


Abstract
Hydroxyurea (HU) is an antitumor agent effective in the treatment of myeloproliferative disorders. It is usually well-tolerated and has low toxicity but its use is associated with several adverse cutaneous effects. Among them, leg ulcers have been noted in association with long-term administration. Poor response to traditional local and systemic therapy is a typical feature of HU-induced leg ulcers, and discontinuation of the drug is often required to achieve complete wound healing. We present a case of circumferential HU-induced leg ulcer in a patient affected by essential thrombocythemia, in which the lesion occured after the definitive suspension of the treatment. We propose a conservative management with a new collagenase (Bionect Start®) for skin lesions in this type of patient, for whom a surgical treatment could be more complicated, due to the underlying disease.
Hydroxyurea (HU) is an antitumor agent, a hydroxylated derivative of urea, that has been recognized since 1960 as being effective against cancer (1). It is a cytostatic agent and through inhibition of the enzyme ribonucleotide reductase, it promotes the inhibition of cellular DNA synthesis and cell death in the S phase of the cell cycle (2).
Chronic myeloid leukaemia and other myeloproliferative disorders (3, 4), such as essential thrombocythemia (5) and polycythemia vera (PV) (6) are the most common indications for HU therapy.
The cutaneous side-effects of hydroxyurea include xerosis, hyperpigmentation, nail discoloration, scaling, lichen planus-like lesions, poikiloderma and atrophy of the skin and subcutaneous tissues (7-9). Another rare and incompletely-characterized complication, described in patients with myeloproliferative-receiving high-dose long-term HU treatment, is the occurrence of painful leg ulcers (10). Leg ulcers induced by HU have common features; most of them are localized to the malleolar region, and are refractory to meticulous wound care. Poor response to traditional local and systemic therapy is a typical feature of HU-induced leg ulcers, and discontinuation of the drug is often required to achieve complete wound healing (6, 8, 11). Suspension of the drug usually improves the skin ulcer; although, in some cases, the ulcer remains and additional therapies, such as skin grafting, are needed (12).
We present a case of circumferential leg ulcer in a patient affected by essential thrombocythemia, previously treated with HU therapy, in which the lesion occurred after the definitive suspension of the treatment, probably triggered by a traumatic event. We also propose conservative management with a new collagenase (Bionect Start®) for skin lesions in this type of patient, for whom a surgical treatment could be more complicated, due to the underlying disease.
Case Report
A 74-year-old female, affected by essential thrombocythemia, presented to the Department of Plastic and Reconstructive Surgery of Policlinico Umberto I of Rome with a circumferential wound of the right leg.
The patient referred that she had been treated with HU, receiving 1 g daily of HU, for 7 years and that the treatment had been suspended for six months. During the treatment, she did not develop any cutaneous or soft tissue complications.
She reported that the lesion appeared one month after a leg trauma, caused by the hit of a soccer ball and that she had undergone other outpatient care with poor results. The skin lesion progressed to become a deeper, severely painful and hemorrhagic ulcer. The complete blood cell count revealed a hemoglobin level of 9.2 g/dl, and a platelet count of 788×103/μ/l.
At local clinical examination, the lesion was found to extend from the knee to the ankle (25×30 cm), involving the cutaneous and subcutaneous tissues. The lesion had regular margins and definite limits. The bed of the ulcer was highly fibrinous and appeared to be contaminated (Figure 1).
Before starting any treatment, a bacterial examination was performed. The treatment consisted of conservative management and antibiotic therapy, administered due to Staphyloccocus aureus and Pseudomonas aeruginosa wound contaminations.
The wound care consisted of saline solution washes, disinfection with Amukine and Betadine, application of Bionect Start® (Fidia Farmaceutici SpA, Medical Devices, Abano Terme, Italy) and occlusive dressing. Zinc oxide paste was also applied to the skin surrounding the wound. No advanced dressings that could vary healing time was used. The treatment was performed daily by the patient personally and every three days at our outpatient clinic, to examine for changes and progress.
We observed a progressive and rapid improvement of the condition, with resolution of the contamination and reduction of secretion, exudates and pain or burning during dressing. (Figure 2).
The complete re-epithelialization of the extensive loss of substance was achieved after three months, obtained with antibiotic therapy and dressing-alone without surgery (Figure 3).
Discussion
HU is an antitumor agent, which is usually well-tolerated and has low toxicity (1). Adverse cutaneous effects associated with HU have been occasionally described in the literature (8, 13). In addition, leg ulcers have been noted in association with long-term HU administration. HU-induced skin ulcers were first reported in 1985 by Stahl and Silber (10). Approximately nine percent of patients receiving HU medication develop this complication (7, 14). HU effects on actively proliferating epithelial cells have been less described (14). The pathogenesis of HU-induced ulceration may be multifactorial. The main assumptions are: interruption of the microcirculation due to leukocytoclastic vasculitis or arterial microthrombi related to platelet dysregulation (13, 15), cumulative toxicity in the basal layer of the epidermis through inhibition of DNA synthesis (8); and repeated mechanical injury in areas subject to trauma (16). Literature data reveal that most of the patients with HU-induced leg ulcer had been treated with more than 1 g of HU per day for at least one year (8).
Poor response to traditional local and systemic therapy is a typical feature of HU-induced leg ulcers, and discontinuation of the drug is often required to achieve complete wound healing (6, 8).
In the case described here, a new ulcer had developed even after 5 months from cessation of HU administration. Probably in this case, a traumatic event triggered the onset of the first event and since the direct cytotoxic effect of HU (8) may continue even after the withdrawal of the drug, the repair of the first injury may have been inhibited. Recurrence of HU-related leg injuries after discontinuation of the therapy has already been described (17), but our case is particularly interesting because the recurrence occurred many years after discontinuation of HU therapy.
