


Abstract
Aim: To evaluate the impact of physical training on central hemodynamic parameters and elasticity of large arteries in hypertensive patients. Patients and Methods: A total of 129 hypertensive patients were divided into two groups: group A followed lifestyle changes and physical training; and group B acted as a control group; seven parameters were recorded: Pulse wave velocity (PWVao), systolic blood pressure (SBP), diastolic blood pressure (DBP), pulse pressure (PP), central aortic systolic blood pressure (SBPao), aortic diastolic blood pressure (DBPao), and central aortic pulse pressure (PPao). Results: The difference between values at 4 months and baseline (Δ) were as follows: ΔPWVao was −1.02 m/s (p<0.001) versus 0.17 m/s (p=0.035), ΔSBPao was −9.6 mmHg (p=0.009) versus 1.6 mmHg (p=0.064), and ΔPPao was −6.8 mmHg (p<0.001) versus 3.2 mmHg, (p=0.029) in group A versus B, respectively. Conclusion: Exercise training improves SBP, PP, SBPao, PPao and may delay arterial ageing.
Death caused by cardiovascular diseases ranks first in Europe (1). Among cardiovascular diseases, hypertension is the most frequent pathology diagnosed by practitioners (2). The prevalence of arterial hypertension for Europe overall is 30-45%, and has continuously increases with increasing age (1-3). In Romania, the prevalence is about 40.1% according to the SEPHAR study (4). Current trends for a better evaluation and classification of arterial hypertension include the assessment of subclinical changes of arterial blood vessels. The latest guidelines concerning hypertension management emphasized on the importance of evaluating asymptomatic organ-damage parameters for future cardiovascular prognosis (5). These parameters include: pulse pressure (PP), left ventricular hypertrophy, pulse wave velocity (PWV), intima-media thickness (IMT), ankle brachial index and renal damage.
The blood vessel status of hypertensive patients can be assessed by several parameters that have a direct impact on cardiovascular mortality. Current European Society of Cardiology/European Society of Hypertension (ESC/ESH) guidelines promote, along with previously mentioned parameters, other key players of hypertension with similar predictive value, availability, reproducibility and cost–effectiveness as markers of organ damage such as: arterial aortic pressure, aortic rigidity, and carotid IMT. Some data reported that arterial rigidity is not fully evaluated and is less used as an endpoint for some clinical studies (6).
Physical training has several benefits on the heart and blood vessels but the precise, intrinsic mechanisms of the body adjustments to exercise are less clear.
Current clinical guidelines (2) have extensive recommendations concerning lifestyle changes for patients with hypertension accompanied by sustained and regular physical training.
A large meta-analysis of randomized controlled trials has shown that aerobic endurance training reduces resting systolic blood pressure (SBP)/diastolic blood pressure (DBP) by 3.0/2.4mmHg overall, and even by 6.9/4.9 mmHg in hypertensive participants (1, 7). Even regular physical activity of lower intensity and duration has been shown to be associated with a 20% decrease in mortality in cohort studies (1-3), and this is also the case for measured physical fitness (5). Lifestyle changes, particularly weight loss and physical exercise, are recommended to all individuals as Class I, level A of evidence (1). Regular exercise is recommended, i.e. at least 30 min of moderate dynamic exercise on 5 to 7 days per week.
There are still a few gaps in the current ESC/ESH 2013 Guidelines regarding the effects of physical training or other lifestyle changes on reducing mortality and morbidity caused by cardiovascular diseases. Some unanswered questions may arise from these facts such as: (i) whether the known lifestyle measures are able to reduce BP, and consequently, also the morbidity and mortality in hypertensive patients, and (ii) whether central BP be added to cardiovascular event prediction in untreated and treated hypertensive patients.
Based on the previous controversial data, we aimed to study the impact of personalized, specific physical training and lifestyle changes on selected peripheral and central hemodynamic parameters and also on arterial stiffness.
