


Abstract
Background: Previous studies have shown antiviral, antibacterial, and anti-inflammatory activity of alkaline extract of the leaves of Sasa senanensis Rehder (SE). Here, we investigated whether SE is effective on oral lichenoid dysplasia and osteoclastogenesis. Materials and Methods: A male patient with white lacy streaks in the oral mucosa was orally administered SE three times a day for 11 months. The area of white streaks was monitored by intraoral photography. Interleukin-6 and -8 in the saliva were determined by enzyme-linked immunosorbent assay. Osteoclastogenesis of mouse macrophage-like RAW264.7 cells, induced by receptor activator of nuclear factor-κB ligand (RANKL) was monitored by tartrate-resistant acid phosphatase (TRAP)-positive multinuclear cell formation. Results: Long-term treatment with SE progressively reduced both the area of white steaks and the levels of salivary interleukin-6 and -8. SE significantly inhibited the macrophage differentiation towards osteoclasts. Conclusion: The present study suggests the therapeutic potential of SE towards oral diseases.
Over the counter (OTC) drugs in Japan are classified into three groups (I, II and III), based on their safety. Group I drugs have the highest risk of the adverse effects on our health. The intensity of safety increases in the order of group I<II<III. Alkaline extract of the leaves of Sasa senanensis Rehder (SE) (SASA-Health®), which belongs to group III of OTC drugs (1), is expected to be less hazardous, as compared with Kampo Medicines, which belong to group II. SE is recognized as being effective in treating fatigue, low appetite, halitosis, body odor and stomatitis, but there is no scientific evidence to demonstrate these phenomena, due to lack of appropriate biomarkers. SE has exhibited in vitro antiseptic (2), membrane-stabilizing (3), anti-inflammatory (4-6), antibacterial (7, 8), antiviral (7, 8), anti-UV (9, 10) and radical-scavenging (5, 8, 11) activities, and synergistic action with vitamin C (7). SE also exerts several common biological properties with lignin–carbohydrate complex (LCC): the prominent anti-HIV, anti-UV and synergistic activity with vitamin C (12), as expected from the use of alkaline solution for the extraction of both SE and LCC. We have recently identified substances responsible for the anti-UV activity of SE as being, p-coumaric acid derivative(s), lignin precursor (Matsuta et al., unpublished data). Both SE and LCC demonstrated prominent antiviral activity, one or two orders higher than that of tannins and flavonoids (7, 8, 13), suggesting their possible application for the treatment of virally-induced oral diseases. We have recently shown that an oral intake of LCC–vitamin C tablet significantly improved the symptoms of patients infected with herpes simplex virus (14, 15).
Lichen planus is a chronic mucocutaneous disease that affects the skin, tongue and oral mucosa. The most common presentation of oral lichen planus is the reticular form that manifests as white lacy streaks on the mucosa (known as Wickham's striae) or as smaller papules (small raised areas). The cause of lichen planus is not known. Some lichen planus-type rashes occur as allergic reactions to medications and complications with chronic hepatitis C virus infection (lichenoid reaction of graft-versus-host disease) (16). Hepatitis C virus has been reported to occasionally replicate in oral lichen tissue and contribute to mucosal damage (17, 18). It has been reported that the Epstein-Barr virus is more frequently detected in oral lesions such as oral lichen planus and oral squamous cell carcinoma in comparison to healthy oral epithelium (19). In the present study, we investigated whether oral intake of SE improves the symptoms of oral lichenoid dysplasia, by measuring the area of white lacy streaks and salivary interleukin-6 (IL-6) and IL-8. Activated macrophages are known to release various pro-inflammatory cytokines (20, 21). Mouse macrophage-like cell line RAW264.7 has been utilized for the study of signal transduction after stimulation with lipopolysaccharide (LPS) or the receptor activator of nuclear factor-κB ligand (RANKL) (22). We have previously shown that SE inhibited nitric oxide and prostaglandin E2 production by LPS-stimulated RAW264.7 cells (5). In the current study, we also investigated whether SE inhibits the RANKL-induced differentiation of RAW264.7 cells towards osteoclasts.
