


Abstract
Intracytoplasmic sperm injection (ICSI) has become an indispensable procedure of every assisted reproduction unit. This has created as much controversy as it has awe. As this is a multistep invasive technique, every part of the procedure has become subject to investigation. We contribute this review aspiring to offer the embryologist insight into all available approaches of securing an effective ICSI practice. Herein we present all the different approaches with respect to handling of the human oocyte, taking into consideration the important steps of the technique such as the oocyte positioning, timing of performing ICSI, the option of viewing the meiotic spindle and further individual action such as artificial oocyte activation, rescue ICSI and in vitro maturation. We enrich this by including our view based on our collective experience and current practice. Published studies have led to various options for performing ICSI, resulting in in vitro fertilization units around the world adopting different approaches. The steps that ICSI technique entails discussed from the oocyte perspective are still a long way from being organized into one secure and optimal protocol. Our stressing of the need to secure an efficient ICSI protocol could be the trigger for further well-designed larger scale studies with all the latest technological advantages. We aim to approach this subject in categories and assess them separately. However, ICSI is a multifaceted procedure involving several consecutive steps and when evaluating one we cannot exclude the end effect of the previous, or the overall effect of the different practitioners involved form beginning to end.
Recent global demographic surveys indicate that infertility remains an ongoing reproductive problem and is estimated to affect as many as 186 million people worldwide (1). The assisted reproductive technology (ART) community is committed to working towards not just a positive pregnancy test but rather striving to secure excellent obstetric and perinatal outcomes. An estimated 3.75 million births have resulted from assisted conceptions (2) During the last 37 years since the birth of Louise Brown, the world of in vitro fertilization (2) has changed dramatically from overcoming blocked fallopian tubes into the era of the ‘omics’ evaluation of the embryo, employing equally invasive and non-invasive tools that promise to predict and improve results.
The evolution of several techniques dedicated to assist male factor infertility in the IVF laboratory incidentally led to the birth of intracytoplasmic sperm injection (ICSI) (1) and the face of IVF has never been the same since. The ICSI procedure entails the deposition of a single spermatozoon directly into the cytoplasm of the oocyte, thus bypassing the zona pellucida (3) and the oolemma. Due to the invasive nature of ICSI, which goes hand in hand with eliminating natural selection barriers by bypassing many steps in the normal process of fertilization, numerous studies have focused on assessing the associated potential health risks. Studies have concluded that both IVF and ICSI could pose a risk factor for both mother and baby, form pregnancy complications such as pre-eclampsia, growth retardation, and prematurity (4), as well as higher rate of congenital malformations, developmental abnormalities and a higher risk of increased aberrations in imprinting patterns due to the possible transmission to progeny from ICSI of chromosomal alterations leading to all the above (5, 6). However, an equal number of studies negate any correlation (7-9) and emphasize that any association could very well be attributed to the increased risk for health problems present in couples undergoing IVF/ICSI cycles and not the actual techniques themselves. Before placing the blame, we need to remember that in the frame of ART, it is not feasible to dissociate the effect of a certain technique from the effect of the existing biological and clinical profile of the prospective parents, let alone the effect of the overall treatment during an ICSI cycle, from ovarian simulation to embryo culture conditions. The follow-up studies on children from ICSI have shown that the procedure is safe and the slightly higher incidence of neonatal malformations or de novo gonosomal abnormalities are related to the genetics of the infertile couples (10).
There has been much hype lately within the clinical embryology community with respect to how best to approach ICSI practice, especially with respect to controversial procedures suggested for extremely challenging and rare circumstances, such as zona-free oocytes or globozoospermia (11). With this review, our principal intention is to offer the embryologist and the standard IVF laboratory insight as to the clinical options practiced in routine typical ICSI cases and the challenges arising from such. In the following sections, we provide insight into the various approaches regarding the oocyte in relation to ICSI and evaluate their clinical significance in improving the outcome. An outline of our approach analysis is clearly illustrated in Table I. Our review is arranged in the following categories: handling and positioning of the oocyte, timing of performing ICSI, the option of viewing the meiotic spindle during the procedure, the effect of the numerous stimulation protocols that yield oocytes, and further special treatments deemed necessary such as artificial oocyte activation (AOA) and in vitro maturation (IVM). Finally with respect to the procedure, we acknowledge the effect of the medium environment and physical conditions during ICSI, the several options available, and even the human element namely the differing experience from practitioner to practitioner which always adds another level of complexity when aiming to conclude to what should be avoided and what should be adopted in terms of practice.
Polar Body Positioning and Morphology During ICSI
A major debate with respect to the ICSI procedure is the optimal positioning of the first polar body as it has been associated with the presumed location of the meiotic spindle (12). During meiosis, the meiotic spindle is responsible for normal alignment and separation of chromosomes, thus any disruption of the meiotic spindle can lead to rearrangement of chromosomes in the cytoplasm and may contribute to aneuploidy after fertilization (13). Therefore, in order to avoid damage to the spindle that may lead to genetic abnormalities, embryologists orientate the oocyte on the holding pipette on the basis of the position of the first polar body (14).
Understanding the risks of such a delicate procedure, in order to reduce possible damage to the precious oocyte, the most common clinical practice of ICSI involves positioning the first polar body at 6 or 12 o'clock (see Figure 1) and injection of spermatozoa into the oocyte at 3 to 9 o'clock (14).
