


Abstract
Background: The purpose of the present study was to examine the effect of SonoVue™ on right ventricular (RV) dimensions and contractility in patients with heart failure. Patients and Methods: Twenty-four patients were divided into two groups. Group A consisted of 15 patients with heart failure and group B (control) of nine patients without heart disease. SonoVue was administered at low (2 ml) and high (4 ml) doses in both groups separately, in a random order. RV dimensions, contractility, peak systolic pressure gradient from tricuspid regurgitation (TRPG) and the time to maximal RV end-diastolic dimension (EDD), as well as the time for RV-EDD to return to the baseline value (recovery), were calculated in every cardiac cycle starting before the administration of SonoVue (baseline) until the recovery of RV-EDD. Results: Low-(group A, p<0.001 and group B, p<0.05) and high-dose (group A, p<0.0001 and group B, p<0.01) contrast infusion increased the RV-EDD compared to baseline values. TRPG increased significantly (p<0.05) in both groups, under low-as well as high-dose. In group A, high-dose compared to low-dose produced a significant delay in the time duration to max RV-EDD (p<0.05) and in the time to RV-EDD recovery (p<0.0001). Conclusion: The administration of SonoVue in patients with heart failure was followed by an acute, transient, dose-dependent increase in RV-EDD and TRPG, without any effect on RV contractility.
The second-generation ultrasound contrast agents (GUCA-IIs) consist of microbubbles filled with gas that are able to travel through the pulmonary circulation. The durable bubble construction, in combination with the ultrasound interaction, raises the possibility of side-effects during the use of this contrast medium (1).
The adverse effects of GUCA-IIs have been extensively studied. Most studies report on mild allergic reactions, rhythm disturbances, hypotension and other complications (2, 3). However, in addition to mild manifestations, there are some severe side-effects that obscure the safety profile of GUCA-IIs, such as anaphylactic reactions due to complement activation-related pseudoallergy and significant exacerbation of cardiac symptoms, mainly in patients with clinically unstable ischemic heart disease (4-6).
The European Medicines Agency (EMEA) emphasizes on the avoidance of the use of SonoVue™ in patients with acute coronary syndromes, unstable hemodynamic condition, uncontrolled hypertension, adult respiratory distress syndrome and severe pulmonary hypertension (2). Regarding its effects on pulmonary circulation, the results of different studies are ambiguous and insufficient to grant the confidence of either the EMEA or the FDA, resulting in the contraindication of contrast agents use in severe pulmonary hypertension cases (2, 7-10).
The purpose of the present study was to examine the effects of the GUCA-II SonoVue on right ventricular dimensions and contractility in patients with heart failure, and to investigate whether there is a dose-related interaction between the contrast agent and RV function.
Patients and Methods
Study population. Twenty-four patients (17 males) were studied in two groups. Group A consisted of 15 patients suffering from heart failure, NYHA class II and III, and group B (control group) contained nine patients without heart or respiratory disease. The study was approved by the Scientific Committee of the Alexandra University Hospital and all participants gave their written informed consent at enrolment.
Echocardiography. Studies were performed using a commercially available GE Vivid 7 Dimension system (GE Vingment Ultrasound, Horten, Norway) with a broad bandwidth 2-4 MHz transducer. Images were obtained from the apical view (standard 2- and 4-chamber views).
The RV end-diastolic dimension (EDD) at the level of the tricuspid valve annulus in late diastole, at the time of maximal tricuspid opening, and the end-systolic dimension (ESD) at the time of minimum reduction of the RV chamber, were measured from the conventional 4-chamber view. The fractional shortening (FS) of the RV was calculated by the formula: FS(%)=(EDD–ESD) × 100/EDD. The tricuspid regurgitation was evaluated qualitatively by color-flow Doppler imaging. The peak systolic transvalvular gradient, which is correlated with the peak systolic pulmonary pressure, was calculated by continuous wave Doppler measurement of the tricuspid regurgitation. Additionally to the conventional 2-D echocardiography, tissue Doppler imaging (TDI), was performed at the tricuspid annulus to assess the peak systolic tissue velocity (sTDI) as an index of RV systolic function. LV end-systolic and end-diastolic volumes were measured from the conventional apical 2- and 4-chamber images and the left ventricular ejection fraction (LVEF) was calculated by the modified bi-plane Simpson's method (11).
SonoVue™ (Bracco Inc., Milan, Italy) was used in this study. SonoVue contains microbubbles, each of which consists of a phospholipid shell filled with sulfur hexafluoride (SF6).
Study protocol. A standard echocardiographic study was performed focused on the precise RV measurements. A low-(2 ml) and high-dose (4 ml) solution of SonoVue was administered at both A and B groups, as an intravenous slow bolus injection (5 s) in a random order. Values when the RV-EDD reached its maximum were considered as maximal and recovery was defined as the time when RV-EDD returned to the baseline value. Repeated measurements of the RV-EDD and RV-ESD in every cardiac cycle were performed, starting at 10 s before the administration of the contrast agent (baseline) until the return of RV-EDD to the baseline value (recovery).
