


Abstract
Lung resection is still the only potentially curative therapy for patients with localized non-small lung cancer (NSCLC). However, the presence of cardiovascular comorbidities and underlying lung disease increases the risk of postoperative complications. Various studies have evaluated the use of different preoperative tests in order to identify patients with an increased risk for postoperative complications, associated with prolonged hospital stay and increased morbidity and mortality. In this topic review, we discuss the role of cardiopulmonary exercise testing (CPET) as one of the preoperative tests suggested for lung cancer patients scheduled for lung resection. We describe different types of exercise testing techniques and present algorithms of preoperative evaluation in lung cancer patients. Overall, patients with maximal oxygen consumption (VO2max) <10 mL/kg/min or those with VO2max <15 mL/kg/min and both postoperative FEV1 and DLCO<40% predicted, are at high risk for perioperative death and postoperative cardiopulmonary complications, and thus should be offered an alternative medical treatment option.
- Lung resection
- non-small cell lung cancer
- comorbidities
- oxygen consumption
- forced expiratory volume
- cardiopulmonary exercise testing
- review
Lung cancer is one of the leading causes of death and is associated with poor prognosis, even when diagnosed in early stages (1). Lung resection is considered to be the only potentially curative treatment and remains the treatment of choice in early stage lung cancer (2). However, most lung cancer patients are elderly, smokers or have serious comorbidities, thus are excluded from surgery and directed toward medical or non-invasive treatments. Given the recent advances in operative techniques and perioperative care, which have considerably reduced surgical morbidity and mortality, an effort is being made to expand the group of candidates for surgical resection.
Postoperative cardiopulmonary complications include respiratory failure (acute respiratory distress syndrome, ARDS), prolonged postoperative mechanical ventilation or reintubation, pneumonia, atelectasis requiring bronchoscopy, myocardial infarction, and arrhythmias requiring intravenous treatment. Various single and combined parameters of functional operability have been proposed to assess the surgical risk. Pulmonary function tests adequately assess the pulmonary risk, and baseline or stress electrocardiography, echocardiography and nuclear cardiac studies assess cardiac risk. The cardiopulmonary risk index (CPRI), a multifactorial tool assessing cardiovascular and pulmonary parameters (e.g., obesity, cigarette smoking within 8 weeks of surgery, productive cough within 5 days of surgery, FEV1/FVC <70%, PaCO2), has been used in lung cancer patients scheduled for surgery and has also been found to be associated with a higher rate of postoperative complications (3).
The aim of the present review was to discuss the role of cardiopulmonary exercise testing (CPET) in the preoperative evaluation of patients scheduled to undergo lung resection. We searched MEDLINE (1962 to 2010) and EMBASE (March, 1974 to February, 2005) using the terms lung/surgery, lung resection/cancer, bronchogenic carcinoma, thoracotomy, pneumonectomy, exercise test, cardiopulmonary exercise testing and postoperative pulmonary complications. We augmented our search by reviewing the reference lists of retrieved articles, including review articles, as well as the reference lists of related articles in our files. Initially, pulmonary function tests traditionally used in the preoperative evaluation of lung cancer and split functions techniques are reported; subsequently, exercise capacity tests are described and discussed, and algorithms of preoperative evaluation of lung cancer patients are presented.
Pulmonary FunctionTests
Spirometry and maximum voluntary ventilation. Spirometry is a simple, inexpensive, standardized, and readily-available test. All patients scheduled for lung resection should have spirometry as a first step in the preoperative evaluation. Forced vital capacity (FVC), forced expiratory volume in one second (FEV1) and their ratio (FEV1/FVC) remain the most decisive indexes (4-6). Patients with a preoperative post-bronchodilator FEV1 >2.0 L or FEV1 >80% predicted are considered operable for pneumonectomy, while a preoperative FEV1 >1.5 liters permits lobectomy (7-10) and FEV1>0.6 L permits wedge or segmental resection (10) without further testing. Furthermore, patients with a maximum voluntary ventilation (MVV) <50% predicted (4, 5) are considered high-risk patients for post-pneumonectomy complications, while the cut-off point for lobectomy is 40% predicted (6).