Frequently, management of resistant HU-related ulcers requires surgical therapy such as skin graft. We propose a conservative management for this type of patient, for whom a surgical treatment could be more complicated, due to the underlying disease.
We proceeded with disinfection and use of Bionect Start®. Bionect Start® is a topical cream containing hyaluronic acid, bacterially-fermented sodium hyalunorate (0.2% w/w) salt and bacterial collagenase obtained from non-pathogenic Vibrio alginolyticus (>2.0 nkat/g) (18). The use of collagenase is based on its lysis of fibrin and necrotic tissue. The topical administration of collagenase increases the effect of macrophagic collagenase, which is responsible for wound debridement by splitting and breaking down proteins which hold dead and devitalised material on the wound (19). Bionect Start® provides an optimal moist enviroment and wound preparation which facilitates the natural healing process (20, 21). This drugs also contains hyaluronic acid (HA) (21), which above all generates a microenvironment stimulating the secretion of growth factors and proliferation and migration of fibroblasts, endothelial cells, keratinocytes and angiogenesis (19, 21) and has a positive effect on the inflammatory response (22-24). Moreover HA is also capable of regulating the water balance, acting on osmotic pressure and flow resistance and selectively regulating the diffusion of plasma and matrix proteins (25).
With conservative management and the use of Bionect Start®, we obtained complete resolution and re-epithelialization of the circumferential lesion in three months.
Conclusion
We suggest to HU-treated patients, that it is important to be aware of the possibility that this type of complication may occur, even years after HU treatment suspension, as did in our case. We advise such patients to avoid conditions that may lead to traumatic events which could create discomfort and reduce their quality of life.
We also propose conservative management of such lesions in patients with essential thrombocythemia because the underlying pathology could complicate major surgical treatment. Bionect Start® appears to be useful for this indication and to permit rapid wound healing of the lesion with no morbidity for the patient.
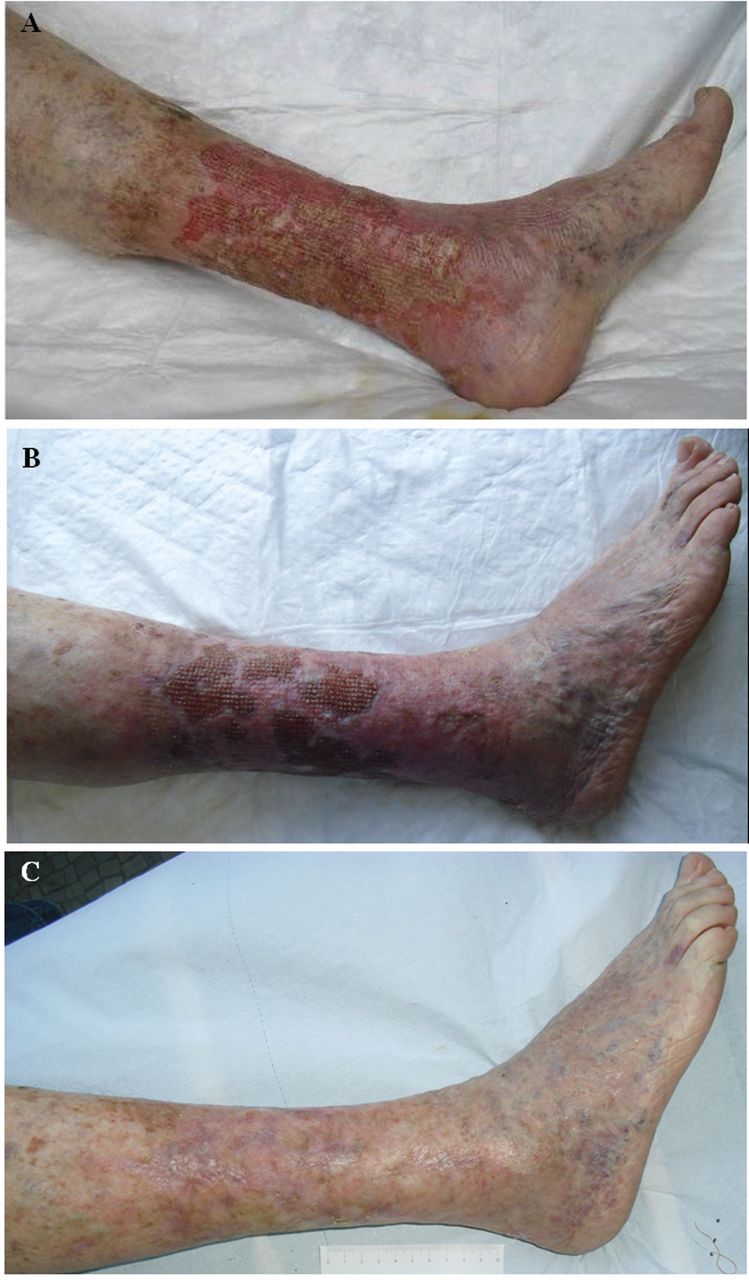
A: At presentation, the lesion extended from the knee to the ankle (25×30 cm), involving the cutaneous and subcutaneous tissues; the bed of the ulcer was highly fibrinous and contaminated. B: Progressive and rapid improvement of the condition occurred, with resolution of the contamination and reduction of secretion, exudates and pain or burning during dressing after one month and a half. C: Complete re-epithelizlization of the extensive loss of substance was apparent after 3 months of therapy.
Acknowledgements
Special thanks to Dr. Franco Bartolomei for his help in preparing this manuscript.
Footnotes
-
Conflicts of Interest
The Authors have no financial interest to declare in relation to the content of this manuscript.
- Received June 21, 2012.
- Revision received September 13, 2012.
- Accepted September 20, 2012.
- Copyright © 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.