


Abstract
Aim: To test whether melatonin reduces oxidative and inflammatory biomarkers in a closed-chest porcine model of acute myocardial infarction. Materials and Methods: Twenty pigs were randomized to receive a total dosage of 200 mg (0.4 mg/ml) of melatonin, or placebo immediately prior to reperfusion of a coronary artery balloon occlusion in a randomized, observer-blinded, placebo-controlled trial. We assessed high-sensitivity troponin T (hs-TnT), malondialdehyde and interleukin-1b, -6 and -10 at baseline, 30 min and 1, 2, 3 and 4 h after the start of reperfusion. Results: Seventeen pigs completed the trial. There was an increase in hs-TnT, but no significant difference between the melatonin-treated and placebo-treated groups. There were no significant differences in development of any of the circulating plasma markers between the two groups. Conclusion: Melatonin treatment did not result in reduction of inflammatory or oxidative stress markers after experimental myocardial infarction compared to placebo.
Coronary heart disease and its most severe presentation, acute ST-segment elevation myocardial infarction (STEMI) is the leading cause of mortality and morbidity in the Western world (1). Primary percutaneous coronary intervention (pPCI) with restoration of coronary blood flow is considered the optimal treatment-of-choice for STEMI (2). However, the restoration of blood flow and concomitant re-oxygenation of myocytes are frequently associated with an exacerbation of tissue injury and a profound inflammatory response called reperfusion injury (3).
Melatonin, (N-acetyl-5-methoxytryptamine), an endogenous circadian hormone secreted by the pineal gland, is known to protect against oxidative stress due to its direct free radical-scavenging of reactive oxygen species (ROS) and its indirect antioxidant actions by up-regulating antioxidant enzymes and down-regulating pro-oxidant enzymes (4). Melatonin possesses anti-inflammatory properties (4) and previous experimental studies have shown it to reduce myocardial ischemia-reperfusion (IR) injuries (5). In combination with its low toxicity (6), this makes melatonin a promising candidate with regard to potential treatment of IR injuries.
The aim of the present study was to analyze the circulating levels of oxidative (malondialdehyde, MDA) and inflammatory [interleukin (IL)-1β, IL6 and IL10] biomarkers in a porcine closed-chest model of STEMI and examine whether intracoronary and systemic melatonin could reduce these markers following reperfusion of the ischemic myocardium.
Materials and Methods
The present study reports secondary outcomes from a randomized, double-blind, placebo-controlled trial that primarily examined the cardio protective effect of intracoronary (i.c.) and intravenous (i.v.) melatonin in a clinically relevant in vivo closed-chest porcine model of myocardial ischemia, during experimental STEMI and reperfusion assessed by cardiac magnetic resonance (CMR) as will be reported in another article (data not reported here).
Experimental procedure. In the closed-chest porcine model, we used a group of 20 normally-fed, female, Danish Landrace pigs. The pigs were premedicated with 4 ml intramuscular (i.m.) Zoletil (6.25 mg/ml ketamine, 6.25 mg/ml tiletamin, 6.25 mg/ml zolazepam, 1.25 mg/ml butorphanol and 6.5 mg/ml xylazin), intubated with cuffed endotracheal tubes and mechanically ventilated with FiO2 0.5. The ventilation was adjusted to obtain normocapnia (pCO2 4-6 kPa). Anesthesia was maintained by inhalation of 1% isoflurane and analgesia was assured by continuous infusion of 5 μl/ml fentanyl and 5 μl/ml midazolam at a rate of 8 ml/min, adjusted if needed. Throughout the study, the pigs were continuously monitored by electrocardiography, pulse oximetry and central body temperature. Access to the central venous system was assured with a 7 Fr introducer sheath in the femoral vein. Prior to arterial catheterization, unfractionated heparin (single bolus, 5,000 units) was administered i.v. During the pre-ischemic period, baseline values were recorded.