Materials and Methods
Materials. SE was prepared and supplied by Daiwa Biological Research Institute Co., Ltd., Kawasaki, Kanagawa, Japan. Lyophilization and measurement of the dry weight of SE showed that it contained 66 mg of solid materials/ml.
Treatment of a lichenoid dysplasia patient with SE. A biopsy was taken from a 43-year-old male patient, and diagnosed as lichenoid dysplasia in July 7, 2003 (physician in charge: Dr. K. Mori, Division of Oral Maxillofacial Surgery, Meikai University School of Dentistry). Treatment with vitamin B1 improved the patient's symptoms, but discontinuation of the treatment resulted in the disease recurrence. The patient was subjected to the SE treatment for 11 months (April 12, 2011 until March 12, 2012), according to the guideline of Intramural Ethic Committee (no. A0901). The patient was orally administered 13.3 ml SE (diluted two-fold with water, thus containing 33 mg dried materials/ml) three times-a-day, 30 min before each meal. At each administration, the patient swallowed and retained SE in the oral cavity for 1 min before washing it down. The patient did not take any other medications during the treatment period. The patient's oral cavity was photographed with a digital camera (EOS. 30D; Canon, Tokyo, Japan) and the total saliva was collected just before lunch on days 1, 3, 7, 14, 21, 28, and then every two weeks, after the start of SE administration. The saliva was centrifuged at 10,000 ×g and the supernatant was stored at −30°C until assay for IL-6 and IL-8.
Assay for IL-6 and IL-8 production. The IL-6 and IL-8 in the saliva supernatant were determined by ELISA, according to the manufacturer's instructions (Quantikine ELISA kit, R&D systems, Minneapolis, MN, USA).
Assay for osteoclast differentiation. RAW264.7 cells (5×104 cells/ml) (purchased from Dainippon Sumitomo Pharma, Osaka, Japan) were cultured in a 96-well plate (0.1 ml/well) with α-Modified Eagle's Minimum Essential Medium (α-MEM) (Wako Pure Chemicals. Osaka, Japan) containing 10% fetal bovine serum (FBS), in the presence or absence of RANKL (10 ng/ml R&D Systems), with or without SE. After three days in culture, tartrate-resistant acid phosphatase (TRAP) staining of