


Abstract
Aim: To examine the role of radiation therapy (RT) and factors' influence on tumor control for angiosarcoma of the face and scalp (AS-FS). Patients and Methods: We reviewed the records of 14 patients with histopathology proven AS-FS (median age=77 years) who underwent RT between 2000 and 2015. A total dose of 60 to 100 Gy was administered in 24 to 50 fractions. The median calculated biological effective dose (BED) was 93 Gy (range=63.25-120) based on α/β=10. The median follow-up was 16 months (range=5-62). Results: Of the 14 patients, 8 patients (57%) experienced disease recurrence. The median overall survival (OS) rate was 31 months. The 1-year actuarial OS, event-free survival (EFS) and local control (LC) rates were 83%, 71% and 71%, respectively. In univariate analysis, age ≥78years was a significant prognostic factor for LC and OS. BED ≥95Gy was highly correlated with increased LC with borderline significance (p=0.06). Conclusion: Older patients had significantly lower survival rates and higher local recurrence rates than younger patients. The higher radiation dose may have a potential to improve local control for AS-FS.
Angiosarcoma is a rare malignant tumor that most commonly involves the skin and subcutis, particularly that of the face and scalp of elderly people (1). Angiosarcoma of the face and scalp (AS-FS) is an aggressive form with high propensity for local recurrence and early metastatic spread. Previous reports have emphasized the poor prognosis of this disease. Although surgery is the mainstay of treatment, the difficulty in obtaining negative surgical margins and the high frequency of local recurrence remain (1-7). Therefore, most studies assert that surgery combined with radiation therapy (RT) is the optimal approach to eradicate the primary tumor (1, 2, 6, 8-10). However, despite a course of conventional radiation treatment, the majority of patients with AS-FS will ultimately experience local recurrence. Even, the optimal radiation regimen is still unknown due to insufficient data. We conducted a retrospective review of patients with AS-FS treated with definitive RT to evaluate the influence of high-dose RT on local control (LC) and determine whether an elevated RT dose benefits the patients.
Patients and Methods
Between January 2000 and September 2015, a total of 14 patients with AS-FS underwent curative RT at the Department of Radiology, Kyoto Prefectural Medical University Hospital, Kyoto, Japan. All the tumors were histologically diagnosed as angiosarcoma. Clinical information was obtained by a retrospective review of patients' records. The distribution of primary lesions was as follows: 12 on the scalp, 1 on the face and 1 on the ear. A total of 9 males and 5 females with age ranging from 67 to 84 years (median=77) were included. Prior to radiation therapy, all patients were imaged with magnetic resonance imaging (MRI) and/or positron emission tomography/computed tomography (PET/CT). No patients had tumor invasion into the skull and the temporal muscle. Cervical lymph node metastasis and distant metastases were not found at initial diagnosis. Eastern Cooperative Oncology Group performance status (PS), tumor size and number of tumors were evaluated at the start of treatment. Also, in the current study, we analyzed the presence of ulceration, as well as nodules on the primary tumor. The patients' characteristics are summarized in Table I.
Treatment. RT was delivered with 5- to 9-MV electron beam using techniques appropriate to the site of the tumor. Daily fractions of 2.0-3.0 Gy at 5 days per week were used. The median total RT dose was 70 Gy (range=60.0-100.0) with an optimal shrinking field technique at the dose of 50-60 Gy and the median dose per fraction was 2.0 Gy. The primary site was irradiated using the extended local fields. The primary tumor and all satellite lesions with a 3- to 5-cm margin are encompassed by a single or multiple matched appositional electron fields.
Patients' characteristics.
Therapeutic characteristics.
To compare the effects of various treatment protocols with different fraction sizes and total doses, the biological effective dose (BED) was used in a linear-quadratic model (11). Here, the BED was defined as nd(1 + d/α/β), with gray units, where n is the fractionation number, d is the daily dose and α/β is assumed to be 10 for tumors. The median BED was 93 Gy (range=63.25-120.0). The BED was 95 Gy or more in 6 patients and less than 95 Gy in 8 patients. The median BED for the less than 95 Gy and 95 Gy or more subgroups was 75 Gy (range=63.25-94.5) and 102 Gy (range=95.0-120.0), respectively.