Materials and Methods
Patients, inclusion and exclusion criteria, design of the study groups. A total of 129 hypertensive patients were included. They were selected according to the following criteria: controlled BP values of up to 140/90 mm Hg, stable medication for at least 30 days before the beginning of the study, age between 40 to 70 years, and good communication skill of the patient with the doctor. We established as exclusion criteria any condition non compatible with physical training, uncontrolled blood pressure, other cardiovascular disease such as ischemic heart disease, significant valvular pathology (greater than grade II), cardiomyopathy, congenital heart disease, myocarditis, pericarditis, and lack of cooperation. All these patients were treated and were instructed according to the ESC/ESH guidelines regarding hypertensive patients (2).
After inclusion, we divided the patients into two groups: group A=63 patients, who gave their informed consent to be involved in a physical training program, and group B with 66 patients who refused to participate in the physical training program but gave their consent to be enrolled in the present study as part of the control group.
We assessed the hemodynamic parameters and arterial stiffness at baseline and at 4 months in both groups. Patients in group A performed an exercise test at baseline in order to evaluate the exercise capacity and to include them in the rehabilitation program.
Methods, materials and evaluated parameters. For parameter evaluation, we used an arteriograph device (TensioMed, Budapest, Hungary). The system is equipped with software able to measure several hemodynamic parameters and arterial stiffness. The vascular parameters we aimed to assess in this study were: SBP, DBP, PP, aortic systolic bood pressure (SBPao), aortic pulse pressure (PPao), aortic pulse wave velocity (PWVao). These parameters were evaluated at the beginning of the study and at 4 months. Details regarding patients, clinical parameters and applied therapy are summarized in Table I.
The patients had 15 to 20 min total rest before initial evaluation of vascular parameters in a quiet room with normal temperature. Alcohol or coffee consumption and smoking were forbidden 12 h, and 3 h respectively before evaluation. Parameters were registered before breakfast in supine posture. Two assessments were recorded every 5 min, and the final value represented the mean of the two measurements for each group.
Study group characteristics.
Physical training design. The intervention was applied only to group A, and consisted of 50 min of exercise training, four times a week for 4 months, under the supervision of a licensed physical therapist highly experienced in cardiovascular rehabilitation. The exercise training program comprised a combination of 30 min of aerobic exercises and 20 min of resistance exercises per session. Aerobic exercise training was performed on an ergometer bike and treadmill. The exercise sessions was also performed at an intensity of 60% of each patient's age-predicted maximal heart rate reserve. In order to supervise the exercise intensity and energy expenditure of the patients, we used Polar FT80 heart rate monitors (manufactured by Polar Electro, Kempele, Finland).
Resistance training used the methods previously described by Ho et al. (8) and consisted of 2-3 sets, 10 repeated procedures per set at 10-repetition maximum (RM) of various resistance exercises: leg press, leg curl, leg extension, bench press, and rear deltoid row. Each major muscle group involved in resistance exercises was evaluated weekly using the 10RM test: patients performed each exercise at a selected weight and if they completed fewer than 8 or more than 12 repetitions, the weight was adjusted accordingly and the exercise re-attempted after resting until the 10-RM level was determined. Each patient was evaluated at the baseline and at the end of the study protocol (after 4 months) with regard to arterial stiffness and physical performance. For each patient, physical training was stopped when the assessed parameters such as BP and heart rate reached 80% of their values evaluated during the preliminary exercise test.
Ethical considerations. Informed consent was signed by all patients enrolled in this study before medical procedures started. The Ethics Committee of Victor Babeş University of Medicine and Pharmacy Timişoara (Romania) approved research methodology (5/4429/20.04.2016) and all procedures were performed according to the World Medical Association Declaration of Helsinki.
Statistical analysis used SPSS software, version 17 (SPSS Inc, Chicago, IL, USA); a p-value less than 0.05 was considered statistically significant.
Results
The physical exercise was individualized taking into consideration hemodynamic parameters, age and tested exercise capacity at baseline in order to obtain maximal benefit. At the baseline of the study, the differences between the two groups were not statistically significant.
Significant differences were registered between the two groups after 4 months of physical training combined with usual medication administered to the patients before and during our study. As general parameters, the patients enrolled in group A improved their life quality by changing their lifestyle, which had a strong impact on their work and personal life. Patients from group A became more active and declared that they did not become tired as quickly as they had before the enrollment in the present study. Patients from group A declared that during the 4 months of the study, the physical training had become a habit. They also stated that their exercise capacity had gradually increased. They also registered an enhancement of self-confidence and will to live. In contrast, group B patients became more sedentary and with a decreased effort capacity. In group A, there was also a tendency of wanting to increase the intensity of the treatment quickly, but for safety reasons, this was tempered by the therapist.