Under X-ray guidance, a 6 Fr PCI-guiding catheter inserted through a 9 Fr introducer sheath was placed in the left coronary ostium through the femoral artery. A baseline coronary angiogram was performed using the contrast agent Iomeron (300 mg/ml). An over-the-wire 6 Fr PCI-catheter (Apex OTW balloon catheter; Boston Scientific, Natick, MA, USA) was placed in the left anterior descending artery or the circumflex coronary artery under X-ray guidance. Under angiographic control, absolute ischemia was induced by inflation of the angioplasty balloon at submaximal, but just occlusive pressure. The occlusive inflation of the balloon was kept unchanged for 45 minutes. If the animals during the experimental protocol suffered from ventricular fibrillation a biphasic defibrillator (360 J) was used for cardioversion. Changes in the electrocardiogram additionally verified the occlusion. Following 45 min of total occlusion, the myocardium was reperfused for four hours before the animal was euthanized and the heart was explanted.
Intervention procedure. The 20 pigs were randomized to receive either i.v. and i.c. melatonin (0.4 mg/ml) approximately 5 mg/kg, or i.v. and i.c. placebo (isotonic saline, 0.9 mg/ml). Five minutes prior to reperfusion an i.v. infusion of 198 mg melatonin diluted in isotonic saline (0.4 mg/ml) or placebo, 495 ml isotonic saline, was started. Total i.v. infusion time was 30 min. One minute prior to reperfusion a bolus of 5 ml containing 2 mg melatonin diluted in isotonic saline (0.4 mg/ml) or placebo, 5 ml isotonic saline, was slowly injected through the central lumen of the over-the-wire catheter directly into the coronary artery. Total i.c. infusion time was 2 min and the infusion lasted during the first minute of reperfusion. Throughout the study, the experimenters were blinded with regard to the drug administered.
Blood sampling. Blood samples were collected from a catheter in the femoral vein at baseline at 30 min and 1, 2, 3 and 4 h after the start of the reperfusion and analyzed for high-sensitivity troponin T (hs-TnT), oxidative stress marker, MDA, and inflammatory markers, IL1β, IL6 and IL10.
Hs-TnT in blood samples. For the determination of hs-TnT, the levels in plasma were analyzed immediately after sampling. We used the Cobas e 601 instrument (Roche Diagnostic, Hvidovre, Denmark) with a detection range of 3-10,000 ng/l.
Oxidative stress markers in blood samples. For the determination of the concentration of MDA, blood was drawn into tubes containing heparin-free lipopolysaccharide and centrifuged at 3,100 rpm (3,000 G) for 3 min and then stored at −80°C until analysis. MDA was analyzed using a high-performance liquid chromatograph method as described previously (7).
Inflammatory markers in blood samples. For the determination of pro- and anti-inflammatory cytokines, blood was drawn into tubes containing EDTA, and centrifuged at 3,100 rpm (3000 G) for 3 min and then stored at −80°C until analysis. IL6 and IL1βconcentrations in serum were determined by sandwich enzyme-linked immunosorbent assays from R&D Systems Europe Ltd, Abingdon, Oxon, United Kingdom (Duoset DY686, Duoset DY681 and Duoset DY693B, respectively). These use goat anti pig IL6/IL1β/IL10 for catching, and biotinylated goat anti pig IL6/IL1 β /IL10 for detection including a porcine IL6/IL1β/IL10 standard. Development of plates was done with a tetramethylbenzidine peroxide color substrate from KemEnTec (Taastrup, Denmark), following the manufacturer's instructions. Samples were run in duplicates in a dilution of 1:2 with a detection limit of 62.5 pg/ml (IL6), 31.3 pg/ml (IL1β), and 46.9 pg/ml (IL10).
Ethics. The study was performed in accordance with the Guide for the Care and Use of Laboratory Animals (NIH publication no. 85-23, revised 1996) (8) and approved by the Danish Animal Experiments Inspectorate, license no. 2012-15-2934-00583.
Sample size. The sample size calculation for the primary outcome (CMR) was based on a previous trial reporting primary outcome (infarct size relative to the area at risk), assessed by ex vivo CMR imaging. Primary outcome was reduced from 74.1±8.2 % to 58.3±9.6% of the area at risk (mean±SD, SD converted from SEM) (9). With a power of 90% and a type I error of 5%, a sample size of seven pigs were needed in each treatment arm. We chose to include 10 pigs in each group, due to an expected waste of one or two pigs in each arm.