Overall survival, event-free survival and local control rate for patients with angiosarcoma of face and scalp treated with radiotherapy (RT).
Details of the other initial treatments are shown in Table II. Surgery was performed in 4 patients (one post-RT planned surgery and 3 before RT) and the resection included the primary tumor along with 3- to 5-cm margins. Surgical margins at the primary tumor were positive in 3 patients, negative in 1 patient. All patients but 2 were receiving chemotherapy using docetaxel concurrent with RT. Docetaxel was given at 20-40 mg/m2 biweekly or triweekly and also continued same regimen after RT until disease progression or unacceptable toxicity was reached. Adjuvant immunotherapy using recombinant interleukin-2 (rIL-2) was combined before and after RT in 6 patients via intratumoral injection. All patients were enrolled in this study after obtaining written informed consent prior to treatment in accordance with the guidelines of the Institutional Review Board. Patients were followed-up every month during the first six months and every 3-6 months thereafter. The median follow-up time was 15 (range=3-60) months for all patients. LC, event-free survival (EFS) and overall survival (OS) rates were examined. Acute and late toxicities were scored according to the Common Terminology Criteria of Adverse Events, version 3.0 (12).
Statistical analysis. All statistical analyses were performed using the Stat-view 5.0 statistical software (SAS Institute, Inc., Cary, NC, USA). Survival data and cumulative incidences were estimated by the Kaplan–Meier method and examined for significance using the log-rank test. Cut-off values were set as the average or median value of each variable unless otherwise stated. We arbitrary set a cut-off value of biological effective dose at 95. All analyses used the conventional p<0.05 level of significance.
Results
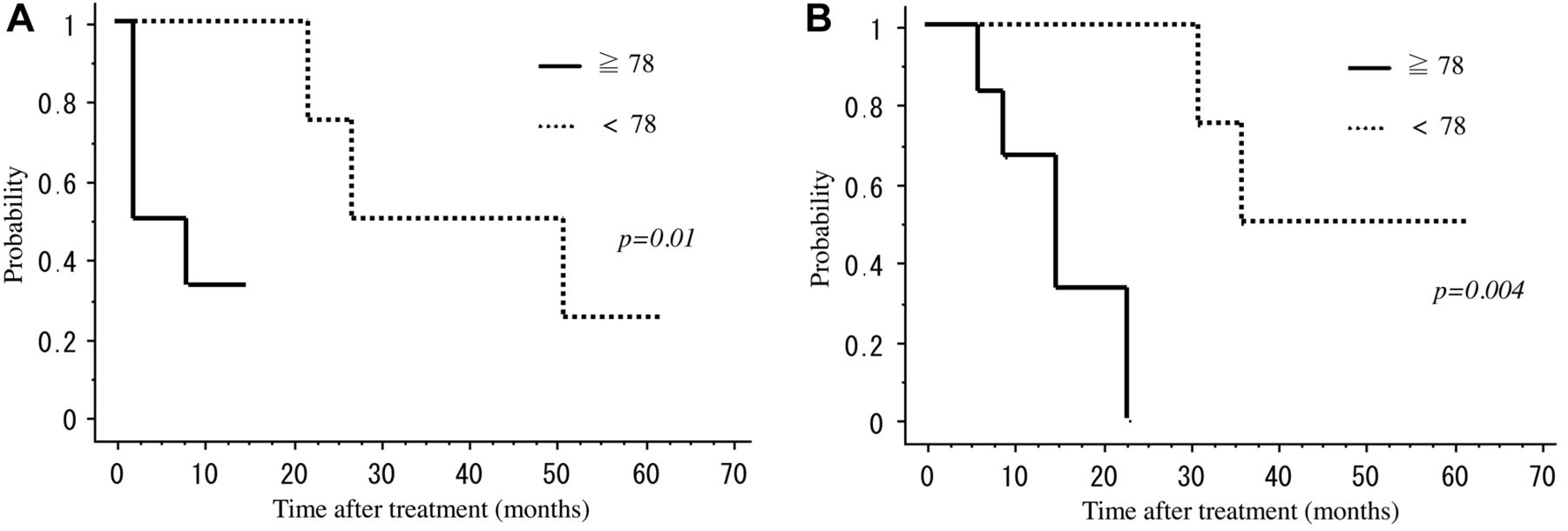
All patients completed RT without an interval for more than 1 day. The median follow-up for all patients was 16 months calculated from the date after RT (range=5-62). The median OS time was 31 months. The 1-year actuarial OS rate and EFS rate were 83% and 71%, respectively (Figure 1). The cause of death was tumor progression in 5 patients, intracerebral hemorrhage in 1 patient; the expected median survival time was 31 months. Recurrence was observed in 8 cases. Local recurrence alone, distant metastasis alone and both of these were confirmed in 3, 1 