


Abstract
Background: Melanoma has the highest rate of spread to the leptomeninges and the incidence of melanoma has been steadily rising. This article describes recent experience at the Lille University Hospital, between 2007 and 2011 and discusses the possibilities for treatment of leptomeningeal metastasis. Patients and Methods: Nine patients were diagnosed with leptomeningeal metastasis of melanoma. The standard criteria were used for the diagnosis. The treatment consisted of a combination of intrathecal chemotherapy, systemic chemotherapy and best supportive care. Results: The overall median survival from the time of leptomeningeal metastasis diagnosis was eight weeks (range=1-168 weeks). In two cases, the median overall survival was 104 weeks. For these patients, there was a clear benefit in intrathecal chemotherapy combined with systemic treatment. No complication was observed. Conclusion: Despite a poor prognosis, treatment of melanoma leptomeningeal metastasis is needed in order to improve the quality of life, neurological progression-free survival and overall survival of patients.
In Europe, melanoma represents a growing public health concern, the incidence of melanoma has been steadily rising, including France. Between 1980 and 2000, the standardized world population incidence rate of melanoma increased from 2.4 to 7.6 per 100,000 inhabitants/year (1). Leptomeningeal metastasis (LM) is the result of the seeding of the leptomeninges and cerebrospinal fluid (CSF) by malignant cells. Symptomatic LM may affect 5% of all patients with solid malignant tumors. Meningeal diffusion of melanoma can be found in 20% of patients in clinical studies, and up to 44-70% in autopsie series of patients with central nervous system (CNS) metastatic diseases (2). Despite its incidence, LM from melanoma is rarely diagnosed and studied in the literature (2-18).
Establishing a diagnosis of LM in a patient with melanoma can be difficult. The prognosis is very poor with progressive neurological signs and symptoms leading to death, sometimes in a few days or weeks. For these reasons it is necessary to achieve faster specific additional tests such as entire-neuraxis magnetic resonance imaging (MRI) and lumbar puncture for CSF. MRI with gadolinium enhancement (MRI-Gd) is the technique of choice to evaluate patients with suspected LM, but normal findings do not exclude the diagnosis and no MRI-specific criteria are defined for diagnosis or follow-up (19). Cytological analysis of the CSF is currently considered the gold standard for the diagnosis of LM. The specificity of this analysis is high (>95%), but the sensitivity remains insufficient (<50%). Small CSF volumes (<10.5 ml) obtained and delayed processing of specimens may lead to inaccurate negative-cytology (20). It may be necessary to repeat the lumbar puncture to detect potential malignant cells if the first puncture result is negative. The low sensitivity of CSF cytology makes it difficult not only to diagnose LM but also to assess the response-to-treatment (21, 22). Treatment consists of a combination of intrathecal and systemic therapy. Commonly used agents in intrathecal chemotherapy are methotrexate, liposomal cytarabine (depocyt) and thiotepa. The treatment is intended to stabilize or improve the neurological status, maintain neurological quality of life and prolong survival. Established neurological defects are rarely improved with treatment, but the progression of neurological deterioration may be halted in some patients (23). Only a few cohorts of melanoma LM have been reported, the median overall survival was 10 weeks in the largest cohort (9).
Patients' characteristics at the time of melanoma diagnosis.
We here report our experience with nine consecutive patients, prospectively followed-up at our Center of Lille between 2007 and 2011, and discuss the different means of diagnosis of melanoma LM and systemic and intrathecal treatment.
Patients and Methods
All consecutive patients diagnosed with melanoma LM between January 2007 and March 2011, were prospectively followed-up at the Lille University Hospital. Only patients who did not have any other prior cancer were considered for enrolment into this study. The standard criteria for LM were used for the diagnosis: presence of tumor cells on the cytological study of CSF and/or presence of typical MRI signs of LM in patients with typical neurological symptoms. All the patients received a combination of intrathecal and systemic chemotherapy. Intrathecal chemotherapy was administered via either lumbar puncture or ventricular device. Standard liposomal cytarabine regimen was used at first (50 mg once every two weeks for two months and then 50 mg every four weeks until progression). A second line of intrathecal chemotherapy with standard thiotetraethylenepentamine (thiotepa) regimen (10 mg twice a week for four weeks, 10 mg once a week for four weeks and then once a month until progression) was administered, in cases of LM progression in patients with a preserved performance status (PS). Systemic treatment was selected by the referent oncologist of the patient. The patients were regularly followed up with clinical, CSF and MRI evaluations until their death. Our goal was to describe demographic, histopathologic and survival data.
