


Abstract
Background/Aim: Radiation-induced heart disease (RIHD) is a concern during radiotherapy. For its comprehensive study, an in vivo selective heart irradiation model was developed. Materials and Methods: Sprague-Dawley rats were irradiated with 50 Gy and functional imaging, biochemical (circulating growth differentiation factor-15 (GDF-15), transforming growth factor-beta (TGF-beta) and morphological (picrosirius red staining of the heart) objectives were tested. Results: Signs and symptoms of RIHD occurred >12 weeks after irradiation with tachypnea, systolic and diastolic dysfunction, cardiac hypertrophy and body development retardation. Plasma GDF-15 was increased 3, 12 and 26, while plasma TGF-beta was increased 12 weeks after irradiation. At autopsy, extensive pleural fluid was found in the irradiated animals. Interstitial fibrosis could be reliably detected and quantified in irradiated hearts after a follow-up time of 19 weeks. Conclusion: The studied parameters could be used in future experiments for testing protective agents for prevention of radiation heart injury.
Radiotherapy is an integral part of anticancer therapy. Nonetheless, a substantial number of irradiated patients may suffer from late side-effects that cause deterioration of quality of life, extra cost to health care or lead, occasionally, to fatal outcome. Among these, cardiotoxicity is one of the most important concerns in oncology practice (1-3). Radiation-induced heart disease (RIHD) is dose-dependent and develops many years after radiotherapy of thoracic tumors (4-7). Although modern radiotherapy techniques significantly attenuate the dose to the heart, in many cases, the whole heart or a part of it still receives a dose sufficient to cause RIHD (1, 8).
The study of the pathomechanisms of RIHD, the identification of its early predictors and its prevention by administration of protective agents are relevant research perspectives, studied under both experimental and clinical research conditions (3, 9). Although different experimental approaches have been tested to model the clinical scenario of RIHD, the results obtained so far are rather contradictory and only few of the in vivo models applied selective heart irradiation. Most experience was collected in murine models, despite that, in these species, the different structures of the heart show less radiosensitivity than in larger animals. Using Wistar rats, Lauk et al. (10) demonstrated ventilatory failure accompanied with pleural effusion that developed earlier and in a more severe form at a higher (i.e., 20-40 Gy) than a lower (<20 Gy) heart dose. Yeung et al., >6 months after the delivery of a single dose of 30-50 Gy to the heart, experienced dose-dependent vascular damage and decreased cardiac output in Sprague-Dawley rats, but no or insignificant fibrosis (11). Sharma et al. developed an image-guided irradiation technique in Sprague-Dawley rats and, after the delivery of 21 Gy to the heart, found myocardial degeneration and fibrosis (12).
Although signs and symptoms of RIHD develop many years after radiation exposure, early predictive markers would be useful. Transforming growth factor-beta (TGF-beta) and growth differentiation factor-15 (GDF-15) belong to the TGF-beta/bone morphogenetic protein (BMP) superfamily involved in the regulation of cell proliferation, differentiation, apoptosis, inflammation and tumorigenesis (13-15). TGF-beta is a key cytokine implicated in the development of radiation injury of various tissues (16, 17). In cardiovascular diseases, GDF-15 has great potential as a biomarker (13, 15, 18).
We developed a model appropriate for the comprehensive study of RIHD with heart functional, imaging, biochemical and morphological end-points. A rat model applying high-dose selective heart irradiation and relatively long follow-up was setup.
Materials and Methods
The experiments performed conform to the National Institutes of Health Guide for the Care and Use of Laboratory Animals (NIH Pub. No. 85-23, Revised 1996) and were approved by the local ethics committee of the University of Szeged. All institutional and national guidelines for the care and use of laboratory animals were followed.
Animals. Male Sprague-Dawley rats of 180-200 g were used. The animals were housed three per individually ventilated cages (Sealsafe IVC system; Buguggiate, Italy) in a temperature-controlled room with 12 h:12 h light/dark cycles. Standard rat chow supplemented with 5% fat (Innovo Kft., Gödöllő, Hungary) and tap water were supplied ad libitum (19).
