


Abstract
Aim: To describe our surgical technique and compare the results of obliteration materials. Patients and Methods: Fifty patients over a 7-year period were evaluated retrospectively. Out of these 50 consecutive patients, 29 had recurrent chronic otitis media (COM) with or without cholesteatoma and 21 patients had old open cavities. Efficacy of mastoid obliteration was assessed by an electronic chart review, otoendoscopic findings, temporal bone computerized tomography (CT) images, and postoperative caloric test. Results: Among 50 patients, inferiorly-based periosteal flap was used in 25 patients (50%) and anteriorly-based periosteal flap was used in the other 25 patients. Tympanic membrane and newly-formed external auditory canal wall was intact in 48 patients (96%). The newly-formed EAC provided sufficient aeration, and satisfactory aesthetic appearance. None of our patients complained of vertigo triggered by cold air or water. There was no significant difference in the caloric test results between the operated ear and the normal ear. No difference was observed in the caloric test between the bone pate and costal cartilage groups. Conclusion: Our results indicate that mastoid obliteration using autogenous bone pate or costal cartilage is helpful in improving the outcomes of revision canal wall-down mastoidectomy in patients with an old radical cavity and recurrent COM or cholesteatoma.
Successful surgical eradication of mastoid disease most frequently requires removal of diseased and sometimes normal anatomic structures by the otological surgeon. Canal wall-down (CWD) mastoidectomy is one such common surgical technique with variable long-term outcomes. An open radical mastoid cavity presents a handicap to the patient. The most common presenting complaint of patients with mastoid bowls is recurrent infection and drainage. If elimination of the cavity appears desirable, one should use an operative technique which does not incur the risk of a cholesteatoma redeveloping.
Recurrent or persistent cholesteatoma or persistent infection and suppuration might lead to failure following surgery for otitis media with or without cholesteatoma (1). Revision CWD mastoidectomy is indicated for recurrent cholesteatoma, recurrent suppuration, recurrent perforation, or recurrent or residual conductive hearing loss (2). A previous histopathological study of human temporal bone revealed that labyrinthine fistula can occur even in the case of exteriorization by a CWD mastoidectomy, especially if there is continued suppuration within the cavity (3). Hakuba et al. reported labyrinthine fistula as a late complication of CWD mastoidectomy in 25 patients (4). Therefore, if possible, mastoid obliteration should be performed with revision CWD mastoidectomy. Since the late 1950s, a number of mastoid obliteration procedures using many different materials with or without canal reconstruction have been described. Local soft tissue flaps have been commonly used for mastoid obliteration (3-7). Unfortunately, these soft tissue flaps almost always tend to shrink and retract, and as only the canal skin is reconstructed, sometimes a marked, cavity-like retraction of the canal is produced. For achieving successful obliteration, the semi-circular canal should be covered with the obliteration material in order to protect it from outside temperatures. Fascia and muscles are always at risk of being resorbed (8). Furthermore, in order to achieve permanent success, the obliteration material should be non-resorbable.
To date, the results of mastoid obliteration using different obliteration materials for revision canal wall-down (CWD) mastoidectomy have rarely been reported. In the present study, we described our technique for CWD mastoidectomy and compared the results of using different obliteration materials.

Frequency of materials used for mastoid obliteration. BP: Bone pate, hDBM: human demineralized bone matrix, CC: costal cartilage.
Patients and Methods
All patients were treated by revision CWD tympanomastoidectomy for an old radical cavity or recurrent choronic otitis media (COM) with or without cholesteatoma. Fifty patients over a 7-year period from January 2005 to March 2012 were evaluated retrospectively. To avoid bias caused by different surgeons, we only included the patients who were operated on by a single otosurgeon. Of these 50 consecutive patients, 29 patients had recurrent COM with or without cholesteatoma and 21 patients had old open cavities. All of the patients were operated on general anaesthesia.
Surgical technique. The ear was re-opened post-auricularly, uncovering the old operative opening in the mastoid bone. The superior part of the incision ran parallel to the inferior border of the temporalis muscle. The inferiorly or anteriorly based flap was developed from the periosteum.
