


Abstract
Background: Acute respiratory failure is a frequent cause of emergency medical missions. Continuous positive airway pressure (CPAP) therapy could be particularly beneficial, avoiding risks associated with intubation and invasive ventilation. Hardly any data exist from Germany on this matter. Patients and Methods: CPAP therapy with the Boussignac system as additional measure was introduced in cases of acute cardiogenic pulmonary edema (ACPE) or decompensated chronic obstructive pulmonary disease (COPD) in a physician-supported emergency medical services system (EMS). Results: A total of 57 patients, 35 with ACPE and 22 with COPD, received CPAP. Oxygen saturation improved from 81.6% to 94.8%, and respiration rate from 26.9/min to 18.9/min (p<0.001). Seven patients (12.2%) needed secondary intubation [COPD: one patient; ACPE: six patients, including three with acute coronary syndrome (ACS)]. Conclusion: In physician-supported EMS, CPAP using the Boussignac system is an effective additional measure for ACPE or COPD. For causal ACS, the risk of therapy failure increases.
- Continuous positive airway pressure
- CPAP
- Boussignac
- cardiogenic pulmonary edema
- chronic obstructive pulmonary disease
- COPD
- emergency medical services
Acute respiratory failure (ARF) is a frequent cause of emergency medical missions (1-3). The aim of prehospital care is to stabilize the patient as quickly as possible without endangering him or her through the measures performed in this context. A measure frequently performed in the case of ARF, intubation, namely anesthetic induction, is associated in prehospital treatment with a considerable incidence of serious complications such as hypoxia, failed intubation, hypotension, or circulatory arrest, even if the emergency physician is well trained (4-6). Particularly at-risk are elderly patients and patients with massive hypoxemia (5, 7). For emergency medical services (EMS) it is therefore particularly important to have strategies for circumventing these risks, if possible.
Reviews and meta-analyses based on studies carried out in emergency departments (EDs) have reported a lower rate of intubation and lower mortality compared to standard therapy in cases of acute cardiogenic pulmonary edema (ACPE) and decompensated chronic obstructive pulmonary disease (COPD) if continuous positive airway pressure (CPAP) therapy is applied (8-10). Studies on prehospital CPAP therapy mainly stem from the USA or France. In Germany, with its physician-supported EMS system, only 38% of the EMS areas are using CPAP therapy (11), and studies on success rates and complications resulting from this process are rare (12-13). This article reflects our experience with prehospital CPAP therapy in a German prehospital emergency physician service in patients with ACPE or decompensated COPD.
Patients and Methods
The Kaiserslautern EMS district comprises an area of 1,998 km2 in southwestern Germany with 348,000 inhabitants. According to the indication catalog of the state of Rhineland-Palatinate, an emergency physician is deployed in acute life-threatening situations (e.g. acute severe respiratory distress, unconsciousness, severe traumatic brain injury). These emergency physicians must have a minimum of 30 months of clinical experience, including at least 6 months in anesthesiology and intensive care or in an ED. Every year, about 10,000 EMS missions are performed. In 2007, an initiative by the Medical Director of EMS led to the deployment of CPAP systems on physician-staffed emergency medical vehicles. Due to the simple operation and independence from power sources, Boussignac CPAP systems manufactured by the Vygon company in Aachen, Germany were procured for this purpose (Figures 1 and 2).
Positive airway pressure is established using this system by means of a ‘virtual valve’, where the gas originating from a source of fresh gas is led into a specially shaped plastic cylinder and is swirled around. The vortex creates increasing pressure, dependent on the flow but without direct linear relation. All the time, the system is constantly open, so the patient does not need to overcome additional mechanical obstacles while inhaling and exhaling (12). The generated excess pressure can be read via a manometer using a bypass method. The gas source is oxygen. Depending on the flow, the resulting oxygen content varies between 70% and 100% (14).
Emergency physicians in the Kaiserslautern EMS were trained in the application of the system in a two-hour training session. The indications to be considered were the clinical diagnosis of ACPE or decompensated COPD with massive dyspnea and tachypnea, hypoxia, and pathological auscultatory findings. No defined thresholds were given for respiratory frequency and oxygen saturation. The contraindications were: lack of cooperative ability, age <15 years, disorientation, lack of protective reflexes, retention of secretions, circulatory instability, as well as traumata in the face/neck area.