Experimental setup. Two preliminary experiments focused on dose finding and optimum timing of tests for the pre-specified end-points. In the first experiment, 5 groups of 2 animals each were irradiated with 0 Gy (control), 20 Gy, 25 Gy, 30 Gy and 40 Gy, respectively, and were observed 14 weeks thereafter. In the second experiment, 4 groups of 5 animals each were irradiated with 50 Gy and the observation time lasted for 14, 18, 22 or 26 weeks. An unirradiated group of the same size was observed for 26 weeks. In these preliminary experiments, weight gain, ventilatory symptoms and animal loss were studied. Circulating cytokine tests and echocardiography were performed at weeks 0, 3, 8, 12 and 26; heart pathology was studied with special attention to radiogenic abnormalities.
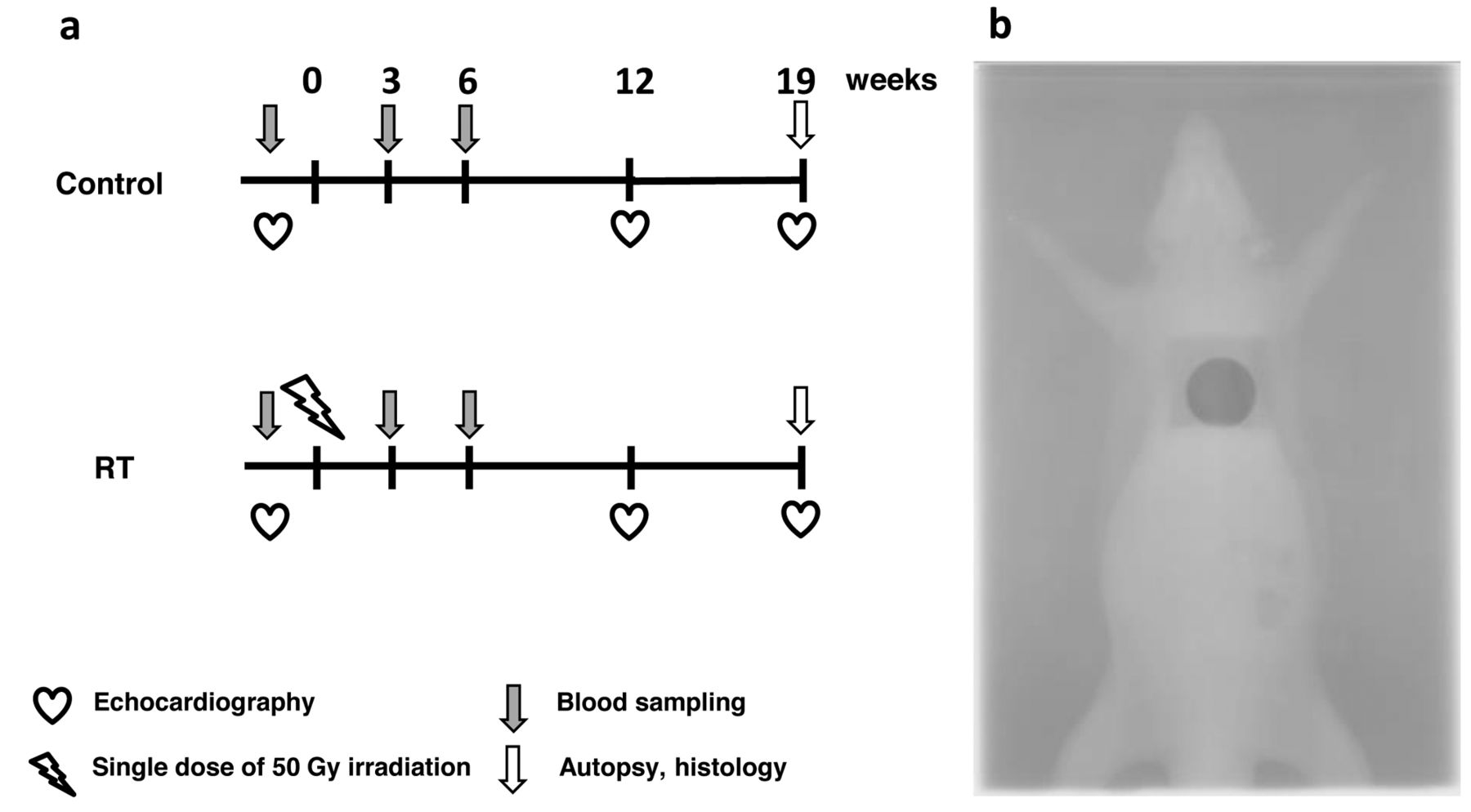
In the third experiment, the animals were divided into control and irradiated groups (n=12 each). In the irradiated group, a single dose of 50 Gy was delivered to the whole heart. Body weight was measured weekly in both groups. Cardiac morphology and function were assessed by transthoracic echocardiography and electrocardiogram (ECG). One-ml blood samples were carefully collected with 25 G needles from the tail vein into heparinized Eppendorf tubes (Figure 1). Plasma was separated by centrifugation at 4,460 rpm, 10 min, 4°C and stored until measurements at −70°C.
Despite the initial plan to follow-up the animals for 24-28 weeks, the experiment was terminated because of status deterioration at week 19.
Heart irradiation. Based on the computed tomography (CT) morphology of the heart in 3-month-old Sprague Dawley rats in the supine position, the irradiation was carried out with a single 2 cm circular 6 MeV electron field. Dose distribution measurements were carried out using a water phantom with a pinpoint ionization chamber (PTW, Freiburg GmbH, Germany). Dose was prescribed as a mean dose to a 1 cm spherical volume 3 mm below the body surface.