In 1995, exploring the different practices for ICSI, including sperm deposition and oolemma breakage, Nagy et al. reported that there were no differences in the survival rate and in the normal fertilization rate between the 6 and the 12 o'clock positioning of the polar body, but a significantly higher rate of good-quality embryos after two days in culture was noted for the 6 o'clock position group. In the same decade, Westerlaken et al. also found that orientation of the first polar body at 6 o'clock resulted in a significantly higher proportion of good quality embryos in comparison to that at 12 o'clock. (15, 16). Subsequent studies that compared the two accepted clinical practices of positioning the first polar body at 6 and 12 o'clock demonstrated different outcomes and slowed that the orientation of the first polar body during ICSI does not seem to affect the clinical outcome (17, 18).
In 2000, Blake et al., on the assumption that the second meiotic metaphase II spindle lies in close proximity to the first polar body, attempted injection in nine distinct orientations so that the first polar body was stabilized at 5, 6, 7, 8, 9, 10, 11, 12, or 1 o'clock, excluding the most rarely performed positions (2, 3 and 4 o'clock) with greater risk of damaging the spindle. A total of 10.417 metaphase II oocytes were assessed for this study and showed that the location of the meiotic spindle in relation with the sperm deposition can in fact affect the fertilization rate as well as embryo development. Therefore, the study suggested the polar body not to be positioned at 8, 9 or 10 o'clock, nor at 5, 6, 12 and 1 o'clock because of the potential delay in pronuclear syngamy. Furthermore, orientation of the polar body at the 7 or 11 o'clock position during ICSI appears to ensure higher fertilization rates and the development of the greatest proportion of high-quality embryos (19). In the same field of study, new findings strengthen this hypothesis, and suggest that the 11 o'clock position may be the preferred position of the polar body during sperm injection (20).
All the above studies tried to suggest the optimal position for the oocyte respecting the theoretical association between the first polar body and the location of the meiotic spindle. Nevertheless, the location of the polar body is only a crude measure for spindle position (21) because these do not always coincide as evidenced by immunostaining or polscopy (22).
Risks and benefits of human oocyte handling options during intracytoplasmic sperm injection (ICSI).
Moreover, since it has been reported that the morphology of the first polar body before ICSI is related to the fertilization rate, cleavage rate and embryo quality, it is important to record its size as normal or enlarged, as an enlarged polar body is related to poorer rates (Figure 2). The same study maintains that polar body fragmentation (Figure 3) does not seem to affect ICSI outcome (23). Still, there are no criteria for predicting oocyte quality based on polar body morphology, as the reported data in the literature is controversial.
It was interesting that our literature search did not reveal any studies where the positioning of the polar body during ICSI was entirely random. Hence, it is not possible to state whether total random positioning affects the outcome or not. In our practice, we opt for the 11 o'clock positioning as our collective experience shows that it is the safest option ensuring higher rates, a stand that is also supported by recent studies.
Oocyte Bi-refringence (Polarization Microscopy)
The most essential parameter that gave birth to numerous studies regarding the association of the first polar body position and the ICSI outcome is the importance of the meiotic spindle status during ICSI, and how this affects subsequent embryonic development and normal chromosomal separation. The meiotic spindle consists of a cytoskeleton of microtubules which cannot be observed with light microscopy. This is why the position of the first polar body and its connection to the spindle is so important to the best practice for the injection technique (22).
Various methods have been described employing both human and animal oocytes in order for a new protocol to be included in clinical IVF practice, one that provides safety in performing ICSI and prevents meiotic spindle disturbance. For example, studies with significant findings for the handling of oocytes during ICSI reported that cooling of the oocytes at room temperature for either 10 or 30 min and re-warming them prior to ICSI can cause irreversible disruption of the meiotic spindle and lead to aneuploidy (13, 24). To date, the only indisputable method for testing embryos for possible genetic abnormalities resulting from meiotic spindle disturbance is preimplantation genetic diagnosis (PGD) either by polar body (25) or blastomere biopsy (26). These techniques play a very important role in the ART outcome but fail to reflect mosaicism, plus their invasive nature limits their application as oocyte or embryo biopsy is required.

Performing intracytoplasmic sperm injection by positioning the polar body at 12 o'clock.
In order for embryologists to identify morphologically normal oocytes for use and to ensure precision in practice and security of the precious meiotic spindle, the use of the polarization microscope (Polscope) was introduced (27). The Polscope was developed to study bi-refringence of living cells and uses novel electro-optical hardware and digital processing of data to image macromolecular structures such as the meiotic cytoskeleton (27). The introduction of the Polscope both in the research field of ART and in IVF units helped studies, providing them with a less-invasive technique in comparison to immunostaining methods. These studies suggested that the embryos deriving from oocytes with normal meiotic spindles have superior development after fertilization and in vitro culture (28).
Regarding further application of the polarized light microscope, it enabled studies to positively correlate the embryonic fragmentation process with the progress of the meiotic and mitotic cycles (29). It also became a useful tool for selecting high-quality oocytes and improving the ICSI outcome in cases of advanced maternal age and in poor responders (30). Moreover, Polscope imaging studies attempted to predict the embryonic development based on the morphological characteristics of the meiotic spindle and the zona pellucida, demonstrating that oocytes with visible spindles, spindle retardance >3 nm, and an inner layer zona of 10-12 nm thickness are associated with greater progression to the blastocyst stage (31). Recently, Ghosh et al. used the Polscope to select bi-refringent spermatozoa and proceeded to inject them in 96 cycles, showing promising results in cases with asthenozoospermia and testicular sperm aspiration or extraction (32).