For the secondary outcomes reported in this article, we conducted a post-hoc sample size calculation based on MDA in plasma measured at reperfusion in an open-chest porcine model (10). This study reported a mean±SD of 3.55±0.18 and 3.3±0.13 nmol MDA/l for the control group and intervention group, respectively. Thus, with a power of 90% and a type I error of 5%, the sample size calculation revealed that we would need 18 pigs in total, nine in each arm.
Statistics. Data were analyzed using non-parametric methods after testing for normality using the Kolmogorov-Smirnov test. Data for change over time were analyzed using Friedman analysis of variance and data between groups were analyzed using Mann–Whitney U-test. Data are presented as median (interquartile range, IQR). Results with p-values less than 0.05 were considered statistically significant. Data were analyzed using SPSS version 20 software (SPSS, Chicago, IL, USA).
Results
Of the 20 animals entering the study, three died (2 pigs in the melatonin group and 1 pig in the placebo group) due to irreversible ventricular fibrillation during the balloon occlusion. Thus, 8 pigs randomized to melatonin and 9 pigs randomized to placebo completed the experimental protocol and were included in the final analysis.
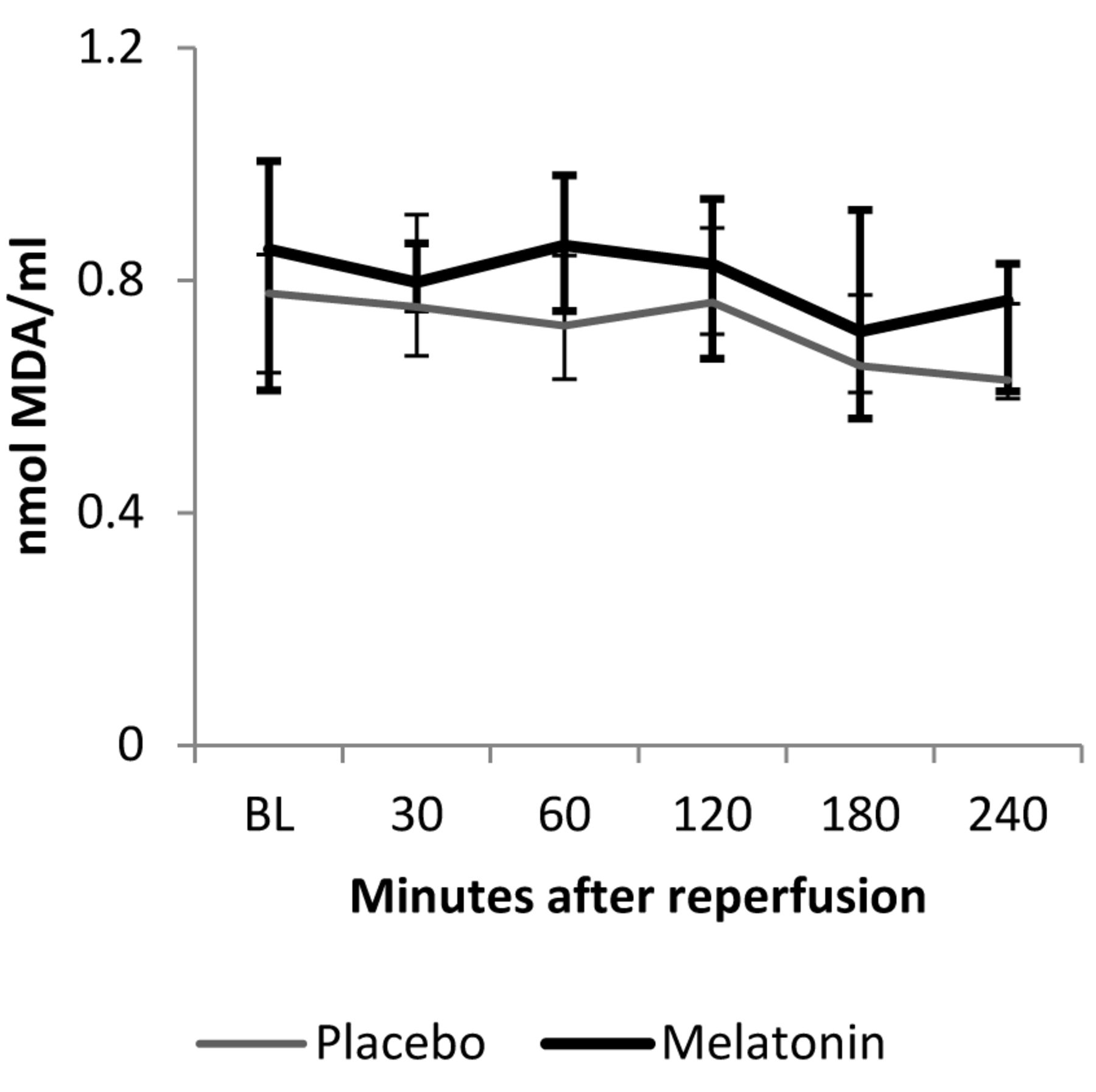
MDA measured in plasma at baseline and up to 4 h of reperfusion of the pigs receiving melatonin or placebo. Curve chart with median (lines) and interquartile ranges, IQR (bars). Thick error bars represent IQR of the melatonin data. BL=Baseline.