Results
Nine patients (5 women) with melanoma LM were diagnosed and treated at the Lille Univsersity Hospital. Seven patients presented with a cutaneous primary lesion and two with melanoma of unknown primary site. The Breslow depth of the primary melanoma was <2 mm for three patients (0.62 mm, 0.95 mm and 0.98 mm) and between 2 mm and 10 mm for three patients (2.05 mm, 3.5 mm and 8 mm). One patient presented with three melanomas (0.48 mm, 2 mm and 2.1 mm). Details on patients' demographics and characteristics of the primary melanoma are listed in Table I. No particular risk factor for LM was indicated upon analysis. The median age at LM diagnosis was 44 years (range=31 to 55 years). The median time between diagnosis of primary melanoma and LM was 227 weeks (range=0-580 weeks). The median time between first metastases and diagnosis of LM was 58 weeks (range=0-265 weeks). At the time of LM diagnosis, eight patients had systemic metastases of their melanoma (liver metastases: 5/9 patients, bone metastases: 4/9 patients, pulmonary metastases: 3/9 patients, brain parenchymal metastases: 3/9 patients). LM and brain metastases were the first manifestations of primary melanoma in only one patient. The median time between the first symptoms and diagnosis of LM was two weeks (range=0-9 weeks). At LM diagnosis, patients presented with pleomorphic symptoms and signs (headache, diplopia, lower and upper limb weakness), five patients presented with a PS ≤2 and four patients with a PS of 3 (Table II). Malignant cells were detected in CSF cytological analysis for 8 patients (Figure 1). Tumor cells were all detected at the first lumbar puncture, in a median volume of 8.5 ml of CSF. The median CSF proteinorachia was 1.14 g/l (0.22 g/l to 11.16 g/l) and the median CSF glycorachia was 2.45 mmol/l (1.2 mmol/l to 4.6 mmol/l). The cerebrospinal MRI findings favored the diagnosis of meningitis in seven patients (Figure 2) (hydrocephalia, n=1; leptomeningeal contrast enhancement associated or not with meningeal nodules, n=6) and of intraparenchymal metastasis in three patients (Table III). All patients received intrathecal liposomal cytarabine (depocyt); the number of intrathecal administrations varied from 1 to 27 (median=3). Three patients received a second line of intrathecal chemotherapy of thiotepa (1, 7 and 18 injections) and one patient received a third line by intrathecal methotrexate (four biweekly injections). The first intrathecal injection was administered after a median delay of six days after LM diagnosis. A ventricular device was implanted in two patients, 4 weeks and 12 weeks after LM diagnosis respectively when the patient's general condition was stable. No complication of catheter or intrathecal chemotherapy was observed during the patients' follow-up, corresponding to 45 intraventricular injections. Systemic chemotherapy consisted of temozolomide (n=3), fotemustine (n=5) or carboplatin (n=1). The median overall survival from LM diagnosis was eight weeks (range=1-168 weeks). At the time of writing, the nine patients had died. Treatment probably had only little influence on disease progression in the seven cases with a median overall survival inferior to seven weeks (range=1-17 weeks).
Patients' characteristics at the time of leptomeningeal metastasis (LM).