Oocyte with enlarged polar body prior to intracytoplasmic sperm injection.
As the technology expanded, Koike-Tani et al. introduced a new improved Polscope the LC-PolScope and described its use for measuring bi-refringence and polarized fluorescence in living cells and tissues with clarity and great resolution (33). The technological accomplishments have not stopped there; the next generation Polscope will be the multi-focus microscope (MF-microscope) which is a combination of the original Polscope with time lapse function that will provide embryologists with the opportunity to obtain 3D images with up to 25 simultaneous focal planes, successfully revealing the position, alignment and orientation of submicroscopic features (34).
It is undeniable that the Polscope provides a huge advantage in the hands of embryologists, especially in the research and training field. Prior to its development, it was impossible to visualize the spindle without fixing, staining and hence rendering the oocytes unsuitable for clinical use. Indeed, in clinical routine it could be very useful for selection of spindle-positive oocytes, as well as of the right spermatozoon in some cases, and also in determination of the position of the spindle prior to ICSI (35). In light of all these impressive novelties and their highly promising effect on improving clinical results and outcome of ICSI, it almost comes as a surprise that there are studies which maintain that the observed displacement of the spindle is not necessarily associated with poor oocyte and embryo development following ICSI (36). In our opinion, there is currently lack of sufficient data to support that the use of the Polscope in routine techniques will provide a high rate of embryo development and improved birth rates which would in turn make it irreplaceable and invaluable. Equipping an IVF laboratory with a Polscope undoubtedly has benefits to offer and provides data which can prove valuable, especially in training and research. However, in view of the fact that we aim to sustain a balance between additional cost and clinical care, it is certainly not classified as ‘must-have’ equipment in an average IVF laboratory.

Oocyte with fragmented polar body prior to intracytoplasmic sperm injection.
Timing of Denudation and Injection
With ICSI and numerous factors that its outcome can be related to, we are constantly faced with several options and the inevitable dilemma of what is the best approach. Many parts of this technique have not yet been successfully standardized, namely the optimal time of denudation and injection of the oocyte. There are only a few studies focusing on the optimal timing of the ICSI procedure that lack compatibility of results (37). Furthermore, the literature input is rather poor considering when the denudation should take place and how long the pre-incubation stage of the intact oocytes and cumulus mass should be. Ideally we would like to approach the subject of ‘timing’ by categorizing as follows: length and onset of pre-incubation, denudation and injection times. However, published data are not available for all the categories. It seems that there are two major schools of thought. The first supports use of a longer pre-incubation time prior to denudation, and immediate injection following the denudation procedure (38, 39). The second opts for a shorter pre-incubation period followed by denudation, and immediate injection following the denudation procedure. Most of these studies reported that the denudation was performed directly prior to ICSI, focusing on the time frame between oocyte retrieval and ICSI procedure without analyzing the impact of both denudation and ICSI timing on the outcome (37).
Abnormal oocyte with vacuoles and distorted zona pellucida.
Following extensive research in the literature, it becomes apparent that even though there is a specific suggested time frame of 2-6 h incubation for oocytes before insemination employing standard IVF that significantly improves the fertilization rate (40, 41), there are diverse suggestions regarding the ICSI procedure. There are conflicting results regarding the optimal duration of oocyte incubation prior to ICSI, it does, however, have a sensible limit of 12 h following retrieval, where oocyte ageing results in spindle instability (42). It should be emphasized that in studies where the injection of spermatozoon was carried out 9-11 h and up to 11 h after oocyte retrieval, the result was very poor embryo quality (38, 39). Some studies maintain that a longer pre-incubation period followed by denudation and immediate injection improves the fertilization rate (38, 43).
This observed improvement in the fertilization rate can be ascribed to the reported enhancement in the percentage of meiotically mature (metaphase II) oocytes and it is linked to a long pre-incubation stage prior to denudation (44, 45). It is well known that the maturity of the oocyte can be assessed based on two major events: nuclear and cytoplasmic maturation. Nuclear maturity can easily be observed as it is evident from the expulsion of the first polar body. On the other hand, cytoplasmic maturity is somewhat more vague and it is thought to involve maternal mRNA and proteins (46). There is a vast difference in coordination of these two phenomena between the natural and the stimulated cycles, where in the latter they appear to be asynchronous (47). This divergence of the two maturation events could explain why the timing between oocyte retrieval and denudation influences the fertilization and implantation rates (37).
In 2011, a study employed the Polscope to examine the meiotic spindle over time in order to suggest the optimal time for sperm injection and concluded that the optimal time is probably between 39-40.5 h post human chorionic gonadotropin (hCG) administration (48).
On the other hand, the early studies that focused on the optimal timing of denudation reported that the denudation timing did not significantly influence the fertilization rate (49). Moreover, some studies focusing on injection timing showed that there was no significant difference in the fertilization rate or the pregnancy rate following the pre-incubation period in ICSI cycles (45, 49, 50).