The improvement of the hemodynamic parameters was significant in involved patients undergoing physical training. The results of the study regarding hemodynamic parameters of the brachial and central aortic artery for hypertensive patients in group A are summarized in Table II. We compared the parameters before and after 4 months of exercise training supervised by the specialized physical therapist. The same parameters were assessed for the untrained group B and are presented in Table III. For this group, we only made recommendations on lifestyle change. A comparative assessment of final results after 4 months of the study is presented in Table IV.
By evaluation of the seven parameters included in the present study, significant differences were observed between the trained group A compared with control group. PWV decreased for 60 patients in group A (n=63) and only for 14 patients from group B (n=66). The most important changes were for the PWV (Figure 1), SBPao (Figure 2) and PPao (Figure 3) in group A. Most changes in group B were not statistically significant, except PPao which increased. DBP and DBPao at baseline and at 4 months did not differ between the two groups. During the study, five patients needed to stop the exercise session due to high BP during effort (>200 mmHg).
The best results translated as a significant improvement of the arterial stiffness (PWV) and SBPao, both with great clinical importance in vascular aging and secondary complications to hypertension (which are more likely to be caused by SBPao than brachial SBP) were registered in group A. Our results supported a negative impact of a lack of physical training for group B, where these parameters had tendency to deteriorate over time.
We emphasize that parameter differences between groups are highly representative for further studies in this direction and for the elaboration of new recommendations regarding lifestyle changes in general and physical training, especially in hypertensive patients (cardiovascular rehabilitation program).
Discussion
The general clinical benefits of physical training applied for patients with high BP are well recognized and accepted today. Despite life quality improvement for the patients enrolled in medical programs which combine drug and physical therapy, the parameters for evaluating the effects of exercise training on hypertensive patients are not well defined. Recent articles reported the benefits of aerobic training combined with antihypertensive drug use (9, 10) in BP control.
Compared to aerobic exercise training widely used in clinical studies to assess BP behavior, resistance exercises are less used, most studies being combined with programs involving weight loss by caloric restrictions. A recent article reported that combination of resistance exercise and caloric restriction slightly reduced the BP but none of the measures of arterial stiffness changed with resistance exercise, combined or not with caloric restriction (11).
Association of resistance and aerobic training exercise is still a field of debate among cardiologists regarding the benefits of this combination on the improvement of hemodynamic parameters, and currently represents a challenge of training therapy for hypertensive patients. Most of these studies assessed PWV alone or combined with BP values, which can be considered insufficient at the moment (12-14). Li and co-workers reported that aerobic exercise had a positive influence on arterial stiffness in normotensive and hypertensive patients, and had no effects on arterial stiffness values in patients with isolated systolic hypertension (15).
Resistance exercise has differing effects on arterial stiffness depending on type and intensity. Long-term resistance training is associated with an increase in arterial stiffness and, thus, has been considered to have unfavorable effects on arterial stiffness if the training is of low intensity, in a slow eccentric manner, or with lower limbs in healthy individuals. Li et al. concluded that combined training has a neutral or even a beneficial effect on arterial stiffness (15). Our combined training supports the evidence of the beneficial effects on four out of seven parameters assessed in the present study, by obtaining significant positive changes after 4 month of such combined training.
Variability in hemodynamic parameters among patients enrolled in the 4-month physical training program (group A).
Parameters for control group patients (group B) who refused physical training.
Comparative assessment of hemodynamic parameters between the control (group B) and trained group (group A) after 4 months of physical training of the latter.