and 4 patients, respectively. Local recurrence was developed in-field in all cases and the sites of distant metastasis in all cases were in the lung. The 1-year actuarial LC rate was 71% (Figure 1). Table III summarizes the prognostic factors. Univariate analysis revealed that age at presentation was significant factor affecting LC and OS (Table III). Patients who were aged 77 years and younger at presentation had a significantly better 1-year LC rate (100%) and OS rate (100%) compared with patients older than 78 years (33%, p=0.01 and 67%, p=0.004, respectively) (Figure 2A and B). Total BED of 95 Gy or more also was found to be an important prognostic factor that improved LC; however, this was not of statistical significance (p=0.06, Figure 3). None of the patients treated with BED of 95 Gy or more experienced local recurrence and distant metastasis.

Local control rate and overall survival rate by age. A. Local control rate. Patients who were age 77 years and younger at presentation had 100% local control rate at 1 year, whereas that of the older counterpart was 30% (p=0.01). B. Overall survival rate. Patients who were age 77 years and younger at presentation had 100% local control rate at 1 year, whereas that of the older counterpart was 67% (p=0.004).
Of the 12 patients treated with concurrent chemoradiotherapy, two patients could not receive chemoradiotherapy because of medically contraindication; these patients experienced local progression and died of recurrent disease.
Toxicity. Thirteen cases developed acute toxicity with grade 1-2 skin reactions. Grade 3 skin reaction and grade 3 leukopenia were observed in 1 patient and 3 patients, respectively. Treatment interruption over 1 week due to acute toxicities was not experienced. Non-hematologic grade 3-4 acute toxicity requiring treatment interruption was not observed. Two patients developed grade 4 late toxicities. A 73-year-old woman with angiosarcoma located on the scalp received postoperative RT with 70 Gy at 2.5 Gy per fraction once daily and suffered from grade 4 tissue ulceration surrounding the tumor bed, which required reconstructive surgery. A 67-year-old male patient with a large tumor located on the left face received RT with 100 Gy at 2 Gy per fraction once daily and suffered from grade 4 corneal fistula, although customized lens shielding –consisting of a 1-cm-thick lead shield suspended 1 cm above the cornea to provide shielding to the crystalline lens during the RT– was used.