Diffusion capacity. Diffusing capacity of the lung for carbon monoxide (DLCO) reflects alveolar membrane integrity and pulmonary capillary blood flow in the patient's lungs. In a retrospective study of 247 patients by Ferguson and colleagues (12), DLCO was found to be the most important predictor of mortality and the sole predictor of postoperative pulmonary complications. In a meta-analysis by Benzo et al. (13), preoperative DLCO values were significantly higher in patients without postoperative complications versus those with postoperative complications. Patients with preoperative DLCO <50% predicted (14) or 60% predicted (4, 6, 10, 12) should not be submitted to major pulmonary resections, as they are associated with increased risk of postoperative complications. According to the ERS guidelines, DLCO should be routinely measured in all patients scheduled for pulmonary resection, regardless of normal spirometric values (9) and DLCO >80% predicted permits pneumonectomy without further tests needed (provided that FEV1 is also greater than 80% predicted).
Arterial blood gas levels. Arterial blood gas (ABG) levels have not been extensively studied as a predictor of postoperative complications. It has been suggested that an arterial oxygen tension of <50 mmHg (15) or 60 mmHg (14) is associated with an increased risk of post-resection complications. Also, hypercapnia (i.e., PCO2 >45 mm Hg) has been considered a relative contraindication to lung resection as it indicates chronic respiratory failure (4,10). However, several studies have shown that a preoperative PCO2 value of >45 mm Hg is not an independent predictor of postoperative complications (16-18).
Split-functionStudies
According to the ACCP and BTS guidelines (7, 8), patients with normal pulmonary function, as defined by FEV1 ≥80% predicted and DLCO ≥80% predicted, can undergo major lung resections without further investigation. Patients with FEV1 and/or DLCO <80% should not be excluded from surgery, but further evaluated. Split function studies predict postoperative pulmonary function (mainly postoperative FEV¬1 and DLCO) through either quantitative ventilation-perfusion scanning results or through formulas involving bronchopulmonary segments to be resected.
In quantitative ventilation-perfusion scan, Xe is inhaled or 99Tc-labeled macroaggregates are injected intravenously. The uptake of radioactive ions by the lung by inhalation of the 133Xe or perfusion of the 99Tc macroaggregates is measured by a gamma camera and processed by a computer. The percentage of radioactivity contributed by each lung correlates with the contribution to the function of that lung. Normally, the right lung contributes to 55% of lung function, while the left lung to 45% of lung function. Based on the measured radioactive uptake of the lung that will not be operated on, the predicted FEV1 of the residual lung following surgery was calculated by Kristersson et al. (19) using the following formula:
 According to Kristersson and coworkers (19), a predicted postoperative (ppo) FEV1 of <1 L is indicative of physiologic inoperability, while others lower the cut-off point to 800 mL (5).
According to Kristersson and coworkers (19), a predicted postoperative (ppo) FEV1 of <1 L is indicative of physiologic inoperability, while others lower the cut-off point to 800 mL (5).
Wernly and colleagues (20) developed and tested the following formula for predicting postlobectomy pulmonary function using ventilation-perfusion scanning:
 No prospective study has established a cut-off limit of ppo-FEV1 that precludes a safe resection. Markos and colleagues (21) found that a higher mortality rate was associated with ppo-FEV1 <40%. Gass and Olsen (22) suggested a ppo-FEV1 of <35% of predicted as a low threshold for all patients. Several investigators have reported that the simple calculation using lung segment counting can predict postoperative FEV1 as accurately as ventilation/perfusion scintigraphy (23-26), while perfusion scintigraphy is the most widely used method to predict postoperative lung function in patients undergoing pneumonectomy (7, 8).