A total of 15 pigs had an occlusion of the circumflex artery, while 2 pigs had an occlusion of the left anterior descending artery. Three pigs in the melatonin group and 4 pigs in the placebo group experienced ventricular tachycardia. In the placebo group 1 pig was defibrillated due to ventricular fibrillation. No significant difference was observed between the melatonin group and the placebo group with respect to duration of anesthesia [melatonin: 382 (351-445) min vs. placebo: 375 (364-426) min, p=0.96] or duration of the reperfusion period [melatonin: 4 (4-4) h vs. placebo: 4 (4-4) h, p=1.00].
hs-TnT in blood samples. Baseline hs-TnT levels were 0 (0-13) ng/l in both the placebo and melatonin group. In both treatment arms, we found the highest increase in hs-TnT 2 h after the start of reperfusion, representing a myocardial infarction: 5,881 (1398-9158) ng/l in the placebo group versus 3,413 (2389-6326) ng/l in the melatonin group (p=0.63).
Oxidative stress marker in blood samples. There was no significant difference in development of MDA levels over time in the melatonin group or the placebo group (p=0.06 and p=0.23, respectively) (Figure 1). There was no significant difference in MDA levels between the melatonin and the placebo group at 4 h of reperfusion (p=0.6) (Figure 1).
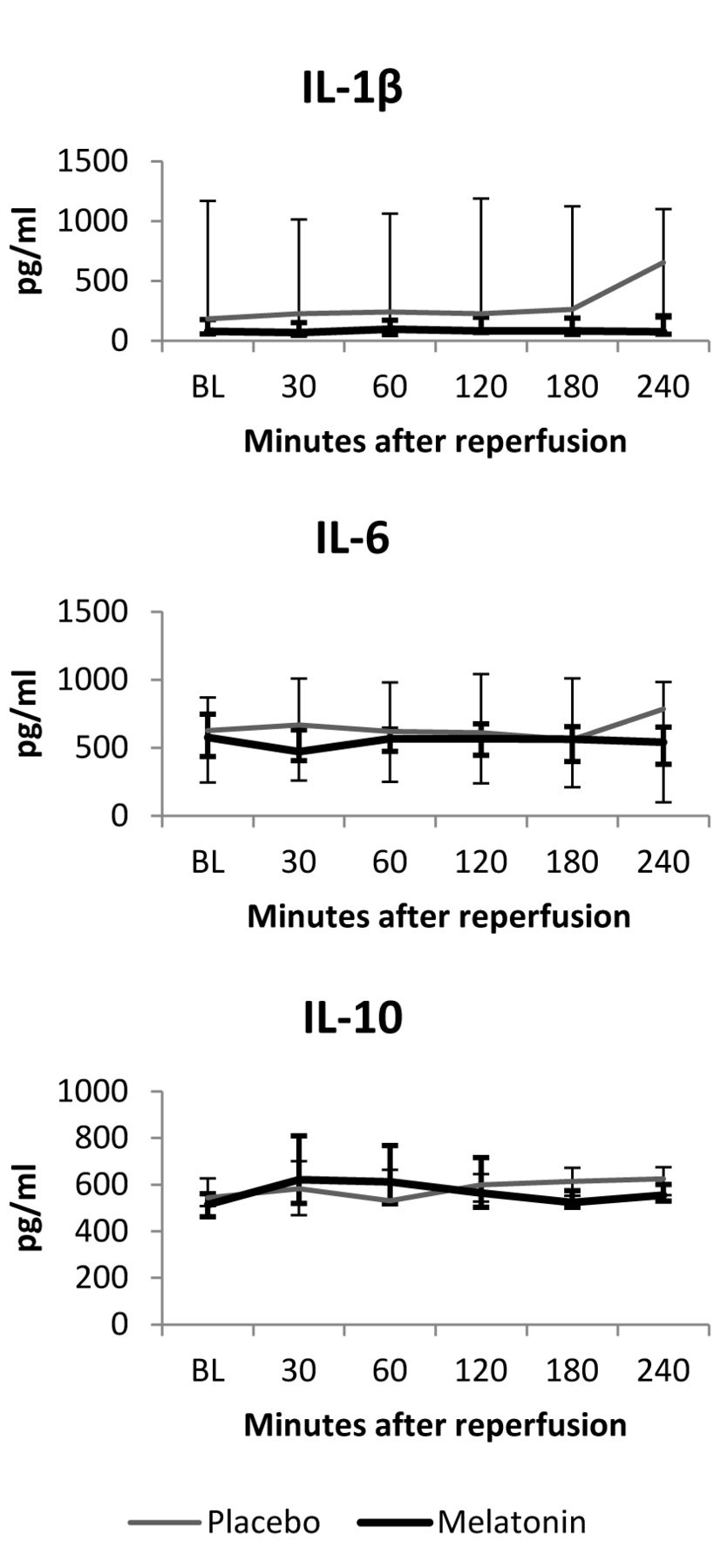
Inflammatory markers in blood samples. When analyzing IL1β, Il6 and IL10 we found no significant difference in development of levels over time in neither the melatonin (p=0.25, 0.08 and 0.08, respectively), nor the placebo group (p=0.11, 0.13 and 0.14, respectively) (Figure 2).
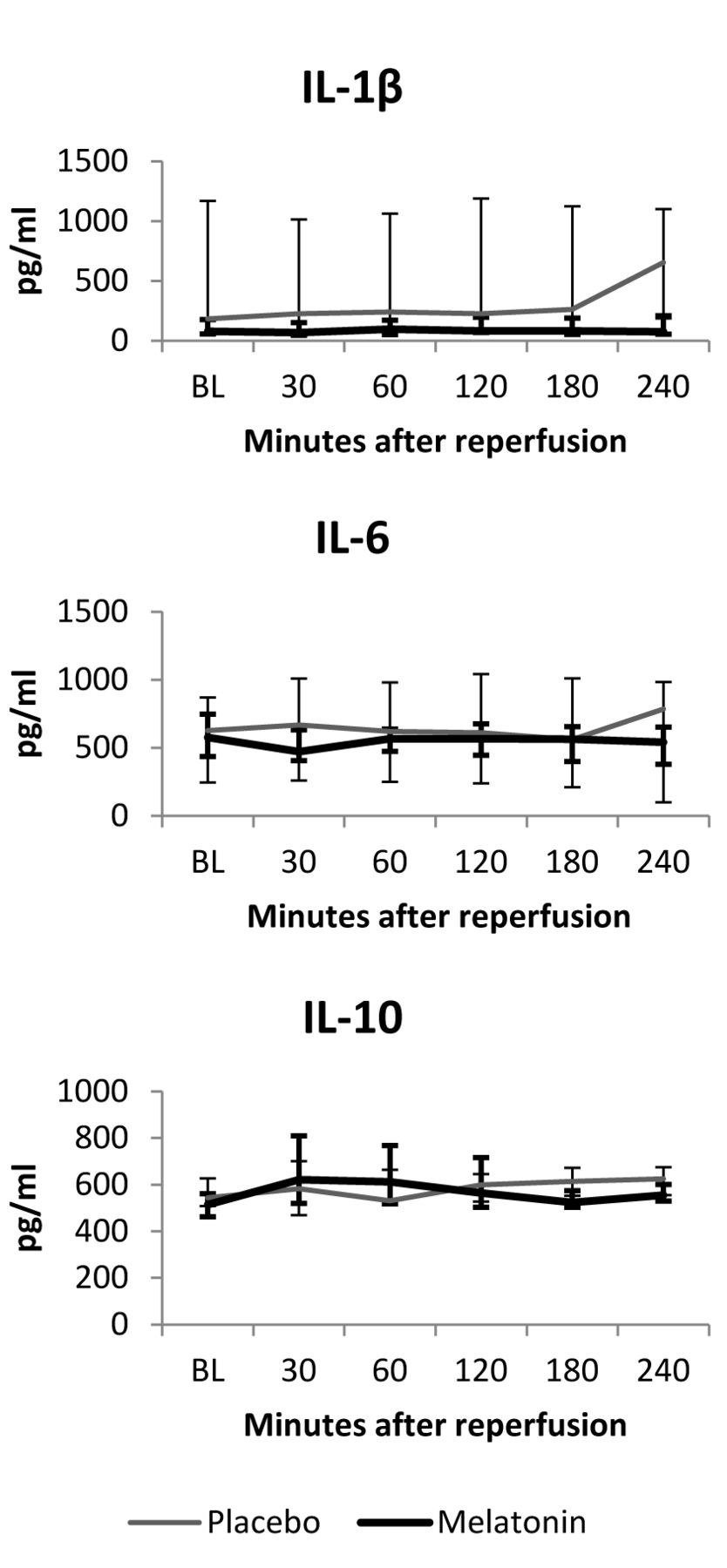