Criteria for termination of CPAP were: increasing agitation or disorientation, insufficient increase in oxygen saturation, insufficient reduction of respiratory frequency, respiratory exhaustion, newly occurring circulatory instability, angina pectoris, or high-level arrhythmia.
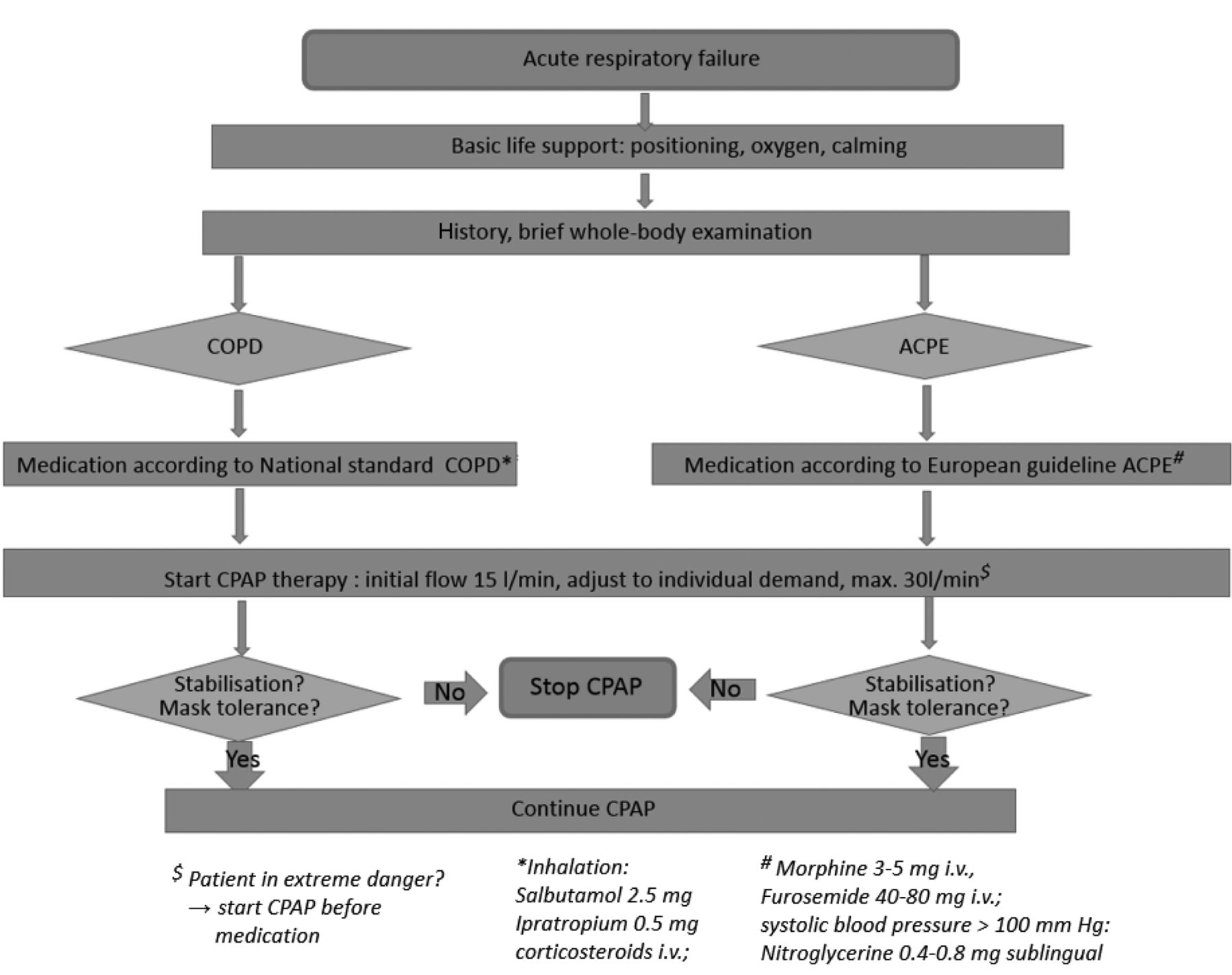
The process was described in a Standard Operating Procedure, which referred to the guidelines of the European Society of Cardiology (ESC) (15), as well as the German National Guideline for COPD (16) with regard to the other measures (administration of medication and oxygen) (Figure 3).