No prospective study has established a cut-off limit of ppo-FEV1 that precludes a safe resection. Markos and colleagues (21) found that a higher mortality rate was associated with ppo-FEV1 <40%. Gass and Olsen (22) suggested a ppo-FEV1 of <35% of predicted as a low threshold for all patients. Several investigators have reported that the simple calculation using lung segment counting can predict postoperative FEV1 as accurately as ventilation/perfusion scintigraphy (23-26), while perfusion scintigraphy is the most widely used method to predict postoperative lung function in patients undergoing pneumonectomy (7, 8).
Other tests assessing differential lung function include bronchospirometry, lateral position testing, and total unilateral pulmonary artery occlusion (27). All are invasive methods, and require specialized equipment and a high level of technical expertise for their performance. For these reasons, and given the advantages of ventilation-perfusion scanning, these tests are no longer performed in the preoperative evaluation of patients who are awaiting lung resection.
Exercise Testing
Cardiopulmonary exercise testing is based on the principle that system failure occurs while the system (muscle-energetic, cardiovascular or pulmonary) is under stress (28). Cardiac output, ventilation, oxygen uptake and carbon dioxide output increase during exercise and in proportion to the severity of exercise. Since CPET stresses the entire cardiopulmonary and oxygen delivery system while monitoring cardiopulmonary variables (such as minute oxygen uptake - VO2, minute pulmonary CO2 output - VCO2, minute ventilation - VE, cardiac frequency), it evaluates cardiopulmonary status and function under stress and provides a good estimate of cardiopulmonary reserve. And since both thoracotomy and the immediate postoperative period represent a severe stress for both the circulatory and respiratory reserve, preoperative exercise should be evaluated as a predictor of post-thoracotomy morbidity and mortality (26).
Types of Exercise Testing
Two major types of exercise tests have been used in the preoperative evaluation of high-risk patients being considered for lung resection surgery. These are: (1) incremental exercise testing, in which the work rate is sequentially increased to a desired end-point, and (2) fixed exercise challenge, in which a sustained level of work is performed. These two types are further divided into maximal or sub-maximal, based on their end-points. The maximal end point can be defined as an exercise, usually incremental, that is performed until a plateau (i.e., VO2max) is reached at which further work will not produce any increase in VO2. The submaximal end point can be defined as exercise performed short of achieving the plateau (maximum VO2 attained, thus designated VO2 peak).
Maximal exercise testing. Eugene and colleagues (29) were the first to use incremental exercise to the point of maximal exertion and measure VO2max in patients being evaluated for lung resection surgery. They found that no death occurred in patients with VO2max values of >1 L/min, while the mortality rate was 100% in those with VO2max<1 L/min. They reported that VO2max during symptom-limited exercise was a better predictor of post-operative mortality than FEV1 and FEV1/FVC. Smith and colleagues (30) reported significantly more postoperative complications in patients with VO2max <15 mL/kg compared to patients with VO2max >20 mL/kg. With this study the researchers demonstrated that VO2 at peak exercise was a valuable non-invasive method of preoperative evaluation and they introduced the value of 20 mL/kg/min as a cut-off point for operability. Berggren and colleagues (31) reported a postoperative mortality rate of 7.7% in 26 patients who completed 83 Watts of work for 6 min versus a postoperative mortality rate of 22% in the remaining 18 patients who were unable to perform that amount of work.