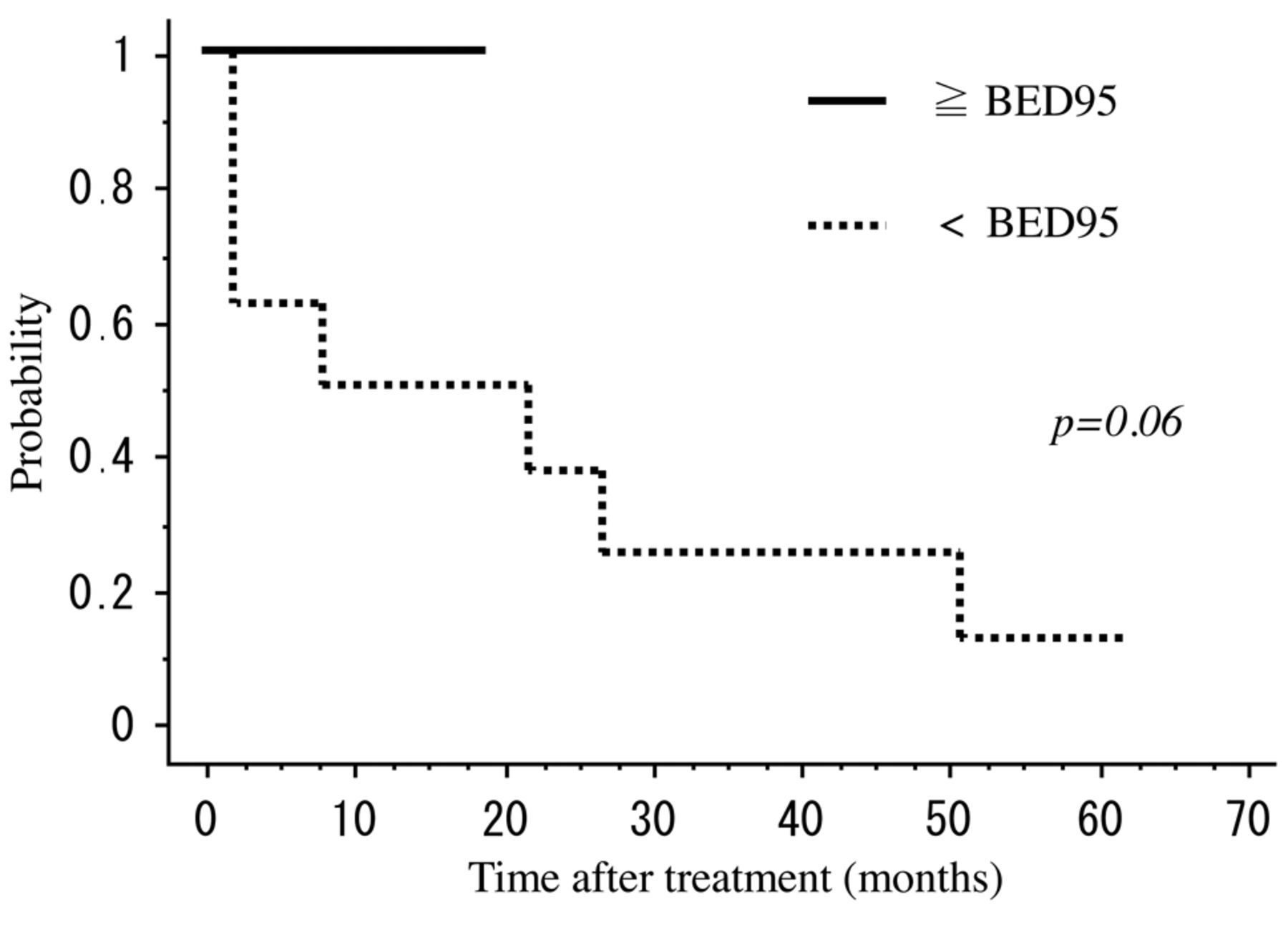
Local control rate. Patients treated with biological effective dose (BED) greater than 95 Gy or more had 100% local control rate at 1 year, whereas that of the lower counterpart was 50% (p=0.06).
Univariate analysis of potential prognostic variables and survival times.
Discussion
Angiosarcomas are rare, aggressive tumors of vascular origin that often present in the head and the neck and carry a poor prognosis, particularly when located on the scalp. In general, surgery is the standard treatment for AS-FS. Given, however, the potentially diffuse nature of involvement of the scalp or face by the primary tumor and the difficulty in obtaining negative margins, most studies assert that surgery combined with RT is the optimal approach to eradicate the primary tumor (1, 2, 6, 8-10). Docetaxel is well-known as having a radiosensitising effect (18). Several recent reports have stressed the importance of rIL-2 in the treatment of AS (4, 21, 22). Ohguri et al. (4) performed curative RT plus rIL-2 immunotherapy and achieved a median OS of 36.2 months, which was an improvement over previous reports. It is possible that the use of chemotherapy or immunotherapy might enhance the efficacy of RT more than a dose escalation; however, evidence about optimal methods to combine with RT is lacking for this disease in particular. Despite intensive therapies, local recurrences in patients with AS-FS are frequent, ranging in frequency from 35% to 86% (2-4).
