


Abstract
Background/Aim: HIV infection is a risk factor for re-activation of latent tubercolosis infection (LTBI). In recent years new blood tests for the detection of TB infection have been developed: Quantiferon TB Gold in Tube and TSPOT TB, which are interferon-γ releasing assays (IGRAs), have improved the identification of LTBI. In our study we have compared IGRAs and TST in HIV-positive patients with different settings of immunodeficiency. Patients and Methods: 98 consecutive HIV patients were recruited. They underwent a blood draw, a chest radiography and a tuberculin skin test. The HIV infection setting was detected and IGRAs were carried-out. Five patients showed a complete correspondence of TST, TSPOT-TB and QFT-IT. Discordant results were observed in patients testing positive to IGRAs but negative to TST. Only 2 patients showed positive TST and negative IGRAs. Conclusion: Our study showed a poor concordance between tuberculin skin test and IGRAs, mainly in patients with a low CD4 cell count.
Tubercolosis (TB) is the leading cause of death in patients with HIV infection. According to data reported by the WHO, one -third of the 34 million people living with HIV worldwide are infected with latent tubercolosis and most of these subjects live in Sub-Saharian Africa (1, 2).
Latent Tubercolosis infection (LTBI) is characterized by the absence of symptoms and signs of disease, with a negative chest radiography and negative direct and cell culture tests, and by a positive tuberculin skin test (TST) or positive interferon-γ (IFNγ) release assays (IGRAs) (3).
Medical conditions associated with immunosuppression, such as HIV infection, treatments based on corticosteroids >15 mg/day or tumor necrosis factor antagonists or immunosuppressor drugs after organ transplant, represent a risk factor for progression to active TB and for development of reactivation. Other risk factors are age <5 years old, recent TB infection (in the last 2 years), smoke, drug addiction, chronic diseases such as diabetes and chronic kidney failure (4-6).
The risk of progression from latent to active TB is between 5% and 10% and this risk is greater in the first years after the development of latent infection (6, 7).
People with TB and HIV co-infection are estimated to be 11 million worldwide and in these subjects the risk of progression from latent TB infection to active disease seems to be about 10% annually, which is also the case in patients who receive highly active anti-retroviral therapy (HAART) (7).
Several studies have shown that isoniazid preventive therapy (IPT) as treatment of latent TB infection (LTBI) may reduce the risk of progression to active disease by about 36% and that this risk reduction is about 62% in patients with a positive tuberculin skin test (TST) (8, 10). In order to enhance TB control, it is necessary and urgent to identify and to treat LTBI in HIV patients.
Until recently, TST was the only test available for diagnosing latent TB infection, but this tool has some limitations such as: false-positive results due to exposure to non-tuberculous mycobacteria and to BCG vaccine; false negative results due to impaired cellular immunity; a reader related variability of the results (9).
Certain studies have shown that among HIV patients, the proportion of negative TST is higher than in people without HIV infection (10, 11).
In recent years new blood tests for the detection of TB infection have been developed: Quantiferon TB Gold in Tube (QFT-GIT) and TSPOT TB (T-Spot), that measure the amount of IFN-γ-released from activated T-cells after exposure to M. tubercolosis antigens. Quantiferon determines the level of soluble IFNγ produced, while TSPOT detects the number of IFNγ- producing cells (12, 13).
The antigens used in these tests seem to be more specific than the ones included in Purified Protein Derivative (PPD) and do not cross-react with BCG and M. avium complex. Moreover several studies have shown that IGRAs may be more sensitive than TST in HIV patients for diagnosis of M. tubercolosis infection and less affected by advanced immunosuppression (12-14).
In current literature the data about the performance of the IGRAs in HIV subjects are discordant and limited and few studies compare both IGRAs with TST for diagnosis of LTBI in patients with HIV infection and different grades of immunodeficiency (6, 13, 14).
The aim of the present study was to compare both IGRAs with TST for the diagnosis of latent tubercolosis infection in a cohort of patients with HIV infection and different settings of immunosuppression.
Patients and Methods
Patients and samples. Patients were recruited into at the 3rd Department of Infectious Diseases, Unit of Pneumology and Unit of Microbiology and Virology at D. Cotugno Hospital- AORN dei Colli in Naples.
All eligible patients were HIV-infected adults (age>20 years) treated from December 2011 to December 2013. At enrollment they gave their written informed consent. The subjects with signs and symptoms related to active TB were considered not eligible. Patients with opportunistic infections and pneumonia were also excluded from the study.
Biochemical, clinical and demographic data, such as age, gender, nationality, sexual attitudes, drug addiction, HIV transmission route, history of HIV infection, history of contacts with TB cases, incarceration, were recorded in a database and reported on a medical record.
