.4% and 63.7%, respectively (p=0.0006; Figure 2a). MDN was also significantly prognostic of RFS, with patients with MDN ≥30 having significantly poorer prognosis than those with MDN <30 (p=0.018; Figure 2b).
Discussion
CRLM may present synchronously in 15-25% of CRC patients, with an additional 30% developing metastases during the course of the disease. Hepatic resection is the only potentially curative treatment for CRLM and may improve patient prognosis (15). Although approximately 20% of patients have potentially resectable metastases and a better chance of long-term survival (16), there is no definitive criteria for selection of resectable CRLM. Thus, defining resectable CRLM and developing treatment strategies are crucially important.
Association between clinicopathological features and 5-year overall survival (OS) rates in patients who underwent surgical resection for colorectal liver metastases (CRLM).
In Japan, there are five criteria for hepatectomy in patients with CRLM: (i) patient ability to tolerate surgery; (ii) primary tumor control or possibility of control; (iii) ability to completely resect the metastatic liver tumor; (iv) absence or possibility of control of extrahepatic metastases; and (v) adequate function of the remaining liver (17). CRLM treatment strategies in Japan do not limit tumor number or size.
Previous reports have shown that the number of tumors, largest tumor diameter, LN metastases of the primary tumor, CA19-9 concentration before hepatic resection and extrahepatic metastatic disease were predictive factors of survival after surgical resection of CRLM (15). These factors resulted in a nomogram prediction of disease-free survival following hepatic resection in patients with CRLM (18), but it was complicated in clinical use because of many risk factors.
Regarding to tumor number or size of CRLM, a previous report showed that the presence of ≥3 tumors and tumor size >8 cm (19) and >10 cm (20), as well as ≥1 tumor and tumor size >5 cm (21), were negatively prognostic of OS. Other studies have reported that the presence of ≥3 tumors and tumor size >5 cm (22) and the presence of ≥4 tumors and tumor size >5 cm (23) were negatively prognostic. However, the significance of the dimensions of metastatic lesions as prognostic factors in CRLM surgery is controversial. Indeed, two independent studies found that the dimensions of metastases were not associated with local recurrence or 5-year survival rates (24, 25). Thus, only the dimensions of metastases cannot be considered an exclusion criterion for surgery, unless they compromise the resection margins or the residual functional parenchyma (24).
Multivariate analysis of factors associated with 5-year overall survival (OS) rates in patients who underwent surgical resection of colorectal liver metastases (CRLM).

Kaplan–Meier curves for (a) overall survival and (b) relapse-free survival in patients with colorectal liver metastases (CRLM) of MDN ≥30 and <30.
On the other hand, in the HCC, The Milan criteria limited the adaptation of liver transplantation to one lesion smaller than 5 cm or up to 3 lesions smaller than 3cm, and it is representing an approximate volume of tumor. Even in the CRLM, simple criteria for resectability especially focusing on tumor volume are required.
In regards to limit of hepatic resection, our institution is most aggressive in the world. In our department, curative hepatectomy was performed whenever possible on patients with CRLM, if the remnant liver volume was ≥40%, even after chemotherapy or hepatectomy. In the criteria of the Japanese Society for Cancer of the Colon and Rectum, H3 liver metastasis was defined as >5 tumors and maximum diameter >5 cm. H3 liver metastasis was judged as not optimally resectable, but it corresponds to MDN ≥25. However, under the condition of aggressive hepatectomy, this study showed that MDN ≥30 was the independent and strong prognostic factor of OS in patients with CRLM who underwent initial hepatectomy.
Based on these results, our department has devised a treatment strategy, in which patients with CRLM, MDN <30 and remnant liver volume ≥40% undergo hepatectomy, whereas those with MDN ≥30 and/or remnant liver volume <40% receive chemotherapy. Patients regarded as non-optimally resectable are treated with FOLFOXIRI plus Bevacizumab, with those showing a sufficient response undergoing subsequent liver resection.
In conclusion, this study showed that MDN was an independent prognostic factor of survival in patients with CRLM. MDN <30 is the optimal surgical criterion of hepatectomy for CRLM.
Footnotes
This article is freely accessible online.
- Received March 3, 2017.
- Revision received March 20, 2017.
- Accepted March 22, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Frailty Can Predict Prognosis After Hepatectomy in Patients With Colorectal Liver Metastasis
- NQO1 as a Marker of Chemosensitivity and Prognosis for Colorectal Liver Metastasis
- Clinical Impact of FOLFOXIRI Aiming for Conversion Surgery in Unresectable Multiple Colorectal Liver Metastasis
- A Score to Identify Patients with Brain Metastases from Colorectal Cancer Who May Benefit from Whole-brain Radiotherapy in Addition to Stereotactic Radiosurgery/Radiotherapy