Documentation. The following parameters were documented prospectively: previous experience of the emergency physician with the CPAP therapy; respiratory rate and oxygen saturation: initially under ambient air conditions, with oxygen administered directly prior to the start of CPAP therapy, as well as at the end of the use of CPAP therapy; maximal oxygen flow and positive end expiratory pressure (PEEP); heart rate and blood pressure: initially as well as at the end of the use of CPAP therapy; tolerance to the CPAP mask (assessment: 1=best grade; 6=worst grade); medication; therapy failures and complications. Complications were recorded for up to about 1 hour after admission to the ED.
The data were stored in a pseudonymized form. The analysis was performed with the approval of the Ethics Commission of the Rhineland-Palatinate State Chamber of Physicians as well as the Study Commission of the Westpfalz-Klinikum hospital (processing number 297 E, decision dated 15 June 2015).
Statistics. When data were distributed normally, the mean value and the standard deviation are depicted; if the data were not distributed normally, the median as well as the interquartile range are depicted. Comparisons between continuous variables were made using the t-test (normally distributed data), the Mann-Whitney U-test (non-normally distributed data), as well as ANOVA. Differences between categorical data were compared by means of a Chi-square test. The significance level for the alpha error was set at 0.05.
Results
A total of 57 patients, 35 with ACPE and 22 with COPD, received CPAP therapy, 40.4% were males, 59.6% females. The median age was 79 years (interquartile range: 75-85 years). At an oxygen flow of 21.2±5.8 l/min, the average PEEP was 6.1±1.6 mbar. Oxygen saturation slightly improved from an initial 76.3±11.5% to 81.6±9.6% when oxygen was administered; when CPAP therapy was applied, it continued to increase to 94.8±5.2% (p<0.001). Respiratory rate decreased from an initial 30.2±10.8/min to 26.9±9.6/min with oxygen then further to 18.9±6.5/min during CPAP (p<0.001). The CPAP therapy was well tolerated overall (grade 2.0±1.1). In four patients (7.0%), the CPAP therapy had to be terminated prior to arrival at the hospital, with three of these patients (5.3%) requiring intubation. An additional four patients (7.0%) were intubated in the ED. None of the therapy failures occurred with emergency physicians who had little or no CPAP experience.
Comparison of patients with COPD and ACPE. Patients with COPD tended to be younger and more frequently female than those with ACPE. In both groups, the proportion of emergency physicians with median or greater previous experience with the CPAP therapy was over 80%. In patients with COPD, the CPAP therapy was only administered to one-seventh of the patients as the initial measure; by comparison, it was administered to one-third of the patients with ACPE. Oxygen flow, PEEP, as well as tolerance to the CPAP mask, only minorly differed between patients with COPD and those with ACPE. Oxygen saturation and respiratory rate improved in both groups to a comparable extent under CPAP, whereas there were differences in the heart rate. Intubation tended to be necessary less often in the case of COPD than in the case of ACPE. Patients with ACPE with concurrent acute coronary syndrome (ACS) had to be intubated significantly more frequently (3/6=50%) than patients with ACPE without ACS (3/29=10.3%) (p=0.02). The administration frequency of morphine, diuretics, vasodilators, corticoids, and bronchodilators differed significantly between the two groups of patients (Table I).
Discussion
As far as we are aware, this study is the first to compare the characteristics and the treatment process of patients with decompensated COPD vs. those with ACPE during prehospital CPAP therapy. In other prehospital studies, either only ACPE patients were included (12, 17-24), or the results were not differentiated by the underlying disease (1, 25-28). Another small study comprised only patients with COPD (13).
The patients with COPD treated in this study were younger on average and more frequently female than patients with ACPE. In the general German population, patients with COPD are also younger than patients with chronic heart failure (29, 30). The prevalence of COPD, however, is lower among German women than among men (30), so the cause for the higher number of female patients with COPD remains unclear. Measured by the progress of oxygen saturation and respiratory rate, the efficacy of the CPAP therapy was equally high by comparison for both diseases. Yet in patients with ACPE, secondary intubation was significantly more frequent than in those with COPD. Our observation that among patients with ACPE, the rate of intubation was significantly higher in those with causal ACS than in those without ACS correlates with the finding that ACPE caused by ACS has a poor prognosis (31) and is often also accompanied by the need for invasive ventilation, compared to a pulmonary edema that is the consequence of a hypertensive crisis (32). Considering the above-mentioned risks of intubation and anesthetic induction in the case of ARF, we believe that CPAP therapy can be attempted even for this indication. However, the higher risk that this technique may fail must be taken into account and secondary intubation must be possible immediately.