In a more recent study on ICSI timing, Patrat et al. evaluated the two different time frames separately between the three different procedures: oocyte retrieval, oocyte denudation, and injection of spermatozoa, showing that denudation should be performed at least 2 h and up to 3 h following oocyte retrieval, with best results achieved around 1.5-2 h in order for high fertilization and implantation rates without negatively affecting the percentage of the metaphase II oocytes. Moreover, injection must not be delayed following the denudation procedure (37).
Clearly, there is no right or wrong approach and therefore there is lack of an exact protocol to be strictly followed. This leads to very diverse ICSI practices around the world and to a constant investigation on the golden standard for the precise timing of denudation and injection. This exhaustive literature search failed to reveal an ideal practice where timing of ICSI is concerned. What became clear is that the incubation time prior to denudation can vary with no significant effect on the rates, providing of course that we do not reach the higher limit where oocyte ageing changes the background. Furthermore, the overall suggestion from the majority of the studies is for the injection to be performed straight after the denudation procedure only. In our practice and in our collective experience, we find that providing the oocyte retrieval is set at 37 h post hCG administration, it is preferable to opt for a pre-incubation time of 3 h, proceed with denudation at 40 h and follow with a short post-denudation incubation period of 1 h leading to injection of the mature oocytes at 41 h post hCG administration. It is apparent that we need larger range studies in order to identify the ideal mode of ICSI practice.
Approaching Failed Fertilization: Artificial Oocyte Activation (AOA) and ‘Rescue’ ICSI
Despite the fact that ICSI is a successful technique with high fertilization rates, complete or nearly complete fertilization failure still occurs in 1-5% of all ICSI cycles, even when a sufficient number of oocytes and spermatozoa are available (51-53). There are many parameters that have been linked to fertilization failure, such as sperm head decondensation, premature sperm chromatin condensation, oocyte spindle defects and sperm aster defects (54). Other causes of fertilization failure can be technical, for example incorrect sperm injection, limited availability of motile spermatozoa (55) and severe disorders such as globozoospermia (56). In the following section, we attempt to approach two clinically applied methods for handling failed fertilization: rescue ICSI and AOA.
Rescue ICSI. In conventional IVF, 5%-20% of unfortunate cases present with total fertilization failure characterized as the absence of the two pronuclei that indicate normal fertilization (57). There are two clinical strategies for treatment. Since the most common cause is failed sperm intrusion, ICSI may be the solution (58). However, informing the couple of failed fertilization marking the end of this cycle and advising towards a subsequent cycle is a challenging situation for all involved, plus such an approach is frustrating, stressful and expensive for the couple, which now has to come to terms with a delay in the course of treatment and the invasive nature of ICSI. An alternate approach, as described for the first time by Nagy et al. in 1993, is to attempt a ‘rescue’ ICSI in the current cycle in 1-day-old oocytes after fertilization failure (59).
In classic IVF, 2-4 h following exposure to spermatozoa, ~90% of the oocytes have been fertilized and 2 h after fertilization the second polar body has been released and can be observed (60, 61). It is therefore possible to identify fertilization failure in a timely fashion and proceed with rescue ICSI within an acceptable timeline.
In a 2014 systematic review of this treatment method, there were 27 studies where rescue ICSI was carried out 22-24 h following oocyte retrieval, reporting a low pregnancy rate outcome of around 9.7%. On the other hand, there were four studies suggesting an early rescue ICSI technique approach of 8-10 h following oocyte retrieval resulted in a promising 44% pregnancy rate. In addition, three studies compared the two approaches, namely the late (22-24 h) and early (8-10 h) rescue ICSI, and concluded that the early rescue ICSI procedure has apparent advantages and a higher pregnancy rate outcome (58). The overall low pregnancy rates reported in rescue ICSI cycles could be related to the in vitro ageing of cultured oocytes or the asynchrony between the embryo developmental stage and endometrial receptivity. These obstacles can be overcome by opting to perform rescue ICSI in the suggested smaller time frame (61) and by cryopreserving good-quality embryos originating from rescue ICSI cycles and transferring them in a subsequent treatment cycle to ensure synchronization (62). Since 2013, application of artificial oocyte activation has lead to a total of 248 pregnancies that have been reported resulting in 177 births or ongoing pregnancies (58). Nevertheless, the main concern about this technique is the possibility of chromosomal abnormalities in the unfertilized oocytes that are ageing during the incubation period and their negative impact on the resulting embryos (63). However, these abnormalities are common in ART and not exclusive to rescue ICSI embryos, and therefore it cannot be extrapolated that rescue ICSI carries a higher risk for chromosomally abnormal embryos and neonatal diseases (58).
It is advisable that rescue ICSI is not routinely used and should strictly be reserved for situations in which oocyte quality does not appear to be a factor. However, every unit must have the required flexibility to accommodate its practice (3). In our view, rescue ICSI is the last resort in failed fertilization cycles and should be practiced with caution and conditionally, depending on the information recorded from the unfertilized oocytes, namely their polar body status, the presence of spermatozoa bound on the zona pellucida, and other observations on the architecture of ooplasm.