The rats were anesthetized with sodium pentobarbital (Euthasol; i.p. 40 mg/kg; Produlab Pharma b.v., Raamsdonksveer, The Netherlands), then fixed in supine position to a flat surface couch. The radiation dose was delivered with a Primus linear accelerator (Siemens Healthcare GmbH, Erlangen, Germany) at a dose intensity of 5 Gy/min if the appropriate position of the animal was proved by the verification film obtained with the radiation beam.
Transthoracic echocardiography. Echocardiography was carried out at weeks 0, 12 and 19. The rats were anesthetized with 2% isoflurane (Forane, AESICA, Queenborough Limited Kent, UK), the chest was shaved and the animal was placed in supine position onto a heating pad. Echocardiography was performed as described previously (20). Moreover, maximal flow velocity and pressure gradient through the left ventricular outflow tract were assessed by continuous-wave Doppler across the aortic valve from the parasternal long axis view. Diastolic function was assessed using pulse-wave Doppler across the mitral valve from the apical four-chamber view. Early (E) and atrial (A) flow velocity, as well as their ratio, provide an indication of diastolic function. The septal mitral annulus velocity e' was assessed by tissue Doppler imaging as an early indicator of left ventricular diastolic dysfunction. The mean values of three measurements were calculated and used for statistical evaluation.
Measurement of GDF-15 and TGF-beta in plasma. Levels of plasma GDF-15 and TGF-beta1 protein were determined in blood plasma taken from the rats the day before and 3, 8, 12 and 26 weeks (preliminary experiment) after the irradiation. Confirmatory measurement of GDF-15 concentrations was performed in the final experiment as indicated in Figure 1. Cytokine levels were determined using the Quantikine Rat GDF-15/TGF-beta1 ELISA kit (R&D Systems, Minneapolis, MN, USA) according to the manufacturer's instructions.
Tissue harvesting. In the third experiment, at week 19, rats were anesthetized with sodium pentobarbital, the heart was excised and perfused according to Langendorff as described (20, 21). The hearts were weighed and a cross section of the whole heart at the ring of the papillae was cut and fixed in 10% buffered formalin for histological analysis. Pleural fluid was collected and measured, whereas all other organs were weighed.