In two cases, the neurological progression-free survival and the median overall survival were improved by the combined treatment (150 and 168 weeks in patient 1; 10 and 60 weeks in patient 2). The first patient had a primary melanoma 3.5 mm Breslow depth of the trunk in 2001, treated with surgical treatment. In April 2006, brain, lung, hepatic, cutaneous and lymph node metastases were discovered and treated with fotemustine chemotherapy (nine injections) until stabilization in January 2007. In March 2007, the patient presented with progressive diplopia, bilateral facial palsy and motor disorders. Initial PS at diagnosis, was 2. Cerebrospinal MRI did not reveal any CNS metastases. The diagnosis of LM was assessed by CSF cytological analysis, nine weeks after the first symptoms. Intrathecal liposomal cytarabine was started in May 2007 until April 2009 (27 injections) and was associated with systemic chemotherapy (four injections of fotemustine) from May to October 2007. This treatment resulted in slight clinical improvement and disappearance of malignant cells in the CSF; it was discontinued due to stabilization of the disease. The patient did not present with new melanoma metastases but suffered from evolving decubitus complications. He died in September 2010, 42 months after LM diagnosis. The second patient presented with a right frontal expansive process with a major mass effect on the brain parenchyma, in August 2008. He suffered from headache, nausea, vomiting and lower and upper right limb weakness. Initial PS was 1 at LM diagnosis. The treatment consisted of neurosurgery, whole-brain radiotherapy and adjuvant fotemustine chemotherapy. The histological analysis was in favor of nodular LM. The CSF analysis did not reveal malignant cells. In March 2009, he presented with a new right parasagittal metastasis next to the vertex, a right frontal nodule on the MRI, and malignant cells were found in CSF. A combined treatment with intrathecal chemotherapy liposomal cytarabine (four injections) and systemic fotemustine was performed. A ventricular device was implanted in April 2009. In May 2009, after four injections of liposomal cytarabine, the patient presented with changed mental status and focal seizures. MRI did not show any radiological progression and the CSF showed no tumor cells. No other intercurrent disease could explain the clinical neurological deterioration. The intrathecal chemotherapy was changed to thiotepa. There was a rapid clinical improvement, and the patient was able to carry out normal daily activities. In October 2009, due to chemotherapy-induced thrombocytopenia and stabilized general condition, systemic chemotherapy with fotemustine was replaced by temozolomide. In December 2009, after 18 intrathecal injections, the patient presented with drowsiness, altered mental status, paranoid delusion, weight loss and asthenia. A progression was observed on MRI, and tumor cells were found in the CSF study. Intrathecal thiotepa was changed to intrathecal methotrexate, but after four bi-weekly injections of methotrexate, there was no significant clinical improvement. Therefore, it was decided systemic and intrathecal chemotherapy for to be stopped in December 2009. Best supportive care was implemented. The patient died in August 2010.
Cytological and radiological characteristics at diagnosis of leptomeningeal metastasis.
Metastatic malignant cells in cerebrospinal fluid. Original magnification ×400: mitotic phase (arrows for example) and visible melanin granules.

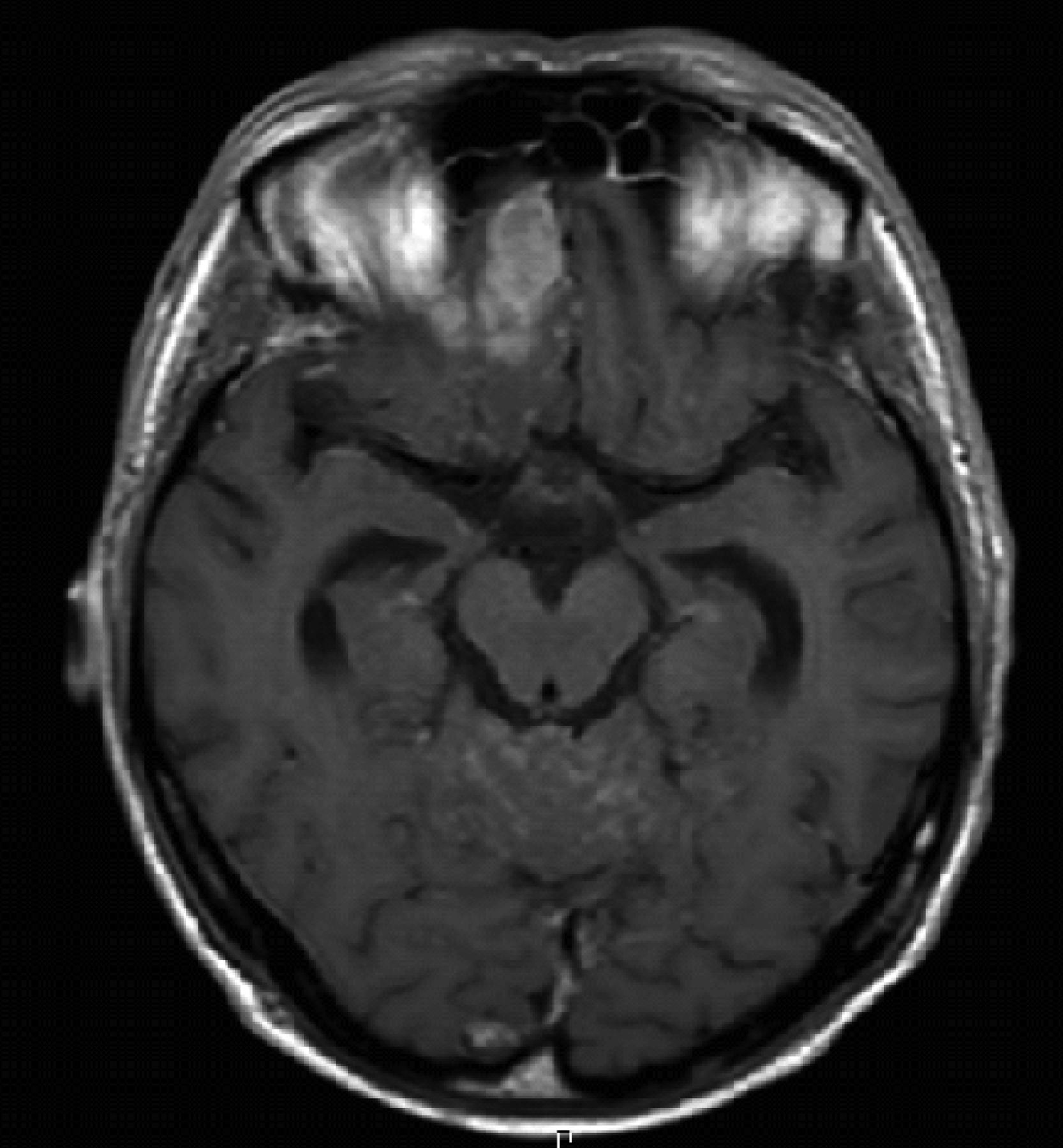
Cerebrospinal magnetic resonance imaging: axial T1 with gadolinium sequence: cerebellar meningeal contrast enhancement and right frontal expansive process.
Discussion