In 1992, Bechard and Wetstein (32) studied 50 patients that underwent exercise testing by cycle ergometry, with 1-min increments of 12.5 Wattsuntil exhaustion or dyspnea occurred, while measuring VO2max and anaerobic threshold. The postoperative mortality rate was 4%, and it occurred in all patients with VO2max levels of <10 mL/kg/min. Based on these results, the authors propounded that a patient with VO2max values of <10 mL/kg should not undergo lung resection surgery. In the same year, Morice et al. (16) measured exercise capacity in 37 patients during an incremental exercise test on cycle ergometer and reported that even in patients with FEV1<40%, ppo-FEV1<33% or PaCO2>45 mmHg, the prognosis is excellent when VO2max is >15 mL/kg/min. The same authors in 1996 (33) found that VO2max ≥50% was a better predictor of operability than VO2max ≥15mL/kg/min. On the other hand, Smith and coworkers (30) had earlier analyzed VO2max as a percentage of predicted normal values and found it to be inferior to absolute values in predicting postoperative complications. Bechard and Wetstein (32) and Smith et al. (30) set a lower cut-off value of 20 mL/kg/min for pneumonectomy.
In 1993, Epstein et al. (3), using an incremental exercise protocol, reported that patients with a VO2max per body surface area (BSA) <500 mL/min/m2 were 6 times more likely to experience a cardiopulmonary complication (p<0.05), while VO2max was not found to be an independent predictor of postoperative complications.Pate and colleagues (34) also suggested that patients with VO2max >10 mL/kg/min could safely undergo lung resection surgery. However, Markos and colleagues (21) in their study observed that VO2max was significantly lower in patients with postoperative complications compared to those without complications, but they found that oxygen desaturation during a 12-min walk, ppo-DLCO, and ppo-FEV1 were more reliable predictors of postoperative mortality than VO2max. Bolliger and colleagues (35)studied 25 patients at increased risk for postoperative complications (FEV1<2L or DLCO<50% or FEV1 and DLCO ≤80% and NYHA [New York Heart Association] index ≥2) and observed that patients with postoperative complications had a significantly lower preoperative VO2max (p<0.01) and postoperative VO2max (ppo-VO2max, p<0.05); they reported that VO2max, expressed as a percentage of the predicted value, was the single best predictor of postoperative complications.
More recently, in 2005, Win et al. (26), in a prospective study involving 99 patients who were submitted to a symptom-restricted treadmill exercise test prior to lung cancer surgery, reported that VO2max percentage, but not the absolute oxygen uptake values, was significantly related with postoperative complications and a poor surgical outcome. In 2007, in a prospective multi-institutional study by Loewen et al. (36), subjects underwent a symptom-limited incremental ramp workload exercise on a cycle ergometer; patients with VO2max <65% predicted were more likely to suffer complications (p=0.0001) and had a poorer outcome (p=0.0356).
Using the formula for calculating postoperative FEV1 based on radionuclide ventilation-perfusion scanning, Corris and colleagues (37) were able to predict postoperative VO2max. Bolliger and colleagues (38) used this formula to estimate ppo-VO2max in a group of 25 patients, and reported a good correlation between estimated ppo-VO2max and measured postoperative VO2max values. The value of ppo-VO2max needs to be studied prospectively to establish its utility in the preoperative assessment of patients prior to lung resection surgery.
Submaximal Exercise Testing
Submaximal exercise testing is particularly useful in patients who are unable to tolerate exercise stress due to dyspnea or fatigue, such as elderly or COPD patients, and might therefore not be motivated to perform exercise to exhaustion (10). During submaximal CPET, the patient is submitted to a designated sub-maximal workload exercise for a specific period of time, while various parameters, such as oxygen uptake, ventilation volume, carbon dioxide output, carbon dioxide and oxygen arterial pressures and lactate levels, are measured. In these studies, VO2 peak is used instead of VO2max, i.e. the maximum attained oxygen consumption before it reaches a plateau.
In 1989, Olsen and colleagues (39) studied 52 elderly male patients with a lung mass and FEV1 <2.0L who were scheduled for lung resection, and submitted them to cycle ergometry at two sub-maximal workloads (25 and 40 Watts). Patients were also catheterized with a flow directed balloon-tipped pulmonary artery catheter for the measurement of pulmonary arterial pressure and pulmonary vascular resistance. The authors found that variables significantly associated with postoperative complications were cardiac index (i.e., cardiac output/body surface area; p<0.01), oxygen delivery (p<0.01) and calculated VO2 (p<0.001).