Cytokines measured in plasma at baseline and up to 4 h of reperfusion of the pigs receiving melatonin or placebo. Curve chart with median (lines) and interquartile ranges, IQR, (bars). Thick error bars represent IQR of the melatonin data. IL-1β=Interleukin-1β, IL-6=Interleukin-6, IL-10=Interleukin-10.
There was no significant difference in any of the pro-(IL1β, IL6) or anti-inflammatory (IL10) markers between the melatonin and the placebo group at four hours of reperfusion (p=1.0, 0.39 and 0.35, respectively) (Figure 2).
Discussion
In the present study, we aimed to analyze circulating levels of oxidative and inflammatory biomarkers after myocardial ischemia and subsequent reperfusion, and examine whether melatonin could reduce the production of these markers in a porcine closed-chest model. However, in our setup, 45 min of myocardial ischemia did not appear to produce a reperfusion injury that could be measured by a broad range of oxidative and inflammatory markers up to 4 h after the start of the reperfusion. Consequently, it was not possible to demonstrate whether melatonin reduced the systemic inflammatory and oxidative stress response following a coronary artery occlusion.
The closed-chest porcine model has proven to be superior in interventional studies of IR injury (11), because of the anatomical, physiological and pathological similarities to the human heart (12). Myocardial IR injury involves a number of pathophysiological mechanisms such as endothelial dysfunction, intracellular calcium overload, dissipation of mitochondrial membrane potential and immune activation (13). Furthermore, a pivotal mechanism in myocardial IR injury is the generation of oxygen metabolites, in particular reactive oxygen species, which can lead to DNA damage, lipid peroxidation, protein oxidation and mitochondrial permeability transition (14, 15). The imbalance between