the cells was performed as described previously (13). Briefly, cultured cells were fixed with 100% methanol for 1 min at room temperature and air dried. After TRAP staining using leucocyte acid phosphatase staining kit (Sigma Chem Co., St Louis, MO, USA), according to the manufacturer's instructions, TRAP-positive multinucleated (more than three nuclei) cells were photographed and counted under phase-contrast microscopy (23, 24).
Statistical treatment. Experimental values are expressed as the mean±standard deviation (SD). Statistical analysis was performed by using the Student's t-test. A p-value <0.05 was considered to be significant.
Results
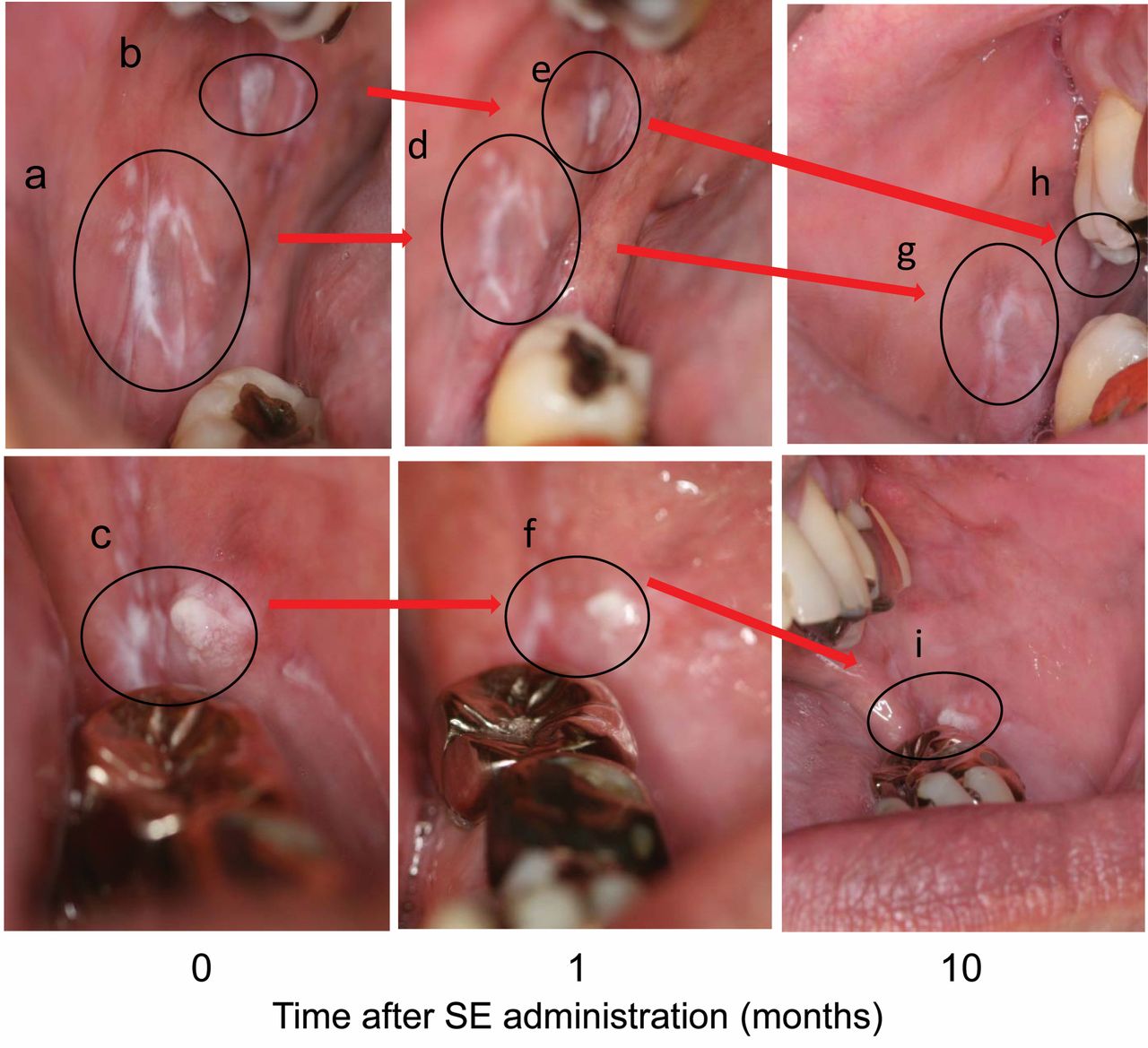
Visual inspection and patient's symptoms. Oral inspection of the patient's buccal mucosa revealed the presence of several areas of white lacy streaks, characteristic of oral lichenoid dysplasia, before SE treatment (Figure 1). The 10-month-long SE treatment cycle (swallowing, retaining and washing down) progressively reduced the area of the white streaks (Figure 1). This was accompanied by the improvement of the patient's symptoms. Before the SE treatment, the patient felt that the mucosa was uneven, rough and cut by touching with his tongue. Three weeks after the treatment, such feelings subsided and the mucosa became much smoother. At four weeks, the rough mucosa was narrowed into a smaller area, and the patient could eat without any pungent feeling on the oral mucosa. Oral intake of SE also improved the patient's symptoms of pollen allergy, and loose teeth, giving an impression that the oral mucosa became much tighter.
Changes in salivary anti-inflammatory cytokines. Before the SE treatment (April 1, 4, 5, 6 and 7, 2011), the salivary concentration of IL-6 was approximately 0.052±0.030 ng/ml (n=5). After the intake of SE, the IL-6 level decreased to 0.01 ng/ml (April 27, 2011, at three weeks after the start of treatment), acutely increased to 0.34 ng/ml (May 6, 2012, at four weeks) due to opportunistic infection, and then again decreased to a baseline level of 0.016±0.009 ng/ml (n=15) (approximately 31% of initial) after June 15, 2011, nine weeks after the start of SE treatment) (Figure 2A).