Nakagawa et al. (40) evaluated oxygen transport in thirty-one lung cancer patients during incremental sub-maximal exercise under right heart catheterization. Their assumption followed a previous proposal that oxygen consumption per body surface area at an arterial lactate level of 20 mg/dl (VO2/BSALa20) is a risk predictor following thoracotomy (41, 42).
Miyoshi and colleagues (41) studied 33 patients undergoing thoracotomy using cycle ergometry to submaximal levels (reaching a heart rate of 140 beats/min or a respiratory quotient - carbon dioxide eliminated/oxygen consumed - of >1) with arterial lactate levels measured during the last 3 seconds of each work rate period. They found that VO2/BSALa20 was significantly different between survivors and nonsurvivors and that the blood lactate threshold expressed by VO2/BSA at La-20 was an important indicator of the risk of hospital mortality. They also found that pulmonary function parameters such as FEV1/BSA, FEV1/FVC, DLCO/lung volume, and MVV/BSA showed significant differences between patients with post-thoracotomy pulmonary complications and those without such complications. This study suggested that in-house mortality could be predicted by submaximal exercise VO2 when the work level achieved was corrected for a fixed level of lactate production.
Fixed challenge exercise testing. Fixed challenge exercise testing involves assessing performance status by doing a fixed amount of work, such as climbing a certain number of stairs or walking a fixed distance. Long before the introduction of pulmonary function tests, surgeons evaluated their patients' preoperative functional status by asking them to climb flights of stairs. Following that observation, several studies were performed based on the assumption that the number of flights climbed can serve as an indicator of cardiopulmonary reserve and of the patient's ability to tolerate pre- and postoperative cardiopulmonary stress. Van Nostrand and colleagues first used stair climbing as a test for endurance in the preoperative evaluation of 119 patients scheduled for lung surgery (43). He reported a postoperative mortality rate of 50% in patients who were unable to climb one flight of stairs with minimal dyspnea compared to a mortality rate of 11% in those able to climb two flights of stairs with minimal dyspnea.
Holden and colleagues (44), in a prospective study of sixteen patients at increased risk submitted to stair climbing as part of the evaluation prior to surgery, reported that 5 of the 16 patients who died in the perioperative period had a significantly shorter 6-min walk distance test and a smaller number of stairs climbed than patients with minor or no complications. They found that a 6-min walking test distance of >1,000 ft or >44 steps of stair climbing were predictive of successful surgical outcome. Olsen et al. (45) suggested that patients able to climb 5 flights of stairs could be submitted to pneumonectomy, while patients climbing at least 3 flights of stairs could undergo lobectomy. Girish and colleagues (46) prospectively evaluated the role of symptom-limited stair climbing as a predictor of postoperative cardiopulmonary complications in 83 patients undergoing thoracic and upper abdominal surgery. They found that complications occurred in 89% of patients who were unable to climb one flight of stairs. The inability to climb two flights of stairs had a positive predictive value of 80%, while the inability to climb five flights of stairs had a positive predictive value of 32%. No complications were seen in patients that could climb seven flights of stairs. The ability of patients to climb stairs was inversely related to the length of postoperative hospital stay. The number of stairs climbed was a strong predictor of postoperative complications (p=0.00002), along with FEV1 (p=0.02) and FVC (p=0.04). Although stair climbing as a measure of exercise capacity could predict postoperative complications, more studies are needed to determine whether it can supplant more sophisticated exercise testing.