Procedures. Blood samples were collected to evaluate immunological and viral status of HIV infection at enrollment (CD4 cell count, CD4 cell nadir and HIV-RNA viral load were detected) and to measure IGRAs tests (Quantiferon TB Gold in Tube- Cellestis Ltd, Australia and T-Spot TB- Oxford Immunotec Limited, UK).
After blood sampling, in the same day, each patient underwent a TST with an intradermal injection of PPD 5 UI (Tubertest- Sanofi Pasteur MSD, SNC). The diameter of induration was measured at 48-72 h and considered positive if equal or higher than 5 mm.
Patients with a positive TST or a positive result of Quantiferon or TSPOT-TB underwent chest radiography in order to exclude active TB.
All patients recruited into the study were divided into four groups on the basis of their immunological status:
Group 1: CD4≤ 100 cells/μL
Group 2: CD4≥ 101 and ≤ 200 cells/μL
Group 3: CD4≥ 201 and ≤300 cells/μL.
Group 4: CD4≥301 cells/μL
Demographical and biochemical characteristics of patients included in the study.
To perform T-SPOT TB, T-Cell Xtend reagent was added to blood samples that were processed 32 h after collection. Peripheral blood mononuclear cells (PBMC) were separated by centrifugation from samples and then placed into four wells. Then the wells were stimulated with phytohemagglutinin (positive control), ESAT-6, CFP-10, AIM V medium (negative control) and