Histology and computerized image analysis of fibrosis in the heart. Five-μm paraffin-embedded transverse cut sections of the formalin-fixed subvalvular area of the ventricles were stained with both hematoxylin-eosin and picrosirius red for detecting collagen (12). In the preliminary experiments, picrosirius red staining was semiquantitatively evaluated by 2 independent pathologists blinded to the treatment received. Based on these results, in the third experiment, a computerized image analysis method was developed. Histological slides were scanned with a Pannoramic P250 scanner (3D-Histech, Budapest, Hungary) and digital images at magnification of ×1.5 (whole transection area) and ×20 (3 specified areas of the left ventricle: anterior, lateral and posterior wall, septum and lateral wall of the right ventricle) were captured. Medium-size vessels and their perivascular connective tissue sheet, the subepicardial and subendocardial areas were avoided. The images were analyzed with an in-house program that uses two simple color filters for determining the proportion of red in the heart. The first filter is used for detecting red portions of the picture. For each Red-Green-Blue (RGB) pixel making up the image, the program calculates the color of the pixel in Hue-Saturation-Luminance (HSL) color space. The second filter excludes any white (empty) or light grey (residual dirt on the slide) pixel from further processing using simple RGB threshold. In this way, the program groups each pixel into one of two sets: pixels considered red (connective tissue and fibrosis) and pixels considered neither red, nor white, nor grey (i.e., green, corresponding to cardiac muscle). Dividing the number of elements in the first set by the number of elements in both sets gives the proportion of the connective tissue compartment of the heart.

Experimental setup. Sprague-Dawley rats after sham or selective heart irradiation were examined by means of echocardiography, blood tests for circulating inflammatory cytokines and pathological studies focusing on the heart (A). A typical verification image of selective heart irradiation is shown (B).
Statistical analysis. Statistical analysis was performed using Sigmaplot 12.0 for Windows (Systat Software Inc., Chicago, IL, USA). All values are presented as mean±SEM, p<0.05 was accepted as statistically significant.
Results
Preliminary experiments. In the first preliminary experiment, heart irradiation with doses of 20-40 Gy caused no symptoms or echocardiography changes during the 14 weeks of observation; also, no animal loss occurred despite the apparent growth retardation due to irradiation. The radiation dose of 50 Gy, in the next experiment, caused tachypnea, abdominal breathing and heart functional changes with arrhytmias, but only after the observation time of 14 weeks; GDF-15 elevation occurred at weeks 3, 12 and 16, TGF-beta concentrations were continuously elevating during the observation period until the maximum value at week 12 (Figure 2). Four animals were lost during anesthesia for echocardiography, 1 at week 18 and 3 at week 22. Hence, a radiation dose of 50 Gy and a follow-up time of a minimum of 24 weeks were chosen for the final experiment.
Clinical symptoms and survival. Although body weight constantly increased throughout the observation period, the irradiated animals showed significantly lower weight gain as compared to the control animals (Figure 3). After week 12, irradiated animals developed tachypnea and abdominal breathing and, after week 16, 2 animals in the irradiated group died. Due to the poor performance status of the irradiated animals, the experiment was terminated at week 19.
Transthoracic echocardiography. In the third experiment, transthoracic echocardiography was performed at weeks 0, 12 and 19. Left ventricular systolic and diastolic anterior wall thickness in the irradiated rats was increased at weeks 12 and 19 as compared to both the baseline values and that in the control animals (Figures 4A and 5). Likewise, in irradiated rats, diastolic septal wall thickness was increased at week 19 compared to the initial values or to the control group. While left ventricular end systolic and end diastolic diameters increased by time in control rats indicating normal heart growth, these parameters in the irradiated rats failed to increase or decreased, thus indicating retarded heart growth (Figure 4C). Increased anterior and septal wall thickness and decreased left ventricular diameters of the irradiated hearts point to the presence of left ventricular hypertrophy (Figures 4C and 5). Echocardiography performed at week 19, in addition, indicated the presence of arrhythmias.