A disadvantage of stair climbing in the preoperative evaluation of patients is that it is not a standardized method, e.g., the height of stairs climbed varies in different Institutions. Having this in mind, Pollock et al. (47) in 1993 standardized stair climbing (height and width of steps, number of steps per floor) and reported that an achievement of 4.6 flights (83 steps) corresponded to a VO2 of 20 mL/kg/min. Pate et al. (34) expressed the number of steps climbed as height climbed in meters to provide standardization. When this standardized value was applied in elderly patients undergoing lobectomy, it proved to be an important predictor of post-operative cardiopulmonary complications (48). Koegelenberg et al. (49) have proposed standardizing stair climbing by looking at the speed of ascent and not just height achieved.
The 6-min walk distance test and shuttle walk test are two other methods used for the preoperative evaluation of cardiopulmonary reserve (50, 51). During 6-min walk test, patients are instructed to walk as far as possible in 6 min. According to Holden and colleagues (37), a 6-min walk distance >1000 ft is associated with a good surgical outcome. However, the results of other studies have been inconsistent (52, 53).
In the shuttle walk test, patients walk a distance of 10 m between two shuttles. When the patient is too breathless to proceed or cannot keep up with the pace, the test is ended. Patients who cannot complete 25 shuttles on two occasions are considered to have a VO2max of <10 mL/kg/min (54, 55). According to Brunelli (9), stair-climbing could be used for selecting patients, but not the shuttle walk or the 6-min walk tests. On the other hand, both the BTS and ACCP guidelines recommend the use of the incremental shuttle walk test (ISWT) because it is reproducible, correlates well with VO2max and can serve as a good alternative if CPET is unavailable (7, 8).
Conclusion
Patients diagnosed with anatomically-resectable lung cancer should be evaluated for surgical operability. Pneumonectomy has a significantly higher rate of complications and mortality than lobectomy (56), thus the selection of lung resection candidates and treatment modality should be performed prudently. Over the last years, a considerable number of studies have focused on preoperative evaluation methods in order to identify lung cancer patients who would more likely benefit from surgery. The analysis of the results and conclusions of these studies has led to official statements and issued guidelines by the British Thoracic Society (BTS), the American College of Chest Physicians (ACCP) and the European Respiratory Society (ERS) (7, 8, 9).
According to the guidelines of the British Thoracic Society (7), no further respiratory function tests are required if FEV1>2 lt (for pneumonectomy) and >1.5 lt (for lobectomy), provided there is no evidence of interstitial lung disease or shortness of breath (20). In every other case, DLCO should be measured and the patient should undergo split-function studies (using the perfusion scanning method), in order to estimate postoperative FEV1 (ppo-FEV1) and DLCO (ppo-DLCO) predicted as a percentage of the absolute normal values. If both ppo-FEV1and ppo-DLCO are >40% predicted, no further tests are required, the patient is considered average risk and can safely undergo the suggested operation. If both ppo-FEV1 and ppo-DLCO are <40% predicted, the patient is considered inoperable (18, 21, 34, 37). If any of ppo-FEV1 or ppo-DLCO is <40%, BTS guidelines suggest shuttle walk test and, if the patient achieves >25 shuttles with <4% desaturation, a full cardiopulmonary exercise test (57). If VO2max is >15 mL/kg/min, the patient is operable to the extent of resection calculated; if VO2max is<15 mL/kg/min, the patient is considered inoperable(16, 21, 30, 32, 35).