ROS production and antioxidant defenses leads to the condition known as oxidative stress (16). ROS and lipid peroxides are short-lived and difficult to measure directly. Thus MDA, a degradation product of lipid peroxides, is often used as a surrogate reflecting the lipid peroxidation level, as it is more stable and has a longer half-life (17). The level of MDA has been shown to increase along with cardiac necrosis markers c-troponin I and creatine kinase (18), and has also been found to be significantly higher in patients with acute myocardial infarction (AMI) compared to controls (19).
In an open-chest porcine model, 30 min of ischemia and 3 h of reperfusion were enough to produce a significant increased MDA response in myocardial tissue of pigs subjected to IR, compared to sham-operated pigs (20). Another open-chest model showed that 60 min of ischemia and 3 h of reperfusion could produce a significant increase in plasma MDA levels measured immediately after the reperfusion period compared to pigs treated with sodium nitrite (10). The influence of the surgical stress produced in these open-chest studies as compared to closed-chest studies might have increased the ROS production, which could be reflected in elevated lipid peroxidation. However, in one of the studies (10), the starting MDA level after insertion of the central venous line and arterial cathetererization was 2.7 nmol/ml, which is much higher than the levels we measured. This might be due to the spectrophotometric determination of MDA, which has been shown to result in artificially elevated MDA levels (21). Human studies measuring MDA following AMI have shown a significant increase in MDA levels in patients with AMI compared to controls, measured 6 h from the onset of symptoms (22).