Plasma growth differentiation factor-15 (GDF-15) levels in 2 consecutive experiments (A and C) and plasma transforming growth factor-beta (TGF-beta) levels (B) in unirradiated controls vs. animals after selective heart irradiation. The data obtained were analyzed by two way ANOVA and Sidak Post Hoc tests comparing data in the irradiated group with the control group (mean±SEM, *p<0.05, **p<0.01), n=5/group.

Body weight in unirradiated and irradiated animals. All data were analyzed by unpaired t-test comparing data in the irradiated group with the control group (mean±SEM, p<0.05 at all time points), n=10-12/group.
Irradiated animals demonstrated increased fractional shortening as compared to controls, at week 19 (Figure 6A). Physiological heart rate decrease, due to aging apparent in control rats, was lacking in irradiated animals (Figure 6B). Isovolumic contraction time was significantly increased in irradiated animals at weeks 12 and 19 as compared to the baseline or to that in control rats at week 19 demonstrating impaired systolic function after irradiation (Figure 6C). Other systolic parameters, maximal flow velocity and pressure gradient through the left ventricular outflow tract were significantly decreased in the irradiated rats as compared to controls at weeks 12 and 19 (Figures 6D-E). The ratio of the early flow velocity E and the septal mitral annulus velocity e' was significantly increased in the irradiated rats as compared to the baseline values or to that of controls at week 19, indicating diastolic dysfunction (Figure 6F).

Left ventricular morphology as assessed by echocardiography. The parameters were analyzed by two-way ANOVA and Holms-Sidak Post Hoc tests comparing data in the irradiated group with the control group (mean±SEM, *p<0.05 compared to control group within the same time point, #p<0.05 compared to initial values within the same group), n=10-12/group. AWTs, Systolic anterior wall thickness; AWTd, diastolic anterior wall thickness; SWTs, systolic septal wall thickness; SWTd, diastolic septal wall thickness; LVESD, left ventricular end systolic diameter; LVEDD, left ventricular end diastolic diameter.
Circulating GDF-15. The early peak of GDF-15, 3 weeks after the irradiation, was confirmed (Figure 2C).
Autopsy. At autopsy, the most common finding was the presence of extensive pleural fluid (11.3±1.7 ml, n=10) in irradiated animals. Neither abnormal macroscopic heart changes (including the large vessels, the valves, the coronary arteries etc.) nor sign of radiation pneumonitis nor lung fibrosis were visible, confirming the selectivity of heart irradiation. In the irradiated group, the tibia length and the weight of various organs, including the heart, was significantly smaller than in the control group (1.3±0.06 vs. 1.7±0.07 g, p<0.05).
Histology and computerized image analysis of fibrosis in the heart. Conventional morphological examinations of the pericardium, myocardium, vessels, perivascular, subendo-cardial, subepicardial areas and the coronary arteries, or the lungs, failed to reveal abnormalities in irradiated rats.
In the preliminary experiments, picrosirius red staining of the heart sections failed to detect fibrosis in animals irradiated with a dose of <40 Gy. In the 40-Gy heart irradiation group, slight but consistent fibrosis was visible after a follow-up of 26 weeks. In the final experiment, 50 Gy dose induced readily detectable collagen deposition appropriate for quantification after a follow-up time of 19 weeks. Our computer-assisted quantitative method indicated significant fibrosis in all parts of the heart (Figure 7).

Representative M-mode echocardiographic images in cross section. Anterior wall, left ventricular diameters and inferior wall in systole and diastole represent 5 cardiac cycles at week 0, 12 and 19 in a control and an irradiated animal. AWTs, Systolic anterior wall thickness; AWTd, diastolic anterior wall thickness; SWTs, systolic septal wall thickness; SWTd, diastolic septal wall thickness; LVESD, left ventricular end systolic diameter; LVEDD, left ventricular end diastolic diameter.