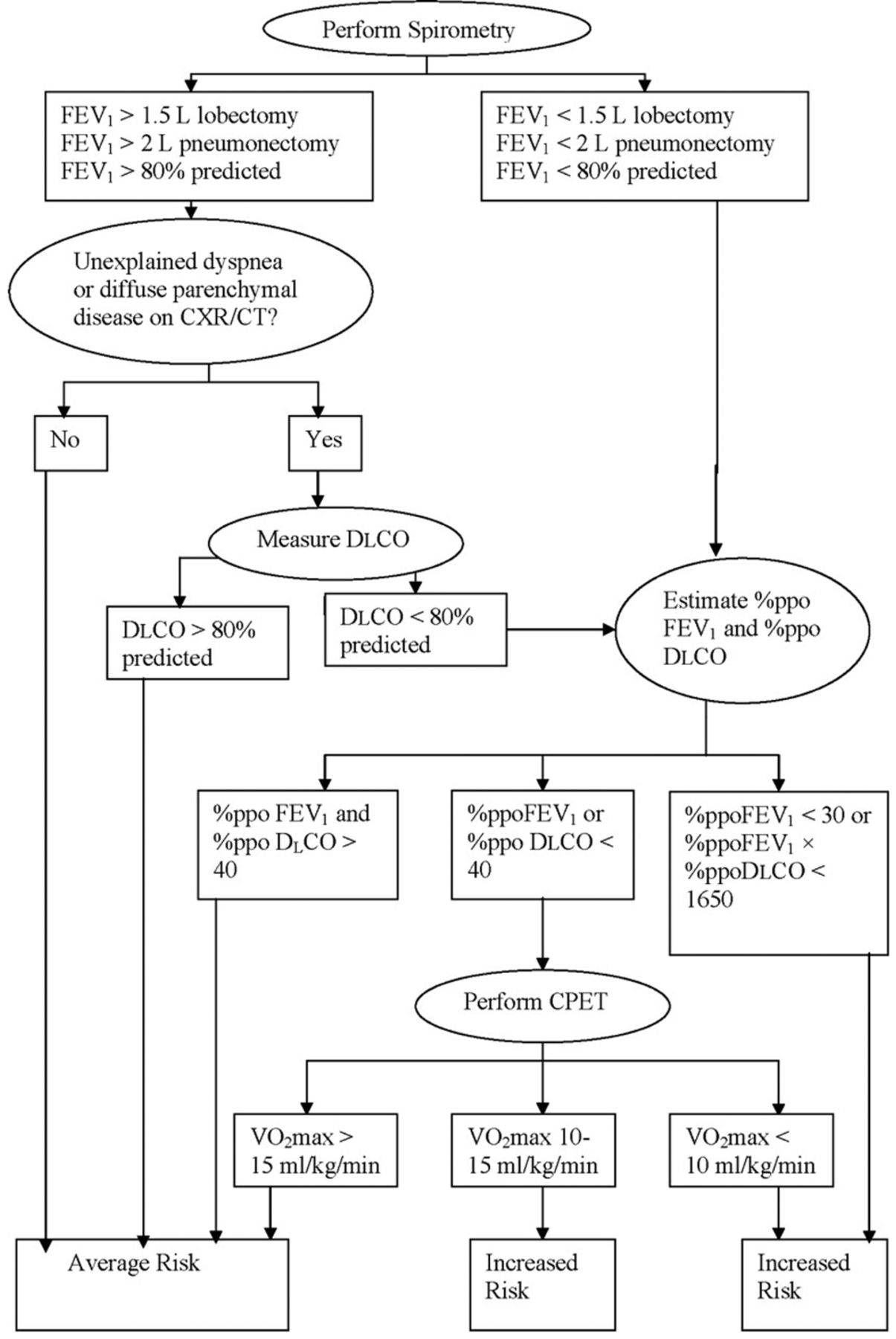
The guidelines of the American College of Chest Physicians (ACCP) (8) issued in 2007 are similar to those of BTS, with the exception of the shuttle walk test, which they have omitted (Figure 1). According to these guidelines, also based on previous studies, in patients with lung cancer being considered for lung resection, VO2max<10 mL/kg/min indicates a very high risk for perioperative death and cardiopulmonary complications (21, 32, 37, 39). These patients should be given non-operative treatment options. Patients being considered for lung cancer resection, who have VO2max<15 mL/kg/min and both a %ppo-FEV1 and DLCO<40% should be considered at very high risk for perioperative death and cardiopulmonary complications (21, 26, 30, 32, 35, 37, 39). These patients should be counseled about non-operative treatment options for their lung cancer. Patients being considered for lung cancer resection who walk <25 shuttles on two occasions or less than one flight of stairs should be considered as very high risk for perioperative death and cardiopulmonary complications (53). These patients should be counseled about non-operative treatment options for their lung cancer.