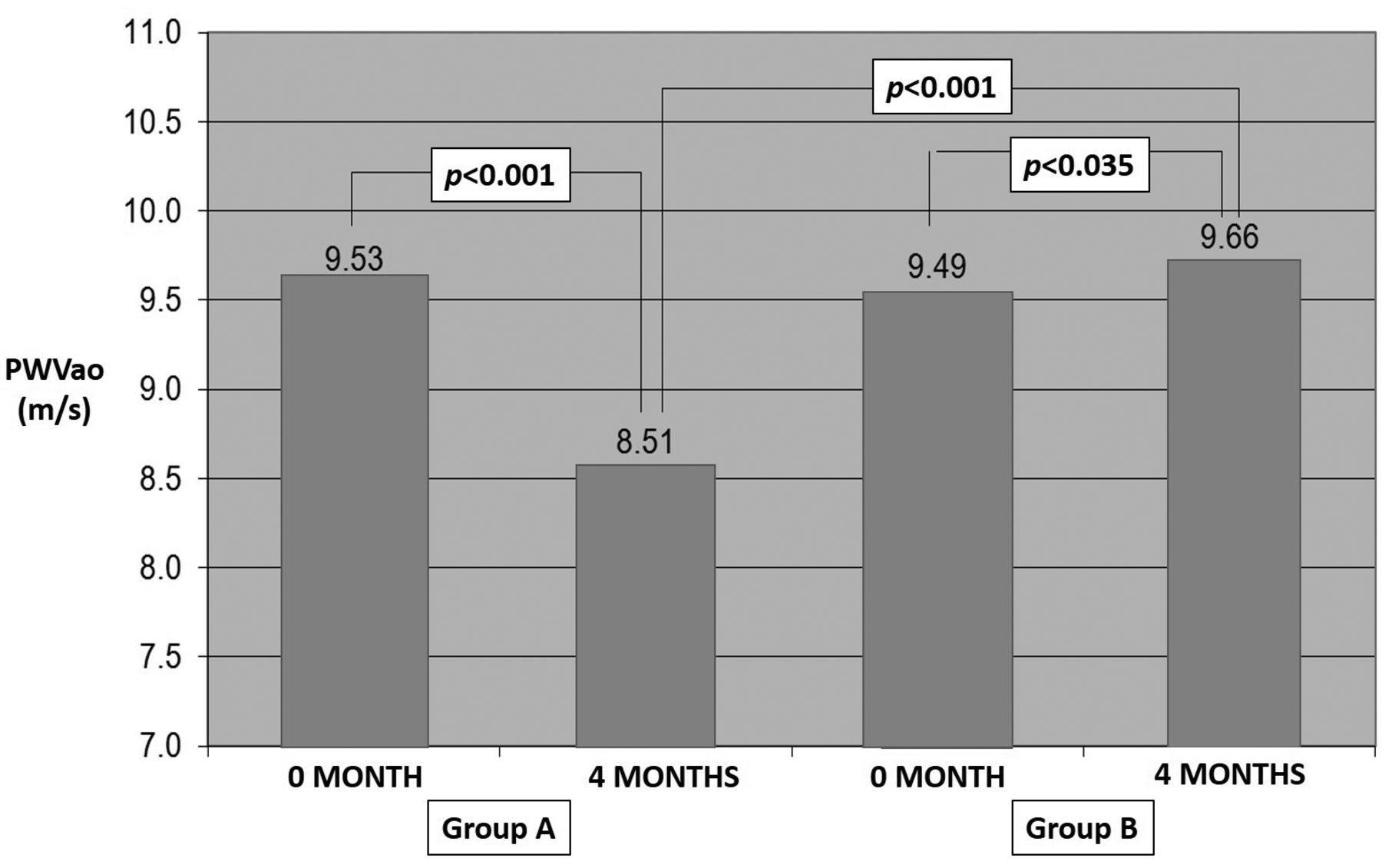
Aortic pulse wave velocity (PWVao) in the control (group B) and trained group (group A) registered at baseline and after 4 months. Significant positive changes were found in group A compared with group B after 4 months; PWVao actually significantly increased in group B patients.