AOA. While the exact cause and the molecular pathways are not yet identified, it is clear that an erroneous oocyte activation procedure can have a detrimental effect leading to fertilization failure (52, 53, 64). Oocyte activation is a noted phenomenon with a key role in the starting point of embryogenesis where a metaphase II oocyte becomes a fertilized egg. This spatial-temporal complex process with a series of events is triggered by sperm entry into the ooplasm (65). The spermatozoon–oocyte fusion generates intracellular calcium oscillations that are maintained for a few hours until pronuclei formation (66). In conventional IVF, the complex process of oocyte activation starts a few minutes after the sperm entrance following an intracellular calcium rise (67), whereas during ICSI, the calcium rises immediately due to the artificial calcium influx from the surrounding medium (64). Therefore, the generally accepted conclusion is that all the important and necessary cytoplasmic and nuclear changes are triggered by the increase of intracellular calcium (68), giving rise to all the AOA techniques.
In human assisted reproductive units, AOA methods were initially introduced in order to overcome ICSI cycles with low fertilization rates (69, 70). Among these techniques there are mechanical (69, 70), chemical (71, 72) and physical approaches (73). Yanagida et al. in 1999 suggested the only electrical method for oocyte activation in which an electric field is generated which causes pores to form in the cell membrane in order to induce calcium influx from the culture medium (75, 76). Although to begin with, the intracellular calcium rises, it gradually falls, failing to produce the required calcium oscillations (64). Another method to achieve AOA in the laboratory is by performing vigorous cytoplasmic aspiration during ICSI that may increase the calcium influx during the injection (69).
The chemical method is the most common representative of all AOA techniques in the clinical field and it employs calcium ionophores such as ionomycin and calcimycin A23187 (72, 74). The use of calcium ionophore increases the calcium permeability of the cell membrane in order to raise the intracellular calcium level but still there is only a small degree of calcium oscillations observed (75). In 1997, a combination of the two previous methods was used as a treatment after ICSI with round-headed spermatozoa. The findings suggested that the combination of a vigorous injection with a small amount of CaCl2 and then exposure to calcium ionophore resulted in a successful delivery of a healthy infant (76). Another chemical method that has been described in mouse oocytes is treatment with strontium chloride (79, 80). However, even though the use of strontium chloride does not appear to be hazardous, its use and exact mechanism is still unclear (77).
One of the latest studies on AOA in mouse models suggest a new potential method for achieving calcium oscillation by microinjection of recombinant phospholipase C-zeta after standard ICSI (78). Phospholipase C-zeta is located in the peri-nuclear theca of spermatozoa and is released into the cytoplasm following sperm-oocyte fusion where it facilitates the hydrolysis of inositol 1,4-bisphosphate to inositol 1,4,5-trisphosphate and activates calcium release from the intracellular calcium stores (68, 79). Consequently, it has been proposed that sperm deficiency of phospholipase zeta could be a possible cause of certain failed fertilization events (80).
It should be emphasized that the AOA method is not a horizontally applied choice of treatment for all patients but only for those with a sperm-related activation deficiency (81). Identifying whether fertilization failure following standard ICSI is a sperm-related or oocyte-related deficiency is important for the clinical management of these couples. On this topic, Heindryckx et al. proposed the mouse oocyte activation test (MOAT) as a diagnostic test for patients with oocyte-related fertilization failure in which patient's sperm is injected into mouse oocytes (82).
In 2015, Sfontouris et al. published a systematic review and meta-analysis of randomized controlled trials that compared results of conventional ICSI and of AOA followed by conventional ICSI (83). It was very interesting that the literature revealed limited data regarding the association between AOA and potential adverse health outcomes in the children born. However, a historical pilot study evaluated the physical and mental health of 79 and 89 children from 275 and 406 couples undergoing ICSI-AOA using ionomycin and conventional ICSI, respectively. Parameters such as clinical pregnancy, abortion, type of delivery, and health of children (major birth defect, mental and behavioral status) were evaluated in this study, which concluded that AOA did not force a greater risk on the physical and mental health of children born through it (84). Nonetheless, there is a great need to further the design of larger clinical trials in order to include AOA in the clinical field as a safe and effective method (83).
Rescue ICSI and AOA are two techniques that do not mutually exclude one another, but both have ensured a particular role in IVF practice, as both have important benefits to offer when applied with strict criteria to very specific target cycles. Rescue ICSI translates as the desperate and final attempt of the IVF laboratory to salvage an IVF cycle that has failed to ensure normal fertilization in the form of evidence of two pronuclei and two polar bodies. It is an action that takes place on the concept of having ‘nothing to lose’ directly following the fertilization check on the same cycle. Literature reveals practices that opt to employ AOA for poorly responding patients (74), as well as for patients with polycystic ovary syndrome (PCOS) (85) in an effort to ensure maximum fertilization rates for these sensitive, patient groups with poor prognosis. Even though the results appear to be promising, there is an issue raised with respect to whether there is a valid requirement for AOA application, and if in fact these patients fit the criteria for such as practice. In light of the recent not-without-reason hype on the vast epigenetic impact of IVF practice, it is our view that AOA application should be a careful decision that the laboratory makes and prepares for in a subsequent cycle following a failed one, identifying this as an acceptable criterion for its use and aiming to limit its potential overapplication simply on the grounds of improving results.
IVM and ICSI
The retrieved oocytes following controlled ovarian hyperstimulation (COH) can be categorized into three maturation stages: mature metaphase II, immature metaphase I and immature germinal vesicle oocytes. Some studies reported that 15-20% of the total number of oocytes retrieved in stimulated cycles were immature (86, 87). In clinical routine procedure, immature oocytes are generally discarded in ICSI cycles. However, in cases where all or most of all the retrieved oocytes appeared to be immature, the recovery of these oocytes followed by IVM and subsequent ICSI is an alternative choice of treatment (88).