SE treatment induced a more stable decline in the salivary IL-8 concentration (Figure 2B). Before the SE treatment, the salivary concentration of IL-8 was approximately 5.25±1.06 ng/ml (n=5), two orders higher than that of IL-6. After the intake of SE, the level of IL-8 decreased to 1.11 ng/ml (April 27, 2011, at three weeks of therapy), acutely elevated to 5.35 ng/ml (May 6, 2011, at four weeks) and decreased again to a baseline level (1.49±0.66 ng/ml, n=16) (approximately 28% of the initial measurement) (June 15, 2011, at nine weeks) (Figure 2B). It should be noted that the salivary IL-8 concentration after SE treatment was below the initial level throughout the experimental period.

Time-dependent effect of alkaline extract of the leaves of Sasa senanensis Rehder (SE) on the oral lichenoid dysplasia. One 51-year-old male patient with lichenoid dysplasia was treated for 10 months with 13.3 ml of 50% diluted SE (containing 33 mg dried material/ml) at each meal, three times a day. Intraoral photographs of the right side (upper panel) and left side (lower panel) of buccal mucosa were taken. It should be noted that the SE treatment progressively reduced the area of the white streaks (a → d → g, b → e → h in the right side of buccal mucosa and c → f → i in the left side of buccal mucosa).
Inhibition of osteoclastogenesis. RAW264.7 cells were differentiated by RANKL treatment towards TRAP-positive cells, and then fused to become multinuclear osteoclasts (25). SE inhibited the RANKL-induced TRAP-positive osteoclast formation and completely inhibited multinuclear cell formation (Figure 3, left). The inhibitory effect of SE was detected at 1% SE by inhibition of mononuclear osteoclast formation, and 2.5% SE completely inhibited osteoclastogenesis (Figure 3, right).
Discussion
Currently there is no cure for lichen planus but there are certain types of medicines used to reduce the effects of the inflammation. Lichen planus may go into a dormant state after treatment, and can flare up years after it is considered cured. Medicines used to treat oral lichen planus include steroids, retinoids, immunosuppressant medications, hydroxy-chloroquine, tacrolimus, dapsone, UVB narrow-band phototherapy (26), aloe vera (27) and purslane (28). The present study demonstrated for the first time that SE potently reduced the area of white streaks of the lichenoid dysplasia, and led to significant reduction of the baseline levels of two pro-inflammatory cytokines, IL-6 and IL-8, but not to complete eradication. This result is in agreement with an in vitro study that demonstrated that SE inhibited significantly, but not completely, the production of IL-8 by IL-1-stimulated human gingival fibroblasts (6). This suggests the necessity for combinational treatment with other drugs that have different sites of action from that of SE.

Effect of alkaline extract of the leaves of Sasa senanensis Rehder (SE) on salivary inflammatory cytokine levels. A patient with lichenoid dysplasia was treated with SE, and the salivary interleukin-6 (IL-6) and IL-8 concentrations were determined by enzyme-linked immunosorbent assay (ELISA). Each value represents the mean±S.D. of triplicate assays. ○ Control, ● SE treatment.