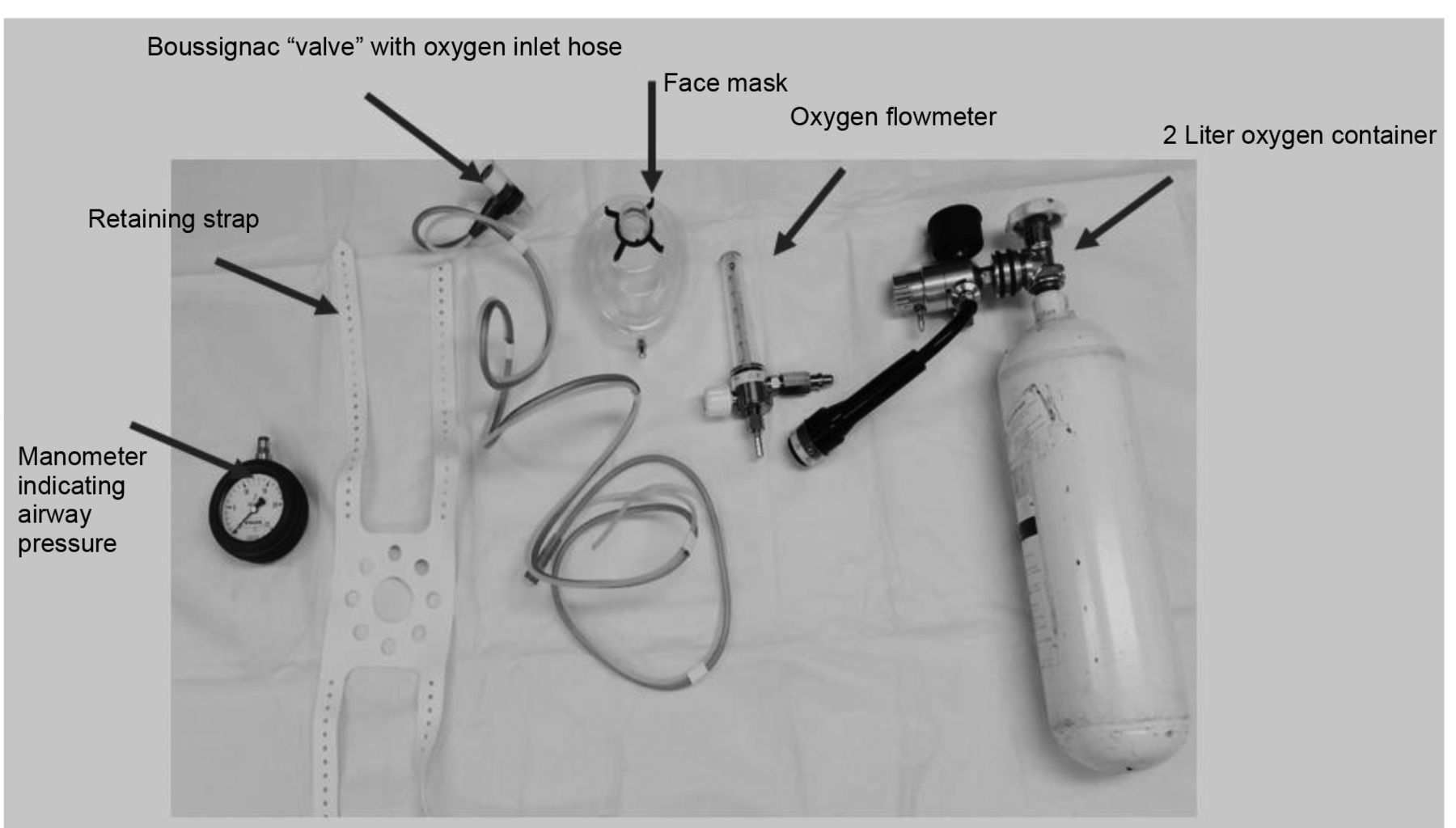
Overview of the Boussignac continuous positive airway pressure system.