It has been reported that for most immature oocytes, rapid nuclear maturation can take place spontaneously in the same day of the retrieval procedure; employing an IVM protocol for the remaining immature oocytes, it seems that they will most likely achieve the desired maturation stage overnight (89). In 2007, Hyun et al. in a small-scale study suggested that in IVM-ICSI cycles, the optimal time for injection is 2-4 h following the first polar body extrusion. This is because even though nuclear maturity is reached earlier and faster, cytoplasmic maturation requires further time (90). Moreover, some IVM studies that include polarized microscopy suggested that the Polscope can be a precious tool in IVM-ICSI cycles, improving the fertilization rate, as it can surely identify the precise oocyte maturation status (91).
IVM is currently not a routine procedure in every assisted reproduction laboratory and despite the development of different culture protocols and use of oocytes from different treatment procedures, IVM is still associated with a low fertilization rate and overall delayed cleavage rate compared to metaphase II oocytes (92). In addition, studies that report normal pregnancies and live births in IVM-ICSI cycles have been limited to case reports, showing a clear need for further investigation (93-96).
It is our opinion that IVM is a very promising technique with a very specific role in the IVF laboratory. There are still trials and tribulations on improving the actual procedure, referring to protocols, media of choice and timeline of application. However, as its application comes hand in hand with benefits as well as detriments due to the lengthy and debatably safe culture conditions the oocytes are subjected to, it is of the utmost importance to restrict its application to the very specific target groups of patients that require it, such as those with PCOS and poor responders.
ICSI Media
A major debate in the ART field is that it is still unclear which culture medium lead to the highest fertilization and pregnancy rates, and whether the composition of the medium affects embryo quality. In trying to answer these questions, some studies reported that the culture medium may have an impact on embryo quality in IVF/ICSI cycles (97, 98). The varying components of the commercially available culture media make the comparison of the diverse protocols difficult, especially as these are combined with different time frames and suggested environmental parameters such as O2, CO2 and temperature. In 2013, Mantikou et al. published a systematic review where 20 different culture media from 11 commercial companies were compared. The study did not identify the ‘best’ medium due to insufficient data available in the literature, it did however prove the indisputable effect of the culture media on embryo quality and success rates during IVF/ICSI cycles, stressing the need for more rigorously designed randomized controlled trials (99). Unfortunately comparative media studies pooling data from various sources suffer from poor quality evidence and present clear limitations involving the inevitable element of ambiguity and inadequate reporting of study methods (100).
With respect to the culture medium that the oocytes are exposed to during ICSI, there are various options mainly summed up in two major categories: HEPES-buffered media (pH stable), and non-HEPES-buffered media. HEPES-buffered media providing the comfort of extra time but a more stressful environment for oocytes; on the other hand, the non-HEPES media are a safer choice for oocytes, but add to the time-sensitive nature of the procedure. In our opinion, the dilemma is not to select between the numerous commercially available media of the same type, as this does not seem to play a role in results (101) but instead select between the two major categories: HEPES-buffered and non-HEPES-buffered media. In our experience, our protocol is adjusted according to the case in hand and its special requirements, if any. In particular, we opt for use of non-HEPES-buffered media when sperm quality does not dictate a longer time for sperm selection, and original oocyte assessment classifies the procedure as straightforward. On the other hand, if the case presents difficulties a priori regarding the sperm or oocytes that we believe will lead to adding extra time to the procedure, such as immotile testicular biopsy-retrieved spermatozoa, or the knowledge from a previous cycle of fragile, or sticky oocytes, then we opt to exclude time from the equation and perform ICSI employing HEPES-buffered media. In our laboratory, we also adjust the media depending on the practitioner and the speed of practice. For instance, during training and for junior embryologists, our recommendation is the use of HEPES-buffered media. All of the above, along with the issue of choice between different media, can be alleviated if the protocol dictates multiple ICSI dishes per patient, ensuring minimum oocyte exposure, and therefore non-HEPES-buffered media should be employed. However, we find that such a practice adds to the overall time and cost that is required to perform ICSI, plus it may increase the risk of needle/pipette blockage if the set is not renewed. Finally, in practices where the micromanipulator is placed within an IVF chamber ensuring the procedure is performed at stable temperature, pH and overall conditions, then non-HEPES-buffered media can be safely employed without the added stress of time of exposure.
With respect to sperm, standard practice dictates that we use polyvinylpyrrolidone (PVP) to ensure better morphological evaluation of the sperm due to the high viscosity of PVP. However, many embryologists opt for media enriched with hyaluronic acid (sperm slow), as well as plain culture media of low viscosity. There are added benefits and disadvantages for each option, with the latter choice significantly affected by the expertise of the ICSI practitioner.
ICSI Technique
ICSI is a stressful procedure for the oocyte and the setting of this technique must minimize the physical and chemical stress the oocyte is exposed to. In order to denude the oocytes from the surrounding cumulus cells, many units employ hyaluronidase. The concentration and processing time varies, but should be kept to the minimum of 40-80 IU/ml and 30 s, respectively (102). The layout of the ICSI dish is an important element as it must allow the practitioner a quick and accurate procedure. The success of ICSI relies on several points of the procedure, but sperm immobilization (103, 104), oolemma breakage (105) and sperm deposition are the three most important ones as described in the literature. Sperm selection is discussed in detail in our publication on “Improving ICSI from the spermatozoon perspective” (submitted manuscript).