The lining of the radical cavity was exposed without causing damage. The edges of the old radical cavity were drilled to obtain a better view of the cavity. The lining was carefully separated from the walls of the cavity, the semicircular canal, and the facial nerve canal. Granulation tissue was removed from the cavity. The walls of the cavity thus exposed were smoothed with a burr. Cleansing of the tympanic cavity was performed. The epithelium of the tympanic membrane was separated from the edges of the perforation using a micropick and the latter was closed with fascia, using the post-auricular approach. In patients with bone conduction thresholds better than 35 dB and an open eustachian ostium and a healthy peri-eustachian mucosa, a silastic sheet was placed tympanic caivity for second stage ossiculoplasty. The medial attic area was filled up with cartilage chips. The flap was given the functionality of a flexible metal watch belt to place it properly into the mastoid cavity and to let it reconstruct the canal wall. The loosened lining of the cavity was then spread evenly over the anterior surface of the periosteal flap and held in position by means of ear canal rosebud packing using a nylon mesh and antibiotic-impregnated Merocel (Medtronic, Minneapolis, Minestota, USA). The space behind the periosteal flap was obliterated using autogenous or homologous materials.
Preoperative and postoperative otoendoscopic examination was performed. Postoperatively, temporal bone computerized tomography (TBCT) scans were performed in 13 patients (14 ears) for second stage ossiculoplasty. Measurement of the otic capsule adjacent to the lateral semicircular canal, and the posterior fossa