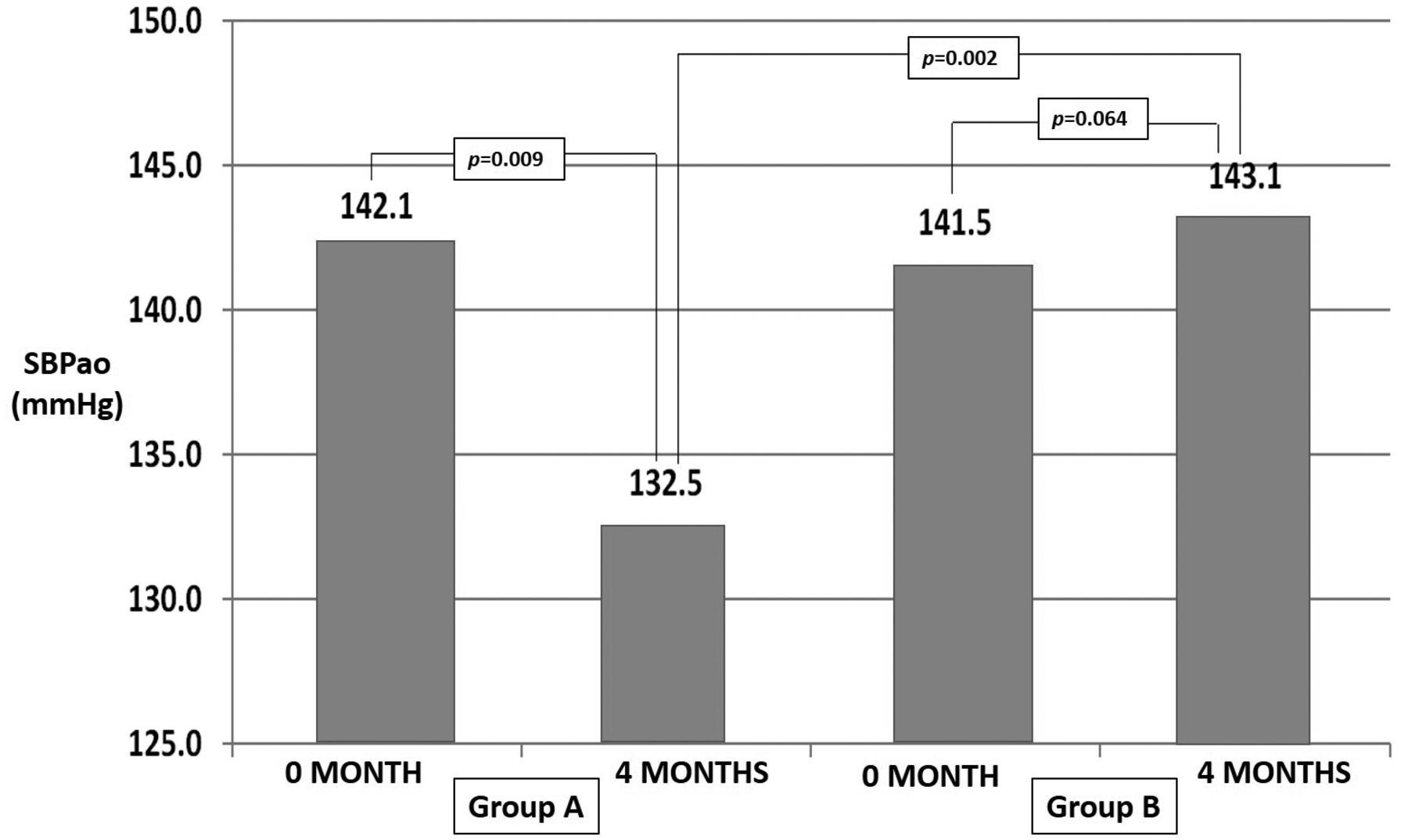
Aortic systolic bood pressure (SBPao) in the control (group B) and trained group (group A) registered at baseline and after 4 months. SBPao significantly decreased in group A at 4 months compared with group B.
Based on these controversial data from the literature regarding The types of physical training with optimal results on hypertensive patients (16), we proposed here a training plan which combines aerobic and resistance exercises but, compared with other previous studies, being followed by study of the effects of this combination on seven main hemodynamic parameters.
Another controversial issue regarding the effects of physical training on hemodynamic parameters in hypertensive patients is the length of physical training able to induce changes in the hemodynamic parameters values. It seems that after 5 weeks of training, BP starts to decrease (17), but other hemodynamic parameters, such as PWV or related parameters are not influenced. After 8 weeks of physical training, Rossow et al. demonstrated that high-intensity resistance training appeared to improve microvascular forearm function, while not changing carotid-femoral or femoral-tibialis posterior arterial stiffness. However, a large degree of individual variation was found and arterial stiffness adaptations appeared to be positively related to initial stiffness values (18).