Discussion
The reported rat model provided drastic functional and morphological changes, some of them already present at 12 weeks. The time course of radiogenic, morphological and functional changes was similar to that in other studies (4, 22, 23). Interstitial collagen deposition is thought to be progressive (4, 22, 24); our experiments indicate that no abnormality occurs earlier than 5-6 months post-irradiation, even if a large dose is applied. Lately, we observed chronic cardiovascular and ventilatory insufficiency, partly due to pulmonary toxicity related to heart irradiation (25). It is thought that the pathomechanism of RIHD in humans consists of progressive atherosclerosis of the coronary arteries due to endothelial damage, as well as diffuse injury of the myocardium (1, 6). The injury to the macrovasculature is difficult to test due to the absence of risk factors for coronary artery disease in experimental animals. We fed the animals with lipid-rich chow but, despite the large radiation dose, no signs of macrovasculature changes were seen. For the detection of the loss of capillaries, no special staining was used. Conventional morphological methods, including hematoxylin and eosin or the Crossman trichrome stain of connective tissue, failed to reveal differences between unirradiated and irradiated animals' hearts even after the use of a dose of 40 Gy. Using the picrosirius red/fast green staining method, after the delivery of 40 Gy and a follow-up time of 22-26 weeks, there was slightly more apparent interstitial fibrosis in irradiated hearts. Since interstitial fibrosis is a major final end-point of radiogenic damage of all risk organs, a computer-assisted quantitative method adequate for future radiobiology investigations was developed.
Pleural fluid is a well-known consequence of heart irradiation due to -and explained by-radiation pericarditis: the pericardium in rodents is interconnected with the pleural space and the origin of pleural fluid is thought to be pericardial fluid (4). Pleural fluid, related to high-dose irradiation, was absent below the dose of 20 Gy both in our hands and the literature (23, 26). In our experiments, no histological abnormalities related to pericardial damage were seen, despite the fact that the pericardium was exposed to irradiation.

Left ventricular function as assessed by echocardiography. The parameters were analyzed by two-way ANOVA and Holms-Sidak Post Hoc tests comparing data in the irradiated group with the control group (mean±SEM, *p<0.05 vs. control group within the same time point, #p<0.05 vs. week 0 within the same group), n=10-12/group. FS, Fractional shortening; HR, heart rate; IVCT: isovolumic contraction time; LVOT vmax, left ventricular outflow tract maximal flow velocity; LVOT PGmax, left ventricular outflow tract maximal pressure gradient; E/e', ratio of the early flow velocity (E) and the septal mitral annulus velocity e'.
We intended to find early markers that could predict consequent damage after heart irradiation. GDF-15 is related a series of heart abnormalities (26-32). We think that, GDF-15 elevation, 3 weeks after the irradiation, reflected an early stress-response, while its increase at weeks 12 and 26 was rather a consequence of heart failure.
Fibrosis is a self-stimulating vicious circle resulting in the progressive nature of the process. The blockade of the key mediator TGF-beta may prevent or mitigate fibrosis (33). In the present model, increased values of TGF-beta, at week 12, predicted fibrosis in yet asymptomatic animals. In future experiments, GDF-15 and TGF-beta determination could serve as early parameters for testing radioprotective agents.
We believe that our animal model will turn appropriate for testing protective agents for the prevention of RIHD.