The most common approach to sperm immobilization is mechanical breakage of the tail by pressing it against the bottom of the dish achieved by a fine swift movement of the glass-beveled part of the injection pipette. However, the introduction of laser into the IVF laboratory soon gave rise to an alternate approach for sperm immobilization employing a non-contact diode laser (106, 107). During the actual injection and in cases where PVP is used, it is better to avoid exposure of the oocyte intrinsically or extrinsically to PVP, although there are no reports suggesting that PVP has an adverse influence on fertilization and embryo development (108). In our practice, we opt for mechanical immobilization of the selected spermatozoon and expulsion of any surplus PVP prior to the spermatozoon reaching the tip of the injection needle away from the injection site and before bringing the injection pipette close to the injection site of the oocyte.
An important determinant of successful ICSI has been reported to be the breakage of the oocyte membrane following aspiration of the cytoplasm into the injection pipette (105), although not every research group reached the same conclusion. Some studies reported that this is not a necessary step for successful ICSI (109). In 2001 Dumoulin et al. showed that the type of membrane breakage does in fact have a significant effect on fertilization rate: A lower fertilization rate was reported when there was no or immediate breakage of the membrane, while a higher fertilization rate was observed when the membrane broke following suction application. Furthermore, in cases where the breakage was obtained immediately, there were higher degeneration rates (18). The same conclusions were reported in previous studies where comparable types of breakage such as sudden, difficult and normal were observed (15, 110).
Ajduk and colleagues in 2011 based their studies on mouse oocytes and reported that the deposition of spermatozoon under the cortex or randomly in the center of the human oocyte may affect the amplitude of the cytoplasmic movements and thus embryonic development (111). Conversely De Vos et al. tried to evaluate whether the deposition of the spermatozoon during ICSI may exert an effect on oocyte survival, fertilization, blastocyst development and quality. They reported that Adjuks et al.'s procedure demands high technical skills, moreover there was no evidence that intentional deposition of the spermatozoon under the cortex improved the outcomes, concluding that the routine ICSI technique that Palermo et al. described in 1992 still remains the golden standard (112).
In our collective ICSI experience, there cannot be a strict unique approach, identified as the ‘best’ when injection type, oolemma breakage, and sperm deposition are concerned. Practice and experience reveal that different oocytes seem to respond differently to the same stimulus and hence our practice should be adjusted based on the uniqueness of the physicochemical characteristics of an oocyte as they are experienced empirically during the injection. In other words, there is no way of predicting how an oocyte will react to a certain harsher or smoother approach of injection technique, and hence flexibility during the procedure is key.
Ovarian Stimulation Protocols
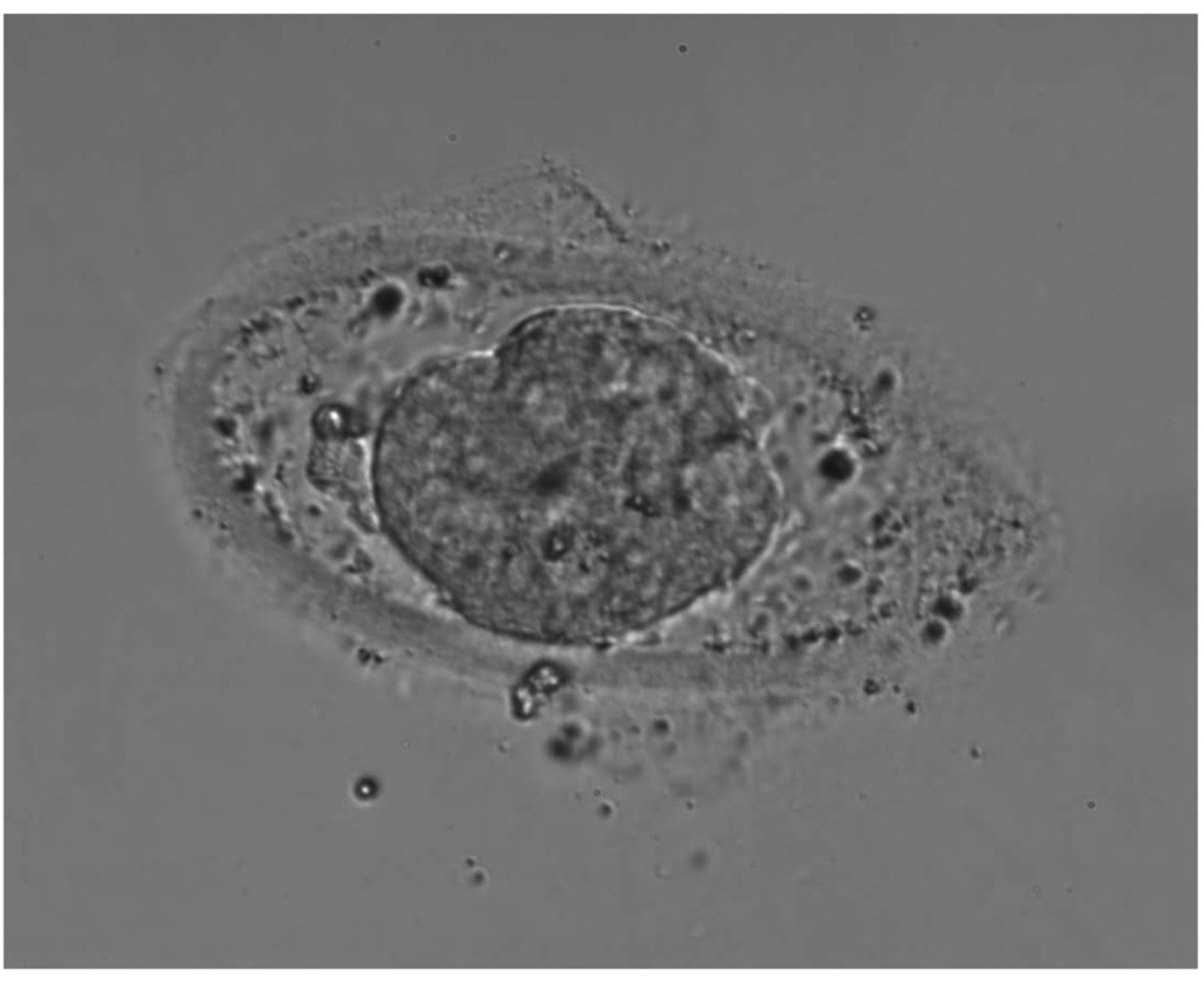
It is without doubt that oocyte quality can be compromised depending on the COH applied. Numerous studies aimed to delineate the molecular mechanisms underlying the association between the various stimulation protocols, their length, and type (use of agonist-antagonist) and the retrieved oocyte quality. Estrogen appears to exert its effects on the cytoplasmic maturation of the oocyte, while progesterone has been shown to accelerate meiotic resumption (113). These in its own right consequently affect ICSI results and, at times, even the actual procedure in cases when the oocyte morphology is clearly affected or if the consistency of the zona pellucida is abnormal (114) (Figure 4). Morphological variations of the oocyte have been linked to extrinsic factors such as stimulation protocols (115, 116). There have been approaches analyzing the expression of relevant genes in cumulus cells aiming to enable us to monitor the consequences of different stimulation protocols and identify the underlying molecular mechanisms by which they influence oocyte/embryo quality (117).