dural plate in the axial plane in Hounsfield Units (HU) was performed using picture archiving and communication system (PACS, Marotech M-View system, Seoul, Korea). Both ears of 21 patients (bone pate, n=11; costal cartilage, n=10) who underwent unilateral operation were evaluated after with the monothermal cold water caloric test using Frenzel goggles, and horizontal ocular beats to the contralateral side were continued for 60 seconds by video-nystagmography (ICS, Chartr 200, Otometrics, Taastrup, Denmark).
For statistical analysis, paired t-test was performed to assess the differences between the operated side and the normal side. The difference between the bone pate and costal cartilage groups was also examined.
Results
The male-to-female ratio was 0.6:1 and the mean age was 44.3 years (range=12-70 years). Most patients had mixed hearing loss. Among 50 patients, inferiorly based periosteal flap (IBF) was used in 25 patients (50%), and anteriorly based periosteal flap (ABF) was used in the other 25 patients. The mean time period for drying of the ABF was 3.5 weeks and that for drying of the IBF was 5.5 weeks.
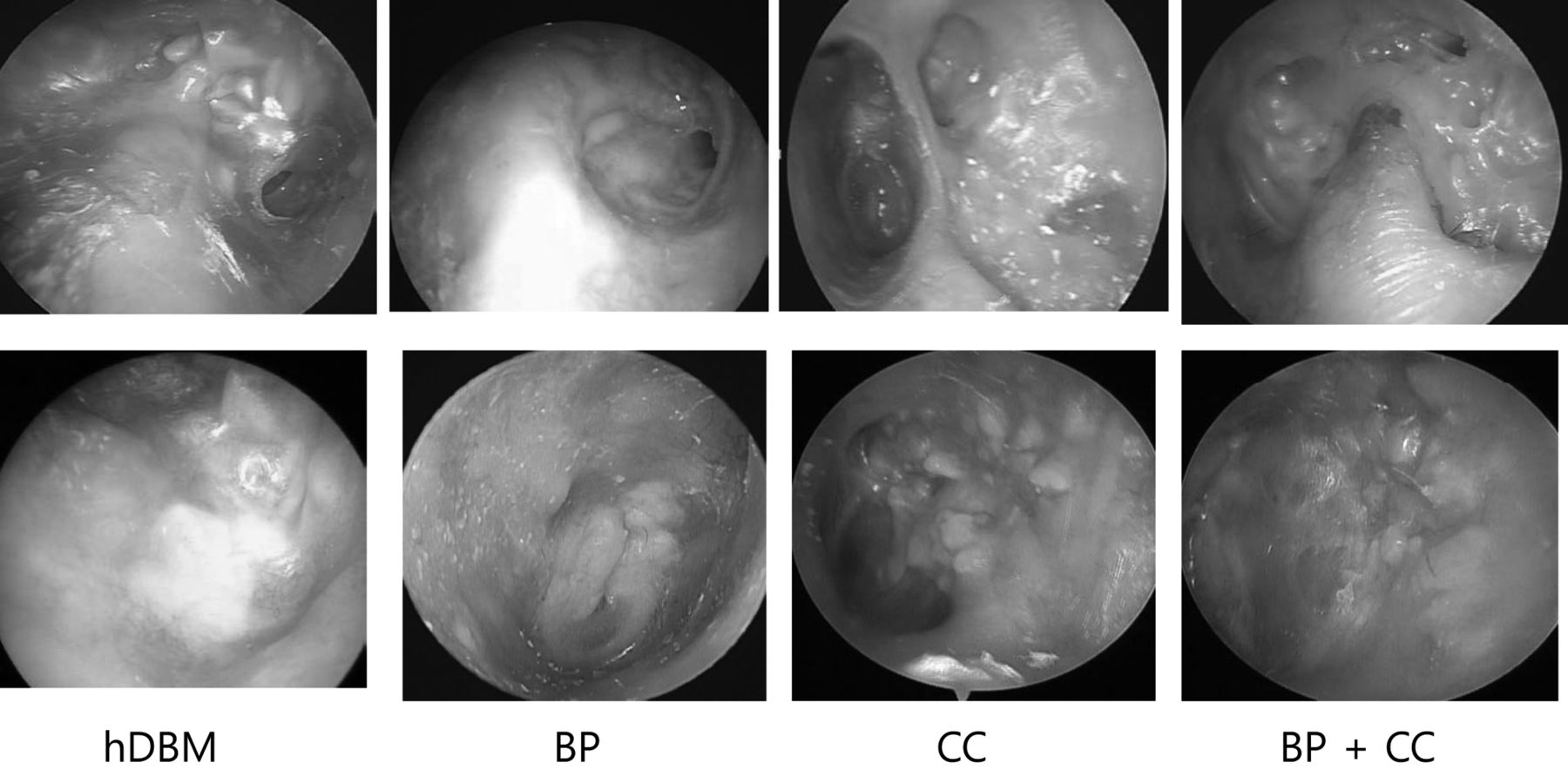
Preoperative and postoperative otoendoscopic findings. BP: Bone pate, hDBM: human demineralized bone matrix, CC: costal cartilage.
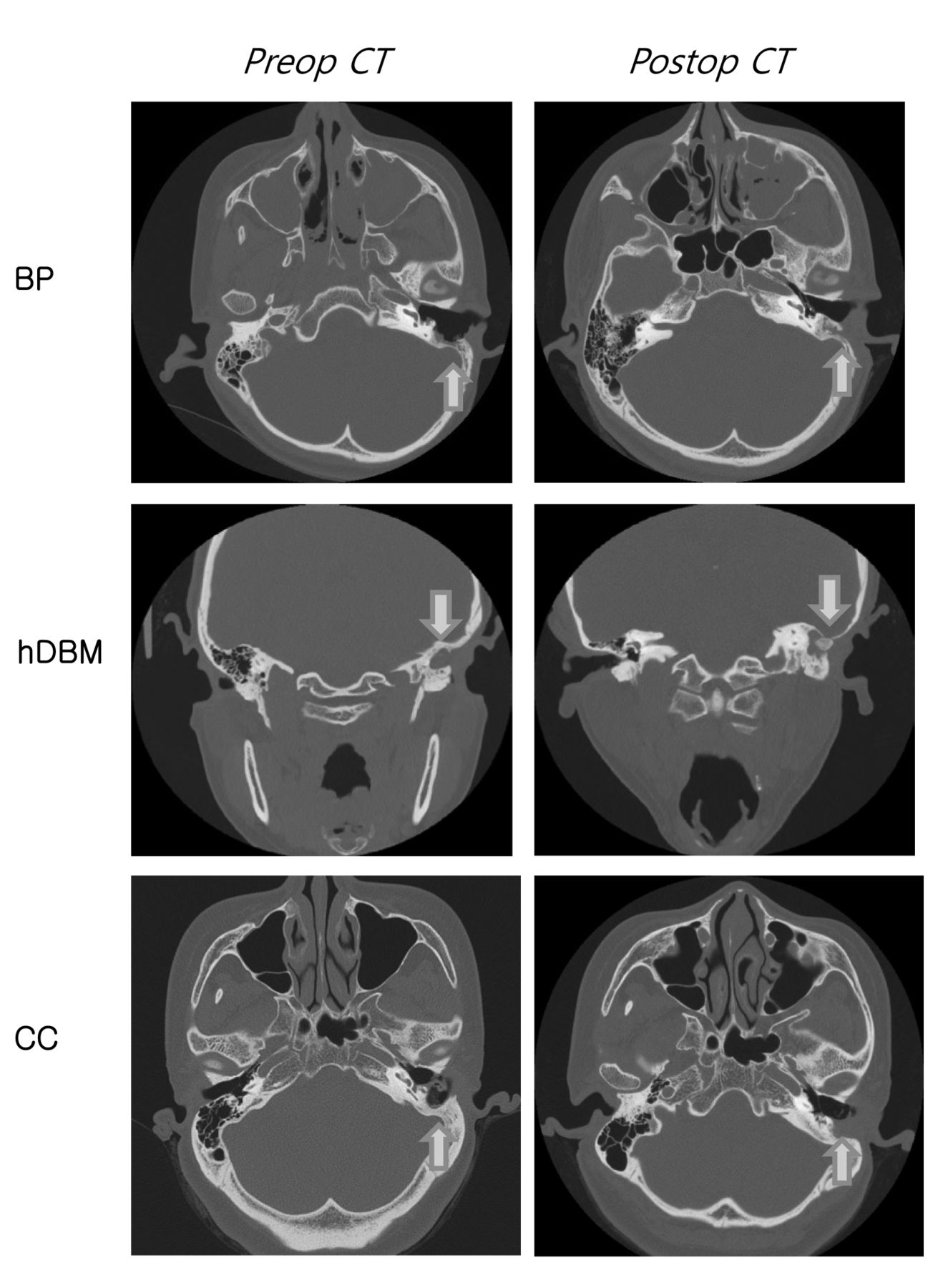
Mastoid obliteration was performed using bone pate (18 patients), costal cartilage (20 patients), costal cartilage chip covered with bone pate (seven patients), and homologous demineralized bone matrix (hDMB) (five patients) (Figure 1). Tympanic membrane and newly-formed external auditory canal (EAC) wall was intact in 48 patients (96%). Postoperative infection