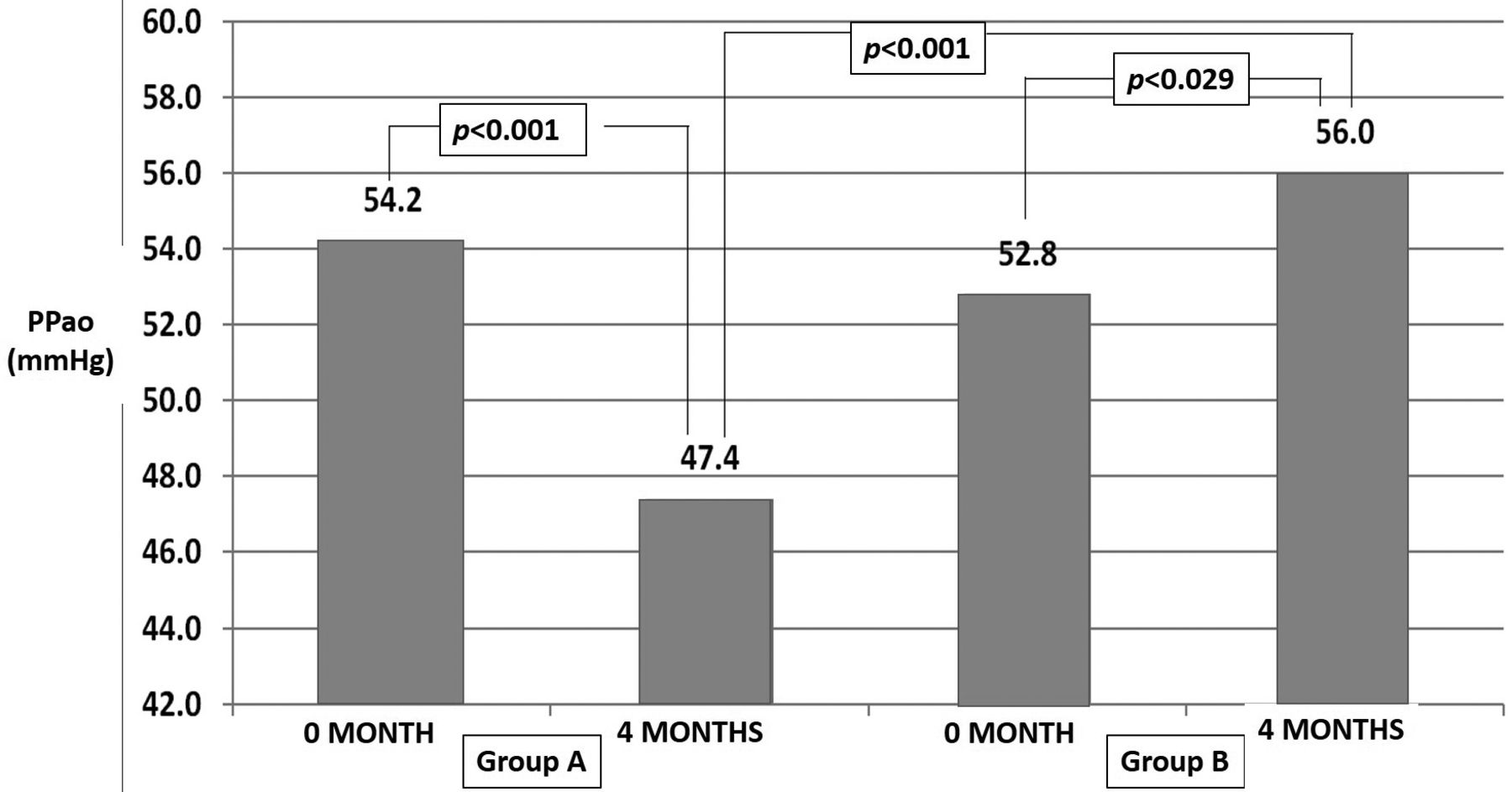
Aortic pulse pressure (PPao) in the control (group B) and trained group (group A) registered at baseline and after 4 months. PPao significantly decreased in the trained group (group A) but also significantly increased for the non-trained group (group B).