Various suggestions and stipulations are reported for which is the ideal stimulation approach that would ensure a good oocyte yield both in number and in quality, and it is agreed that this is a rather delicate balance to achieve. Our literature search revealed opposing schools of thought and for this reason we choose not to broach this in detail but rather accept that COH can in fact negatively influence ICSI results indirectly and should be taken into consideration, but at the same time, as this is not the main focus of our review, it suffices that we agree that since IVF has a ‘custom-made’ approach, it is hard to identify a gold standard protocol.
Conclusion
There is a worldwide need for a universal approach to techniques such as ICSI. It is often that the embryologist ponders on the ever pressing issue of “How can we make ICSI better, safer, and more effective”? Striving to ensure the best results and analyzing every step of the technique in order to avoid failure is always on the laboratory agenda. We found that a combined review collectively analyzing and assessing published approaches on how to improve ICSI is of significant value and can contribute considerably to the embryology laboratory and its routine practice.
Obviously evaluating the effect of the ICSI technique and associating it with the future embryo dynamic would be ideal, but such an approach would require employing tools that would allow us access to the proteomic, metabolomic and genomic profile of the newly-created zygote and future embryo. The invasive nature of such techniques makes it challenging and at times impossible to collect such information in the strict clinical setting. When aiming to suggest ways towards improving ICSI or any clinical technique outcome, it would be ideal to rely on evidence-based studies.
Here we refer to the various approaches available for handling the oocyte in order to perform ICSI. Although highly promising, we must always be very careful when introducing new technology into the IVF laboratory (118). Apart from the added cost and the added level of complexity, as an extra step will be incorporated into the protocols that each IVF laboratory practices, there is also the issue of whether, in our aspiration to improve certain aspects and study them separately in a sometimes isolated fashion, we might miss the possibility that application of such a technique will have a detrimental effect on the biology and physiology of the actual gametes.
We need to stress the need for further well-designed and larger-scale studies on ICSI techniques, indicating the best way to perform the procedure following all the latest technological advances. Organizing such a trial, we need to be able to answer basic questions: Which cases should be included and with what respective reproductive history? Which aspects of ICSI technique are to be evaluated? What is the end-result that we should associate them with? In light of the latest trends, moving our interest from the positive pregnancy test to clinical pregnancy to the “take home baby rate” and finally to obstetric and perinatal outcomes, the need for such trials has become evident.
Footnotes
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Conflicts of Interests
There is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
- Received March 22, 2016.
- Revision received April 25, 2016.
- Accepted May 5, 2016.
- Copyright © 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Polar Body Positioning and Morphology During ICSI
- Oocyte Bi-refringence (Polarization Microscopy)
- Timing of Denudation and Injection
- Approaching Failed Fertilization: Artificial Oocyte Activation (AOA) and ‘Rescue’ ICSI
- IVM and ICSI
- ICSI Media
- ICSI Technique
- Ovarian Stimulation Protocols
- Conclusion
- Footnotes
- References
- Figures & Data
- Info & Metrics