Several previous studies have suggested prognostic factors associated with tumor size, tumor type, age, PS and radiotherapy use in patients with AS-FS (2.3 13-16). Unfortunately, all previous studies, looking at definitive RT for AS-FS, have yielded unsatisfactory outcomes for both local control and survival. Moreover, there is no clear evidence about effective radiation dose to control local disease. In previous reports, increased total radiation dose tended to have a favorable impact on local control (11). Several authors generally recommend approximately 50-70 Gy for treatment of AS-FS (2, 14, 17, 18), whereas ore recent reports suggested that total doses of 70 Gy or more in conventional fractionations are effective in preventing local recurrence in patients with macroscopic disease (16, 19, 20). The differences in dose-fraction schedules in published data were various; it is meaningful that an effective BED was suggested because the optimal dose-fraction schedule of RT for AS-FS is not known. In our current study, local recurrence occurred in 7 of 8 patients treated with BED for less than 95 Gy, while none of 6 patients treated with BED of 95 Gy or more had local recurrence, and BED was potential prognostic factors for LC (Figure 3). Our study also found that local recurrence correlated with the development of distant metastatic disease (Table IV) and dose escalation at the local tumor might be the focus of developmental therapeutic strategies for AS-FS to improve not only local control but also distant metastatic disease.
Outcomes for patients.
Advanced age was associated with a poor prognosis in the current study. Patients who were older than 78 years at presentation had a significantly worse LC and OS compared with younger patients (Figure 2A and B). Wilson-Jones was the first to distinguish a unique form of AS-FS of elderly individuals (23). It has been noted that this form of angiosarcoma, known as senile angiosarcoma or malignant angioendothelioma, carries a particularly poor prognosis (23, 24). The reason for this association remains unclear but may be due to different tumor biology in a relatively more immunocompromised, elderly host. Pawlik et al. reported that patients older than 70 years were significantly predictive of shorter time to recurrence (6). More studies clearly are needed to elucidate the correlation between advanced age and the poorer prognosis seen in older patients with AS-FS.
Tumor size has consistently been shown to be a predictor of outcome in this disease, with larger tumor size being associated with inferior LC (3, 4, 9, 10, 25). Although tumor size was not an independent prognostic factor in our study, large tumor size (>5 cm) correlated with age older than 78 (Table IV) and might tend to decrease LC rate. In our study, four of 6 patients who had large tumor (>5 cm) developed local recurrence and were treated with BED for the less than 95 Gy. Remaining 2 patients with large tumor treated with BED of 95 Gy or more achieved LC (Table IV).
We experienced a postoperative radiation case with grade 4 skin ulceration as late toxicity. Total radiation dose in this case was 70 Gy per 28 fractions (BED=87.5 Gy). Thus, if not combined with surgery, we thought dose escalation was needed, especially for patients with large tumor >5 cm, targeting the BED of 95 Gy or more.
There are several limitations left in our study, specifically with respect to the limited number of patients, retrospective nature of the data collection and short follow-up period. Thus, further studies, including larger number of patients with longer follow-up period, are needed to investigate the role of high dose RT for AS-FS.
In conclusion, age older than 78 years was a significant prognostic factor for LC and OS. BED of 95 Gy or more may have a potential to improve LC for AS-FS.
Footnotes
Conflicts of Interest
The Authors declare that they have no competing interests.
- Received July 1, 2016.
- Revision received July 20, 2016.
- Accepted July 21, 2016.
- Copyright © 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}
{kind=link}