With regard to inflammatory markers, it is known that activation of innate immunity also contributes to tissue damage, thereby determining the infarct size (3, 13), and elevated levels of the pro-inflammatory cytokine IL6 have proven to be an independent risk factor of increased mortality in patients with acute coronary syndrome (23), predictive of recurrent vascular instability and associated with in-hospital adverse prognosis (24), and related to death in patients with acute coronary syndrome (25). A significant elevation of the anti-inflammatory cytokine IL10 accompanies the peripheral immune responses of AMI (26), and IL10 is considered an independent predictor of long-term adverse cardiovascular outcomes in patients with acute coronary syndrome (27). There are, however, no closed-chest porcine models examining the cytokine response following myocardial IR.
With our setup, we were unable to produce an oxidative stress response or an inflammatory response that could be measured in the systemic circulation with the chosen biomarkers. This could be due to several reasons regarding both the duration of the ischemic and the reperfusion periods, and administration of the intervention.
The ischemic period of 45 min was in accordance with previous studies with regard to infarct size (28, 29). However, the present study focused only on biomarkers in the systemic circulation, thus an explanation might be that we did not include enough animals (type II error). However, the post-hoc sample-size calculation revealed we had included enough animals to test the secondary outcomes. However, most patients present with longer periods of ischemia, ranging from 3 to 12 h, hence it could be relevant to subject the animal model to a longer period of ischemia (30). Thus, the short ischemic period could be a reason why we did not see a systemic response.
Another reason might be that in our setup, acute coronary occlusion is mechanically induced in healthy coronary arteries. AMI is an acute inflammatory condition and in most patients with this condition, acute coronary occlusion is due to thrombus formation at a site of a ruptured coronary atherosclerotic plaque (30). Furthermore, it has been shown in both humans and animals that aging might augment ROS formation after myocardial IR (31).
With regard to the reperfusion period, this may have been too short in order to obtain a systemic response. In myocardial tissue, MDA has been found up to 14 days after the start of reperfusion (32). However, elevated MDA levels have also been found in pigs 2 to 3 h after the start of reperfusion (10). These MDA levels were reported in an open-chest porcine model, thus the response might have been augmented by the surgical stress owing to this method. In our set-up, it is possible that we did not see a response in the inflammatory response due to the short reperfusion period. For both IL1β and IL6, there seemed to be an increase in the placebo group at 4 h of reperfusion (Figure 2). Although this was not significantly different from that of the melatonin group, it might be indicative of an incipient increase in the systemic inflammatory response.
With respect to the intervention, we administered the melatonin intra-coronarily at the time of reperfusion, thereby ensuring a high concentration in the myocardium at risk and allowing melatonin to work at the site of the injury. Administration prior to ischemia might have yielded a better outcome for the melatonin-treated group (33), but although this is feasible in a closed-chest porcine model, it would be too far from imitating a clinically relevant situation as it is not possible to predict the time of occurrence of myocardial infarctions in humans.
In conclusion, melatonin treatment did not result in a difference in the markers of inflammatory and oxidative stress, nor in the markers of myocardial damage compared with placebo.
Acknowledgements
A special thanks is due to the Laboratory of Biomedical Science and the staff at the Laboratory of Cardiology, Aalborg University Hospital, Denmark.
Footnotes
-
This article is freely accessible online.
-
Funding statement
This work was supported by grants from the University of Copenhagen, the Lundbeck Foundation, the Aase and Ejnar Danielsens Foundation, the A.P. Møller Foundation for the Advancement of Medical Science, the Axel Muusfeldts Foundation, the Arvid Nilssons Foundation and the Snedkermester Sophus Jacobsens Foundation.
- Received March 5, 2014.
- Revision received May 14, 2014.
- Accepted April 16, 2014.
- Copyright © 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.