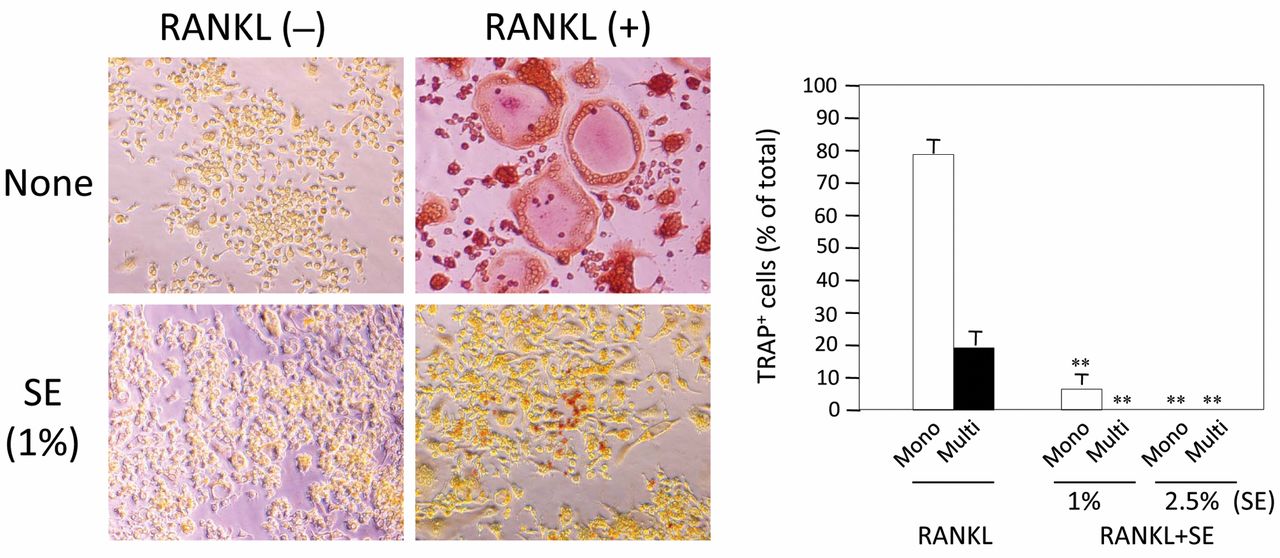
Effect of alkaline extract of the leaves of Sasa senanensis Rehder (SE) on osteoclast formation of RAW264.7 cells by receptor activator of nuclear factor-κB ligand (RANKL) stimulation. RAW264.7 cells were cultured with or without SE in the presence or absence of RANKL. After tartrate-resistant acid phosphatase (TRAP) staining, cells were photographed (left side), and TRAP-positive mono- and multinucleated osteoclasts were counted and compared with the respective controls. **p<0.01 vs. RANKL-treated mononuclear osteoclasts, or multinuclear osteoclasts of the control group, respectively.
Osteoclast is differentiated from hematopoietic cells of the monocyte/macrophage lineage. Formation of osteoclasts is stimulated not only by RANKL but also by inflammatory cytokines, such as IL-1, IL-6, and tumor necrosis factor-α (29, 30). We also found that SE inhibited the RANKL-induced osteoclastogenesis of RAW264.7 cells. Taken together with our previous study (5), SE may inhibit both the activation and the maturation of macrophages, and thus inhibit the production of macrophage-derived pro-inflammatory cytokines that are involved in the initiation and progression of oral lichen planus (31, 32). The therapeutic effect of SE may be generated through antiviral activity, inhibition of pro-inflammatory cytokine production, and immunopotentiation via binding to specific receptors (33), or any combination of these. Further study is required to elucidate the mechanism of action, and find the best partners that synergistically augment the action of SE. Many oral squamous cell carcinomas develop from pre-malignant conditions of the oral cavity. A wide array of conditions have been implicated in the development of oral cancer, including lichen planus, as well as leukoplakia, erythroplakia, palatal lesion of reverse cigar smoking, oral submucous fibrosis, discoid lupus erythematosus, and hereditary disorder such as dyskeratosis, congenital and epidermolysis bullosa (34). The inhibitory action of SE towards lichenoid dysplasia may also inhibit the development of oral cancer.
The present pilot study, based on only a single patient with lichenoid dysplasia, provided the following evidence: (i) oral administration of SE exerts a therapeutic effect on lichenoid dysplasia, (ii) the therapeutic effect of SE is detectable three weeks after the start of SE treatment, and (iii) salivary IL-8 level is a stable biomarker of lichenoid dysplasia. Further study with greater numbers of patients is under way.
- Received June 26, 2012.
- Revision received August 7, 2012.
- Accepted August 8, 2012.
- Copyright © 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Synergism of Alkaline Extract of the Leaves of Sasa senanensis Rehder and Antiviral Agents
- Prominent Anti-UV Activity and Possible Cosmetic Potential of Lignin-carbohydrate Complex
- Anti-Halitosis Effect of Toothpaste Supplemented with Alkaline Extract of the Leaves of Sasa senanensis Rehder
- Efficient Utilization of Licorice Root by Alkaline Extraction
- Biological Interaction between Sasa senanensis Rehder Leaf Extract and Toothpaste Ingredients