incubated for 16-20 h at 37°C. The result was considered positive if the number of spot-forming units was >5, as well as when spot-forming units were >2x spot-forming units of negative control. The result was considered invalid if the positive control was <20 spot-forming cells.
Results
The three tests were performed in 98 consecutive patients with HIV infection. Demographic, clinical and biochemical characteristics of the patients are shown in Table I. 88/98 (89.7%) of patients were male, 10/98 (10.2%) were female. Median age was 44.4 years (range=22-77). 81/98 (82.6%) of patients came from Italy, 11/98 (11.2%) were from Sub-Saharian Africa, 4/98 (4.08%) from Eastern Europe, 2/98 (2.04%) from Southern America. Median CD4 was 403.8 cells/μL (range=6-1400 cells/μL).
The number of patients with a CD4 cells count <100 (group 1) was 18 (18.3%). In this group median CD4 was 41.6 (range=22-67 cells/μL). The patients with CD4 ≥101 and ≤200 (group 2) were 9 (9.1%) and median CD4 was 140.5 (range=111-183 cells/μL). The number of patients with CD4≥201 and ≤300 (group 3) was 14 (14.2%) with median CD4 of 255.4 (range=202-300 cells/μL). Patients with CD4≥ 300 (group 4) were 57 (58.1%) and median CD4 was 595.7 (range=304-1400 cells/μL).
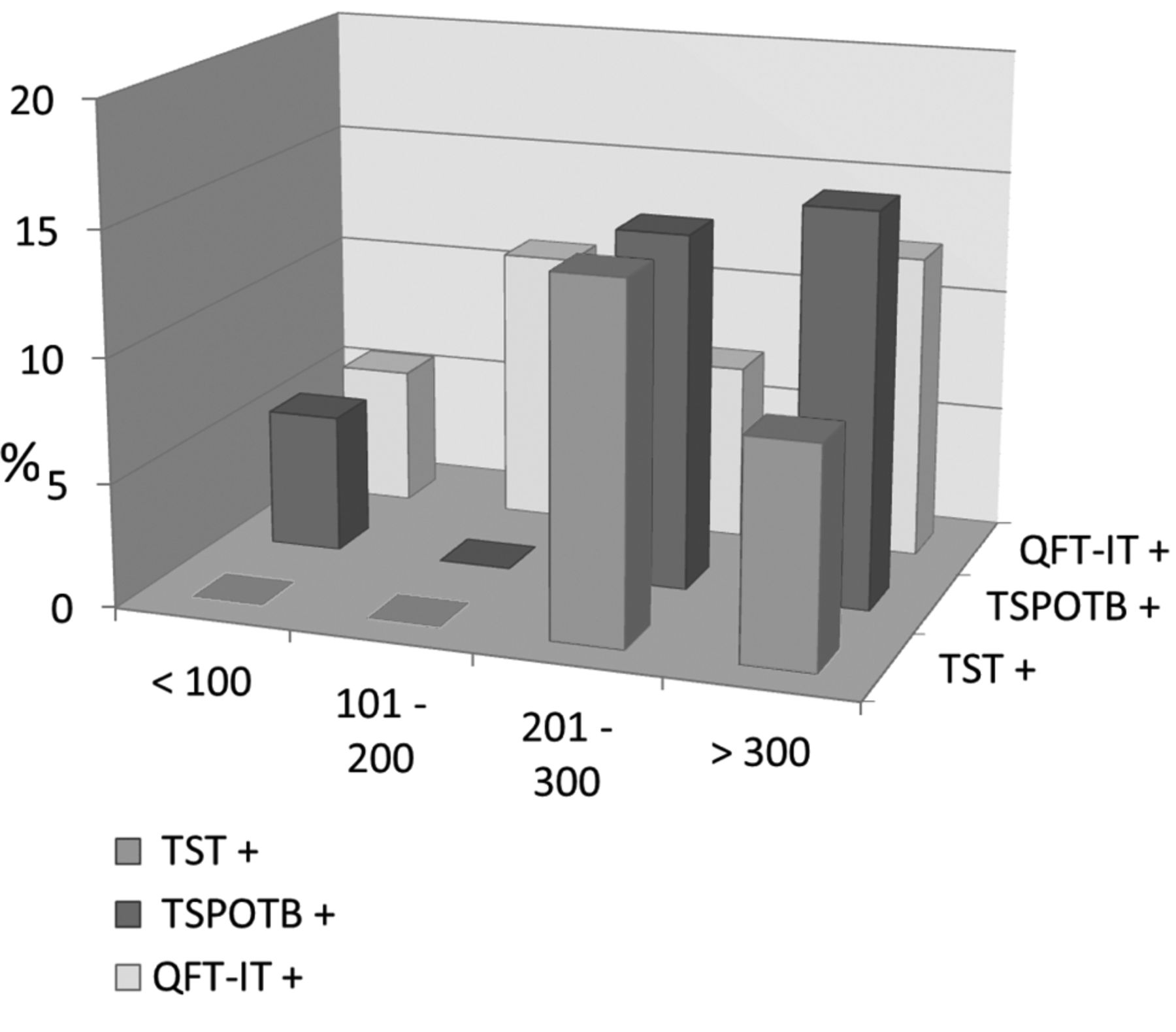
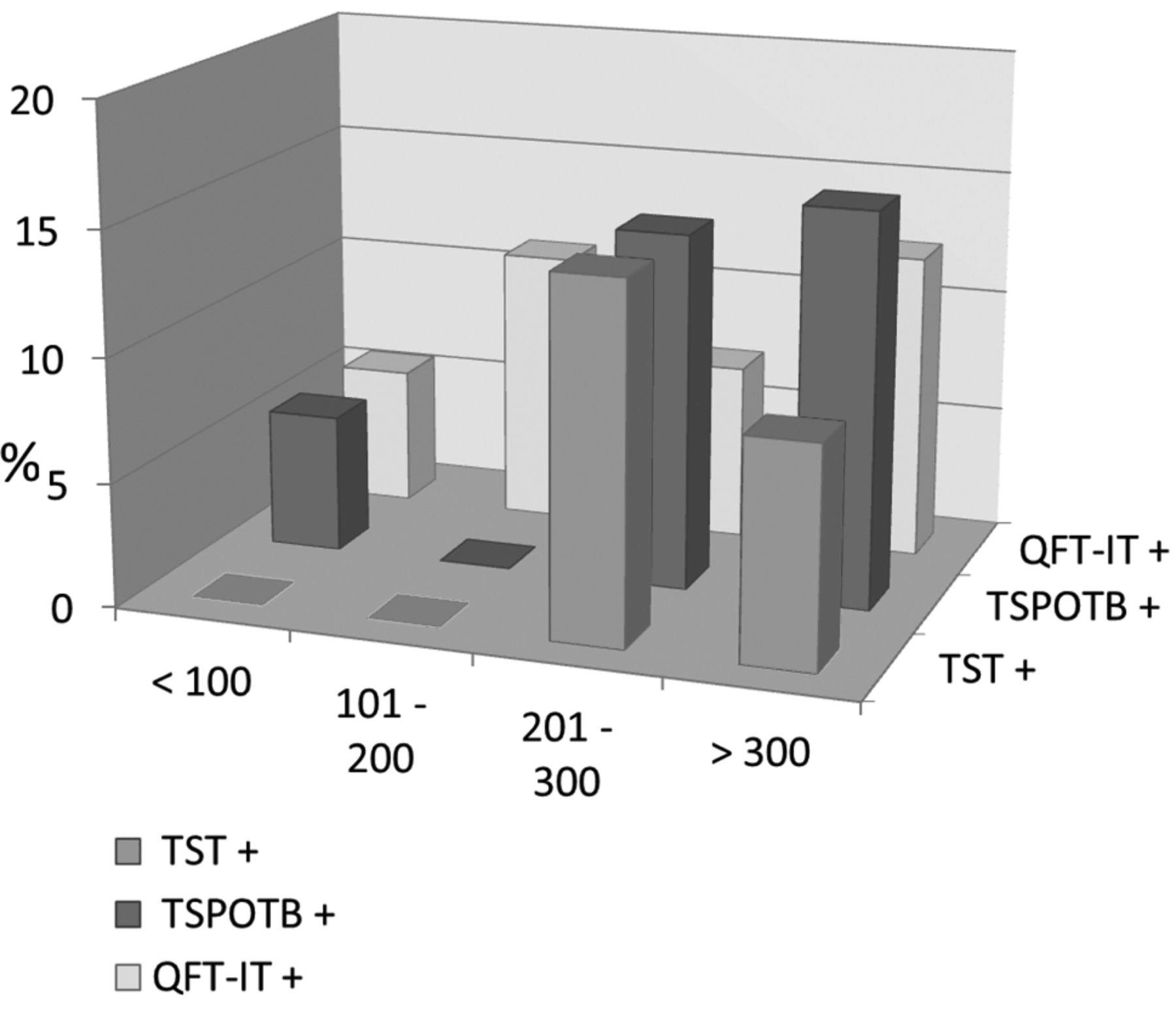
Percentage of positive tests in relation to the number of CD4.