LM is a very devastating complication of melanoma with a somber functional and vital prognosis. LM melanoma is most probably underdiagnosed (2). Amer et al. (24) and Moseley et al. (2) reported two series of patients with disseminated malignant melanoma: meningeal involvement was clinically suspected in respectively 10.6% and 20% of the patients and confirmed in 52% and 44-70% of autopsie series, respectively. The diagnosis of LM is probably often underestimated because of the pleomorphic signs and symptoms of LM, the lack of sensitive assessments and the fulminant progression of melanoma LM. Risk factors for CNS metastases among patients with cutaneous melanoma are: sex, head and neck or oral primary lesion, presence of visceral metastases (mainly lung), primary tumor thickness and ulceration of primary lesion (25). No risk factor was found in melanoma LM in our cohort or in literature. Specific assessments are needed whenever LM diagnosis is evoked. Entire-neuraxis MRI with gadolinium enhancement is the technique of choice to evaluate patients with suspected LM. But there are no MRI-validated criteria for LM diagnosis and monitoring (19, 26-29). However, 30-60% of gadolinium MRI results are false-negatives (19, 30). The most useful laboratory test to diagnose LM is the CSF cytological examination, which is negative at first lumbar puncture in fewer than 50% (20). New, more sensitive MRI criteria and biomarkers still remain to be defined. Some non-specific markers (carcinoembryonic antigen, cancer antigene 15-3, cancer antigen 125, cancer antigen 19-9) could be useful for the diagnosis of LM and the monitoring of the disease (31). It would be also interesting to evaluate lactate dehydrogenase (LDH) in melanoma LM. LDH is the serological marker most commonly used in the early detection of local recurrence or metastasis in patients with melanoma (32). Its plasma concentration seems to be an independent prognostic factor in patients with stage IV metastatic melanoma (33). Other putative tumor markers in CSF (fibronectin, beta 2-microglobulin, IgM index, and rise of IgG index, interleukin-6, and tumor necrosis factor-alpha) could provide preliminary evidence for an invasion by melanoma cells invasion of the subarachnoid space. Studies with new alternative biomarkers (vascular endothelial growth factor, stromal cell-derived factor-1) are ongoing (34). Multiple reverse transcriptase-polymerase chain reaction (RT-PCR) markers (melanoma-associated antigen 3, melanoma antigen recognized by T-cells 1, and tyrosinase) have been compared to immunohistochemistry (IHC), using anti-S100 and anti-human melanoma black-45 antibodies to detect occult metastatic melanoma cells in the CSF (34). Multimarker RT-PCR was more informative and sensitive than cytology/IHC in assessing the CSF of patients with melanoma (34). Immunomagnetic platform technology (IMPT) through expression of epithelial cell adhesion molecule or other markers to be defined, based on the primary cancer could lead to an earlier diagnosis of LM in patients with solid tumors, outperforming CSF cytology and MRI (35, 36). It is now necessary to confirm the results of these technologies in further studies. However, melanoma LM displays a particularly fulminant course, with a mean median survival of 10 weeks after diagnosis (9), which is consistent with the median of eight weeks that we observed. Treatment probably had only a little effect on survival in seven cases. The question arises as to whether such treatment was inefficient in these seven patients or whether the unsatisfactory results were due to delayed diagnosis of a disease that evolves rapidly. Two patients had prolonged survival, of more than one year after diagnosis with treatment. Spontaneous autoimmunity may improve overall survival in patients with visceral metastatic melanoma (37). This observation may explain why two patients had a longer survival, and the delay between the last treatment and the death of patients. When LM is diagnosed, it is necessary to treat these patients quickly (37). Even if overall survival is most often short, it is important to offer some treatment in order to preserve the neurological function and maintain the quality of life of the patient. Only a few studies have been conducted