In other studies about prehospital CPAP therapy in the case of ACPE – and with a basically similar course of the vital parameters – prehospital intubation rates between 0% (23) and 8% (24) were found, and intubation rates in the ED between 3% (18) and 10.5% (22). Studies with mixed causes of ARF report prehospital intubation rates between 0% (27, 28) and 5.6% (25), and intubation rates in the ED between 0% (28) and 22.3% (1). In the only study to date on patients with COPD, the prehospital intubation rate was 5.5% and the hospital intubation rate was 11.1% (13). The reasons for these great differences are hard to determine, as the studies vary with regard to a multitude of parameters (study design, previous experience with CPAP therapy, inclusion and exclusion criteria, comorbidities, initial vital parameters, CPAP system, inspiratory oxygen content, PEEP level, concomitant drugs). In addition, in some publications, the patients' progress in the ED was not indicated. However, it is remarkable that in several studies with a very low prehospital intubation rate, the secondary intubation rate in the ED was relatively high (1, 22, 26, 27).

Boussignac continuous positive airway pressure system in practice.

Standard Operating Procedure ”acute respiratory failure”, implemented in the Kaiserslautern emergency medical services system. ACPE: Acute cardiogenic pulmonary edema; COPD: chronic obstructive pulmonary disease; CPAP: continuous positive airway pressure.
More than one-third of patients with ACPE in this study received CPAP therapy prior to administration of medication, in contrast to only 15% of the patients with COPD. Together with the initially slightly worse vital values for patients with ACPE, this indicates an even greater need for immediate stabilization of these patients. Here, a simple CPAP system such as the Boussignac system has a great advantage, as it can be deployed within a minimum amount of time. In the guidelines for therapy of ACPE and COPD, drug treatment plays an important role. The data of this study demonstrate great adherence to these guidelines: As recommended by the German National Guideline, approximately two-thirds of the patients with COPD received treatment with bronchodilators and corticoids (16). The majority of patients with ACPE received diuretics (class I recommendation of the ESC) and morphine (ESC class IIb recommendation), as well as vasodilators (ESC class I recommendation) (15) in approximately 43% of the cases. The most likely explanation for the different progress of the heart rate (decrease in patients with ACPE, increase in patients with COPD) is the administration of concomitant drugs (increased parasympathetic activity caused by morphine vs. stimulation of the beta receptors or blockade of parasympathetic nervous system caused by bronchodilators). Similarly high administration rates for diuretics, morphine, and vasodilators in patients with ACPE are found in other work from primarily physician-supported European EMS systems (12, 21, 23, 24). In American studies, the administration frequency of diuretics and vasodilators varies very strongly, with rates for diuretics ranging from 0% (26) to 47.7% (27) and for vasodilators from 27% (26) to 86.4% (27). In these EMS systems, morphine was administered significantly less frequently than in European EMS systems (1, 20, 26, 27). Regarding the administration of bronchodilators and corticoids to patients with COPD, no information was found in the cited works.
Characteristics of patients with chronic obstructive pulmonary disease (COPD) vs. those with acute cardiogenic pulmonary edema (ACPE).
Limitations. The data presented in this study cannot be transferred directly to other ESM systems, as particularly in the German EMS system, the majority of the emergency physicians have significant previous experience with CPAP therapy. In addition, the data were elicited during the everyday work of an EMS system and comprise of a relatively low number of patients. Since most of the studies published to date were also uncontrolled and comprise smaller numbers of cases, additional, prospectively controlled studies with larger numbers of cases would be appropriate, particularly also with regard to the issue of a potentially lower intubation rate and a lower mortality rate (33-35).
Conclusion
Prehospital CPAP therapy using the Boussignac system can be performed with high efficacy and safety in a physician-supported EMS system in patients with ARF as a consequence of COPD or ACPE. It can thus represent an important therapy component in such a system, in addition to drug treatment. In patients with ACPE as a consequence of ACS, the risk of therapy failure is higher. Due to the low number of cases studied to date, further prospective studies should be performed, particularly with patients with COPD.
- Received November 30, 2015.
- Revision received January 13, 2016.
- Accepted January 14, 2016.
- Copyright © 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}
{kind=link}