TST was positive in 2 patients of group 3 (14.3%) and 5 patients of group 4 (8.8%). It was negative in 14 patients in group 1 (77.8%), 8 patients in group 2 (88.9%), 8 patients in group 3 (57.1%) and 44 patients in group 4 (77.2%). TST wasn't read in 4 patients of group 1 (22.2%), 1 patient of group 2 (11.1%), 4 patients of group 3 (28.6%) and 8 patients in group 4 (14%).
TSPOT-TB was positive in 1 patient in group 1 (5.5%), 2 patients in group 3 (14.3%) and 9 patients in group 4 (15.8%). The test showed a negative result in 15 patients in group 1 (83.3%), 7 patients in group 2 (77.8%), 11 patients in group 3 (78.6%) and 46 patients in group 4 (80.7%). It was indeterminate in 6 patients in group 1 (11.2%), 2 patients in group 2 (22.2%), 1 patient in group 3 (7.1%) and 4 patients in group 4 (3.5%).
Quantiferon-IT was positive in 1 patient in group 1 (5.6%), 1 patient in group 2 (11.1%), 1 patient in group 3 (7.1%) and 7 patients in group 4 (12.3%). The results were negative in 16 patients of group 1 (88.8%), 7 patients of group 2 (77.8%), 12 patients in group 3 (85.8%) and 49 patients of group 4 (85.9%). It was indeterminate in 1 patient of group 1 (5.6%), 1 patient of group 2 (11.1%), 1 patient of group 3 (7.1%) and 1 patient of group 4 (1.8%) (Figure 1).
Five patients showed a complete correspondence of TST, TSPOT-TB and QFT-IT.
Among patients with a negative TST, 4.1% showed a positive TSPOT-TB and 2.1% had a positive QFT-IT. 9.2% of all patients with a negative TST showed a positive result to IGRAs (Figure 2).

Percentage of positive IGRAs with negative TST.
Discordant results were observed in patients testing positive to IGRAs but negative to TST. Only 2 patients showed positive TST and negative IGRAs. Results of the study are summarized in Table II.
Discussion
TST, TSPOT-TB and Quantiferon-IT were positive in 7.1%, 12.2%, 10.2% cases respectively. Positive results of the tests seemed to associate with higher CD4 cell counts. Our study showed a poor concordance between TST and IFN-γ releasing assays, mainly in patients with a low CD4 cell count, as already reported by several articles in literature (13-15). The results of our study showed an increase in the number of patients that could undergo the preventive therapy for latent TB infection: among patients with negative TST, 4.1% had a positive TSPOT-TB, 2.1% had a positive QFT-IT; 9.2% patients had positive IGRAs, totally.
IGRAs should be able to identify TST negative subjects who could be treated with isoniazid. Interestingly, in our study, the blood tests provided low proportion of indeterminate results (13 cases for TSPOT-TB, 4 cases for QFT-IT). Most of these results seem to be related to a low CD4 cell count.
The undetectable results of IFN-γ release assays could be considered as “transient” results in patients with advanced immunosuppression.
Our results need to be confirmed by further investigations conducted in a larger number of cases, in order to establish the clinical impact and the effectiveness of dual testing approaches.
Comparison of TST, TSPOT-TB, QFT-IT in all 98 HIV-positive patients.
Footnotes
-
Funding
The study was financed by CERIFARC/Regione Campania decree 176 of 03/07/2009 (BURC nr.45 of 20/07/2009) and selected among “Projects for improving of assistance, diagnosis and therapy of HIV infected patients: immunology, co-infection, information and prevention”.
- Received July 17, 2014.
- Revision received October 1, 2014.
- Accepted October 7, 2014.
- Copyright © 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.