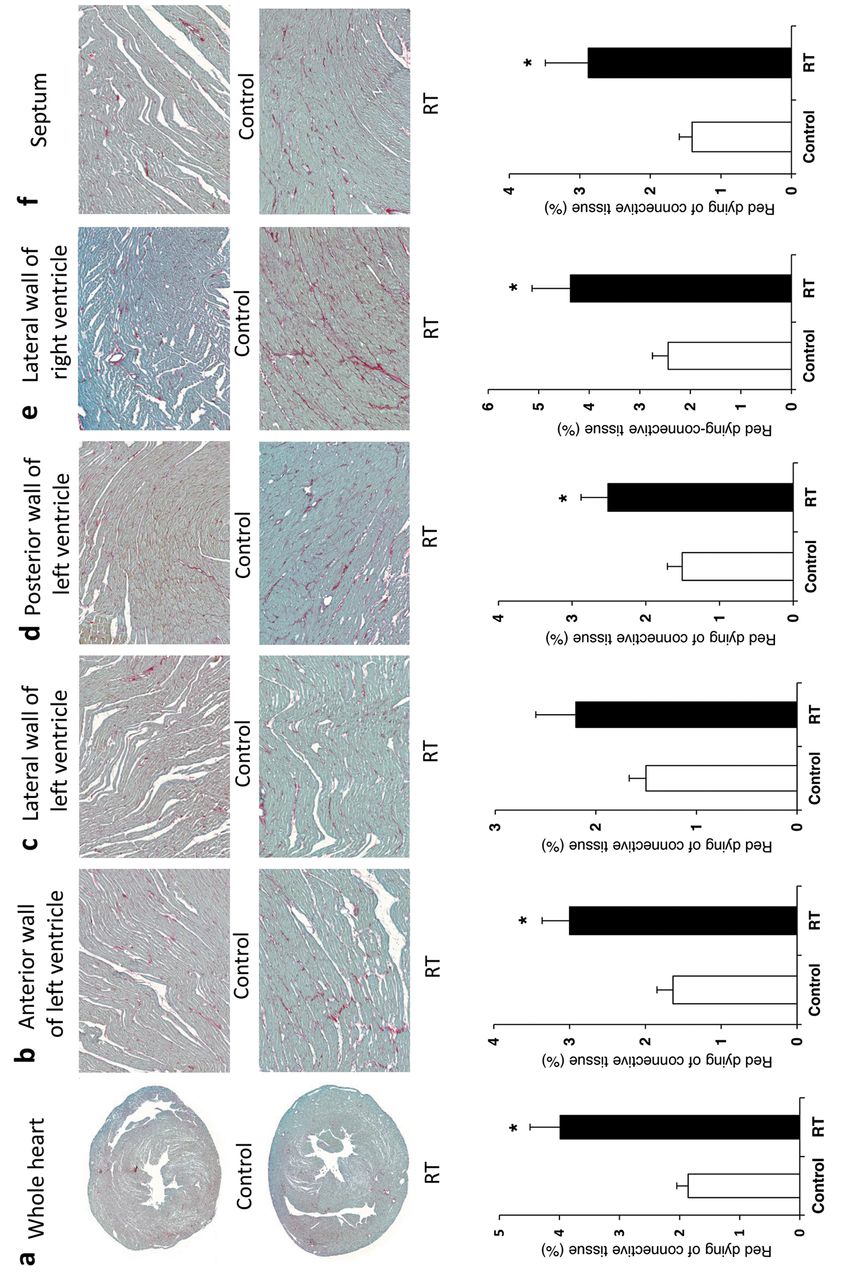
Representative images of picrosirius red staining indicating fibrosis of unirradiated and irradiated heart sections of the whole heart (magnification ×1.5) (A), the anterior (B), lateral (C), posterior wall (D) of the left ventricle, lateral wall of the right ventricle (E) and the septum (magnification: ×20) (F); the corresponding quantitative data on fibrosis are indicated below. The parameters were analyzed by one way ANOVA and Sidak Post Hoc tests comparing data in the irradiated group with the control group (mean±SEM, *p<0.05), n=10-12/group.
Acknowledgements
The excellent technical support of Márton Pipicz MD, Péter Bencsik MD, László Bodor and Róbert Motzwickler is greatly acknowledged.
Footnotes
Conflicts of Interests
The Authors declare that no competing interest exists.
- Received June 9, 2016.
- Revision received July 4, 2016.
- Accepted July 5, 2016.
- Copyright © 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.