All these controversial issues derive from the lack of experimental data regarding the assessment of the seven parameters used in the present study. Recently, Bouissou-Schurtz et al., developed an experimental model for studying the relationship between day-to-day variability in BP and arterial stiffness (19). By using approximately the same parameters as we used in our study, the authors experimentally assessed day-to-day variability of BP and its tissular and clinical impact on the aortic wall and arterial stiffness. Several recent data translated these findings in humans, by noninvasive assessment of 24-h arterial stiffness and central hemodynamics under dynamic conditions in daily life which seems to help in assessing arterial function impairment in hypertensive patients (20). The main common conclusion of these studies was that in hypertensive patients, 24-hour BP variability is strongly strong related to aortic BP and stiffness, which is independent from the absolute 24-h BP level.
Evaluation of the intrinsic mechanisms based on morphological data involved in the hemodynamic parameter variability in hypertensive patients continues to remain one of the most challenging problems faced by cardiologists because of the ethical issues mainly. Essential hypertension is associated with decreased lumen area and a tendency for increased basement membrane thickening in capillaries of skeletal muscle. Exercise training may improve the diffusion conditions in essential hypertension by altering capillary structure and capillary number (21). In a study developed by Gliemann et al., the authors aimed to elucidate whether essential hypertension is associated with altered capillary morphology and density and to what extent exercise training can normalize these parameters (22). They obtained vastus lateralis muscle biopsies from individuals with essential hypertension and normotensive controls before and after 8 weeks of aerobic exercise training. After training, 15% increased capillary-to-fiber ratio was reported in the hypertensive individuals only. Capillary area and capillary lumen area were increased by 7% and 15% in the hypertensive patients, whereas capillary basement membrane thickness decreased by 17% (p<0.05). Vascular endothelial growth factor expression after training was increased in both groups, whereas that of its corresponding receptor-2 decreased by 25% in the hypertensive patients (p<0.05). These findings correlated with hemodynamic parameter changes may improve both treatment and lifestyle of hypertensive patients who are enrolled in physical training programs by explaining the tissular and molecular basis of improvement in hemodynamic parameters (22).
Conclusion
Our results demonstrate that changing the lifestyle is not enough to reduce cardiovascular risk, but we must elaborate adequate and individualized rehabilitation programs evaluated by a panel of hemodynamic parameters comparatively assessed. We need to maximize the benefit of physical exercise and to improve peripheral and central hemodynamic parameters and arterial stiffness. It was shown that by enhancing these parameters, we can reduce cardiovascular morbidity and mortality (8). Although group B also received recommendations according to the ESC prevention guidelines, the parameters were not improved compared to those from group A trained with the rigorous rehabilitation program.
By physical activity in general, and physical training in particular, we can improve both hemodynamic and stiffness parameters in order to make a model for delaying arterial aging. We believe that the is great benefit to be gained from rehabilitation programs for hypertensive patients due to the cost–benefit ratio in favor of public health.
Based on our results, we believe that exercise training programs improve hemodynamic parameters such as SBP, PP, SBPao, and PPao. Thus, physical training as part of cardiovascular rehabilitation has a positive impact on arterial stiffness parameters such as PWVao. Rehabilitation programs are a safe and effective method for reducing cardiovascular risk. Exercise training may delay stiffening of the large arteries (aorta) and in this way perhaps delay arterial ageing.
Acknowledgements
The present work was developed with the support of Atherosclerosis and Atherothrombosis Group of Romanian Society of Cardiology and also supported by Victor Babes University of Medicine and Pharmacy Timisoara, Romania. S. Iurciuc, M. Iurciuc, C. Avram and A. Avram had an equal contribution to this work and thus, all of them can be considered as principal authors of the present work.
Footnotes
Conflicts of Interest
None declared.
- Received April 3, 2016.
- Revision received May 8, 2016.
- Accepted May 11, 2016.
- Copyright © 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}
{kind=link}