was found in one patient and mastoid cutaneous fistula was found in one patient. The fistula was repaired by using the periosteal flap and direct suturing. Partial defect of the posterior canal wall occurred due to necrosis of the soft tissue. After achieving infection control, the skin defect was treated by a collagen sheet. Two patients underwent revision tympanoplasty due to recurrent perforation of the tympanic membrane. To date, none of the patients with a recurrence have undergone further surgery. The newly-formed EAC provided sufficient aeration, and a preferable aesthetic appearance (Figure 2). None of our patients complained of vertigo triggered by cold air or water. The evaluation of the postoperative TBCT scanning revealed obliteration of the mastoid cavity (Figure 3). New bone formation in the mastoid cavity was found in the groups treated with autogenous bone pate group or hDMB group. In the bone pate group, new bone formation filling the mastoidectomy cavity was detected in the postoperative temporal bone CT images taken in the ninth to twelfth month. The average HU measurements in the bone pate group were higher than those in the other groups although the difference was not statistically significant (Figure 4). There was no significant difference in the caloric test results between the operated ear and the normal ear. No difference was observed in the caloric test results between the bone pate and costal cartilage-treated groups (Table I).
Results of monothermal caloric test.

Preoperative and postoperative temporal bone computed tomographic findings after the use of each material. BP: Bone pate, hDBM: human demineralized bone matrix, CC: costal cartilage.