Guidelines of ERS for the preoperative evaluation of lung cancer patients. FEV1, forced expiratory volume in 1 second; CXR, chest X-ray; CT, computerized tomography; DLCO, diffusing capacity of the lung for carbon monoxide; ppoFEV1, predicted postoperative forced volume in 1 second; ppoDLCO, predicted postoperative diffusing capacity of the lung for carbon monoxide; CPET, cardiopulmonary exercise testing; VO2max, maximum oxygen uptake (9).
The European Respiratory Society (ERS) guidelines present a slightly different approach to the preoperative evaluation of lung cancer patients (9). The authors suggest that exercise testing should proceed to split function studies. They set a cut-off point for VO2max of >20 mL/kg/min or 75% predicted for pneumonectomy and <10 mL/kg/min or 35% predicted for non-operability; patients with VO2max 35-75% or 10-20 mL/kg/min should undergo split function tests (16, 26, 30, 34-36). If both ppo-FEV1 and ppo-DLCO are >30% predicted, the patient can be submitted to resection up to the calculated extent (18, 21, 35, 44). If at least one is <30% predicted, ppo-VO2max should be calculated; a ppo-VO2max >35% predicted or 10 mL/kg/min permits resection up to the calculated extent, while a ppo-VO2max<35% predicted or 10 mL/kg/min renders the patient inoperable (35) (Figure 2). ERS guidelines also suggest that if VO2max is unavailable, cardiopulmonary exercise test could be replaced by stair climbing; but if a minimum height of 22 m cannot be achieved, full cardiopulmonary exercise test is highly recommended (43, 44, 45).

Guidelines of ACCP for the preoperative evaluation of lung cancer patients. FEV1, forced expiratory volume in 1 second; DL, CO, diffusing capacity of the lung for carbon monoxide; peak VO2, peak oxygen uptake (alternative for VO2max); ppo-FEV1, predictive postoperative forced expiratory volume in 1 second; ppo-DL,CO, predicted postoperative diffusing capacity of the lung for carbon monoxide; ppo-peak VO2, predicted postoperative peak oxygen uptake (alternative for ppo-VO2max) (8).
This is not a systematic review as no statistical analysis was conducted. However, in their majority, the results of studies presented are clear in showing that cardiopulmonary exercise testing provides an overall assessment of the patient's ability to tolerate lung resection, as it simulates the post-resection status of the remaining lung. It is now evident that some patients once excluded from surgery based on FEV1 and FVC or DLCO results, could undergo surgery, a potentially curative treatment, if CPET permits it. That is why the conclusions of these studies are incorporated in the abovementioned guidelines issued by BTS, ACCP and ERS regarding the preoperative evaluation of lung cancer patients. Cardiopulmonary exercise testing is performed in a controlled environment with continuous monitoring of several parameters and ensures early standardization and good reproducibility of results. However, its widespread use is limited by the low availability of appropriate equipment and well-trained personnel.
Footnotes
-
Conflicts of Interest
Authors have no conflicts of interest to declare.
- Received July 21, 2014.
- Revision received September 29, 2014.
- Accepted October 6, 2014.
- Copyright © 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Association of preoperative spirometry tests with postoperative pulmonary complications after mediastinal mass resection: protocol for a retrospective cohort study
- Cardiopulmonary exercise testing: A contemporary and versatile clinical tool
- Karnofsky Performance Score, Radiation Dose and Nodal Status Predict Survival of Elderly Patients Irradiated for Limited-disease Small-cell Lung Cancer
- 2016 Focused Update: Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations
- Defining the Optimal Dose of Stereotactic Radiosurgery for Treating Cerebral Metastases in Elderly Patients