on melanoma LM. In a cohort of 110 patients with LM diagnosed between 1944 and 2002, different approaches to treatment were chosen. The median overall survival was 10 weeks and 7% of the patients were still alive at one year after LM diagnosis (9). In this cohort of 110 patients, intrathecal therapy did have a positive effect on outcome in multivariate analysis (p=0.0036). Chemotherapy is the only treatment that can treat the entire neuraxis with acceptable toxicity, and may be administered systemically or intrathecally. Few data are available about the pharmacokinetics of the different chemotherapy regimens used in melanoma. Temozolomide, which is considered to be useful in melanoma metastases of CNS, had a CSF penetration of only 20% of the systemic concentration (38). There is thus an interest to combine intrathecal chemotherapy and systemic chemotherapy in LM. For our combined treatment, we did not observe any toxicity or complication. At our Center, liposomal cytarabine was chosen as first-line intrathecal therapy since it had lead to longer progression-free survival and better quality of life than methotrexate, according to results from a randomized trial (39). Liposomal cytarabine has a particularly long half-life in CSF, which leads to separately spaced administrations. Combined intrathecal interleukin-2 and systemic treatment has been evaluated in a cohort of 46 patients. Twelve responses were observed and the median overall survival was 3.8 months. The side effects seemed to be moderate and the authors concluded that interleukin-2 could be an important tool to deal with melanoma LM (38). Intraventricular interferon alpha-2 was tested in five patients with melanoma LM, but safety and rapid progression of the disease did not encourage other studies (40). All these different approaches remain unsatisfactory and treatment remains poor and ineffective. Ipilimumab, a monoclonal antibody that blocks CTLA-4, seems efficient in advanced melanoma. A phase III randomized study showed that first-line treatment with a combination of ipilimumab and the standard chemotherapy drug dacarbazine improves overall survival in patients with previously-untreated metastatic melanoma (41). The identification of somatic mutations in the gene encoding the serine–threonine protein kinase BRAF in 50% of melanoma cases offers an opportunity to test the oncogene-targeted therapy. Another randomized international phase III trial of 675 patients showed that vemurafenib, which targets the V600E mutations in the BRAF gene, was the first drug to improve overall survival when compared to standard chemotherapy in patients with advanced melanoma (42). These approaches represent an important advance in the treatment of metastatic melanoma and perhaps for the treatment of melanoma LM and CNS metastasis.
Conclusion
Improving means of LM is urgently needed. A combination of different antibodies and immune-magnetic platform technology may be interesting. Despite a poor prognosis, early treatment of melanoma LM is required in order to improve the quality of life, neurological progression-free survival and overall survival. Given the small number of patients included in our study, it is difficult to judge the effectiveness of combined intrathecal liposomal cytarabine and systemic treatment. However, its efficacy in some patients encourages us to continue assessing liposomal cytarabine in first-line treatment of melanoma LM, associated with encouraging new treatments in melanoma (ipilimumab and vemurafenib).
- Received June 16, 2012.
- Revision received August 6, 2012.
- Accepted August 8, 2012.
- Copyright © 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Proteomic Analysis of CSF from Patients with Leptomeningeal Melanoma Metastases Identifies Signatures Associated with Disease Progression and Therapeutic Resistance
- Intrathecal Administration of Tumor-Infiltrating Lymphocytes Is Well Tolerated in a Patient with Leptomeningeal Disease from Metastatic Melanoma: A Case Report