Discussion
In the present study, we compared the results of mastoid obliteration using different materials.
Our results showed that mastoid obliteration with the use of any of these material is an efficient and long-lasting way to diminish the size of the open surgical cavity. In a study where Palva flap was used for mastoid obliteration, the ear canal was found enlarged at both the early and the late postoperative check-up compared to the preoperative values (9). We did not perform mastoid obliteration using only a musculoperiosteal or periosteal flap. Mastoid obliteration using autogenous bone pate combined with canal wall reconstruction tympanomastoidectomy, as originally described by Mercke (10), was highly recommended by Gantz et al. (11) to prevent postoperative formation of a retraction pocket.

Computed tomographic density assessed using Hounsfield unit (HU). The BP-treated group had a higher score than the other groups. There was a statistically significant difference between the BP and CC groups (p<0.05). BP: Bone pate, hDBM: human demineralized bone matrix, CC: costal cartilage.
Currently, we prefer to use a periosteal flap with bone pate or costal cartilage chips to line the CWD cavity to reduce the cavity size, thereby avoiding the problem of a large cavity. The use of an IBF or ABF depends on the surgeon's preference. In our experience, healing time of the ABF was less than that of the IBF. Bone pate is an autologous material that is readily available and easily used in primary and revision cases, and in our experience, it gives excellent results. Histological evidence shows that the bone pate becomes surrounded by fibroconnective tissue without inflammation (12). The use of autologous bone pate allows for greater bioresorption and is associated with less risk of subsequent breakdown of the reconstruction as compared with the use of heterologous materials (13). Because there is a possibility of bone pate being contaminated with infected mucosa or squamous epithelium, it should be collected only from the lateral cortical bone (14). We found that in some revision cases, the bone pate collected was not adequate enough to obliterate the cavity.
Autologous or homograft costal cartilage has been used for mastoid obliteration since 1986 (15). Sufficient amounts of autologous costal cartilage can be available but disadvantages of its use are postoperative pain, and difficulty in obtaining it in a child or virgin.
It is difficult to differentiate between recurrent cholesteatoma and cartilage shadow in postoperative TBCT scans. Diffusion-weighted magnetic resonance imaging is required for the differential diagnosis. In the present study, hDBM or hydroxyapatite granules were commonly used for mastoid obliteration. The bone pate combined with hDBM can be used in a child or virgin. The advantage of hDBM is that it is an osteoinductive material; therefore, the bioresorption period is shorter than that of osteoconductive bone scaffold such as hydroxyapatite granules or beta-tricalcium phosphate.
In the study by Dornhoffer et al., the vast majority of patients reported an improved quality of life after revision CWD mastoidectomy with mastoid obliteration for a draining cavity (16). Additionally, the acoustic properties of an obliterated cavity are considered to be better than those of an open cavity (17, 18). Introducing the hearing aids into the EAC was easy and almost natural. Mastoid obliteration reduces the postoperative frequency of vertigo after caloric stimuli such as wind, water, or suction cleaning (8).
There are certain limitations to this study. One of the limitations is that hearing results were not included because half of the original patients were lost to follow-up, and hence, follow-up hearing test could not be performed. Another limitation is the insufficient number of cases in which mastoid obliteration was performed using hDBM.
In the present study, we performed the postoperative caloric test in 21 patients. Because the preoperative caloric test was not performed, the difference between the operated ear and the normal ear was compared. There was no significant difference in the caloric test results between the normal and the operated ear. We also compared the bone pate and costal cartilage groups. There was no significant difference in the caloric test results between the two groups. Mastoid obliteration with bone pate or costal cartilage reduces postoperative dizziness on caloric stimulation. Results of the present study are in agreement with those of earlier studies (8, 16).
Conclusion
Our results indicate that mastoid obliteration using autogenous bone pate or costal cartilage is helpful in improving the outcomes of revision CWD mastoidectomy in patients with an old radical cavity and recurrent COM or cholesteatoma.
- Received August 11, 2014.
- Revision received September 22, 2014.
- Accepted September 29, 2014.
- Copyright © 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.