Once the patient had been stabilized following the initial low- or high-dose administration, contrast agent was given at a different dose and the protocol was repeated. The time from baseline to maximum RV-EDD and the recovery time were recorded. Percentage changes of RV-EDD, RV-ESD, FS, TRPG and sTDI from baseline values during the infusion were calculated. The interobserver variability was assessed on RV measurements by two readers. Intraobserver variability was evaluated by one reader after ten days. Inter- and intraobserver variability was 8±3% and 4±2%, respectively. Blood pressure and heart rate were recorded during the administration of the study agent.
Statistical analysis. Continuous data are presented as mean values±SD. The between-groups analysis was performed using the independent samples t-test, while the intragroup comparisons were made using the paired Student's t-test. Data were analyzed using the SPSS (SPSS Inc., Chicago, IL, USA) statistical software package (version 11.5). A p-value of ≤0.05 was considered statistically significant.
Results
The differences in baseline clinical and echocardiographic characteristics between the patients with heart failure and the control group are presented in Table I. Patients with heart failure had significantly larger RV-EDD and RV-ESD, greater TRPG and lower sTDI and LVEF in comparison to the control group.
Comparison between patients with heart failure and the control group showing baseline clinical and echocardiographical characteristics.
A total of 2,930 measurements of RV were performed before and during contrast infusion. The effect of low- and high-dose contrast administration on RV parameters was found to be comparable in patients with heart failure (group A) and the control group (group B). Low- as well as high-dose SonoVue produced an increase of RV-EDD (p<0.001 and p<0.0001, respectively, in group A and p<0.05 and p<0.01 in group B; Table II, Figure 1) and of TRPG (p<0.05 for both doses and groups). RV–ESD, sTDI and heart rate did not change significantly under low- or high-dose administration in either group (p>0.05). The high dose produced an increase of RV-FS in patients with heart failure (p<0.001) and the control group (p<0.005), whereas with the low-dose, the increase was non-significant in both groups. The change produced in RV-EDD in both groups by high-dose contrast administration (p<0.01 for both) and its time to reach maximum (p<0.05 for both), as well as the recovery time (p<0.0001 for group A and p<0.05 for group B), were all significantly greater the change produced in the case of low-dose administration (Table III, Figure 2). The effect of the high- and low-dose on changes in RVESD, sTDI and TRPG was similar in both groups (p>0.05). However, the high-dose produced a significant increase in FS in the control group (p<0.05), whereas in patients with heart failure the increase was not significant (p>0.05).
Discussion
In our study, we compared the effect of SonoVue administration on RV dimensions and function, as well as the trans-tricuspid systolic pressure gradient (calculated by the tricuspid regurgitation) as an index of pulmonary pressure, in patients with heart failure and in healthy controls. Our findings indicated that the contrast agent produced a significant transient increase in RV-EDD without affecting RV contractility in both groups, independently of the administered dose. RV sTDI did not change significantly, nor did RV-FS under low-dose administration, although the latter increased at the high-dose. These findings are in accordance with our previous experimental results in healthy pigs, where contrast agent infusion was followed by an acute transient increase of RV-EDD, RV-ESD, RVFS, and pulmonary pressure in both the low-dose and high-dose groups, but the increase was greater in the high-dose group (1). A possible mechanism explaining the effect of the contrast agent on RV hemodynamics could be that transient hypoxic pulmonary vasoconstriction resulted in an increase in RV afterload, which was associated with an increase in RV dimensions and contractility. Our findings are in accordance with previous experimental work in pigs by Wauthy and co-workers, who showed that RV contractility increased in proportion to RV afterload (12). TRPG increased significantly in both groups, independently of the administered dose. Previous experimental studies with Albunex and SonoVue showed a dose-dependent acute increase of pulmonary pressure in pigs, which was explained by the release of thromboxane A2 from the pulmonary intravascular macrophages during phagocytosis of the microspheres (1, 12, 13). In patients with heart failure or pulmonary hypertension, Albunex infusion produced an increase of diastolic pulmonary artery pressure (14, 15). However, the direct effect on RV dimensions was not examined, nor was there any comparison with a control group (10). The importance of the dose-dependency effect on RV hemodynamics is supported by the time delay in RV-EDD increase and recovery, which was manifested long after high-dose administration compared with low-dose administration in both groups. These findings confirm our previous experimental work in healthy pigs (1). Moreover, the change in RV-EDD in both groups was greater after high-dose contrast administration than after low-dose.
The effect of low- and high-dose contrast administration on right ventricular function in patients with heart failure and the control group.
Comparison between low- and high-dose effects on right ventricular changes in patients with heart failure and the control group.
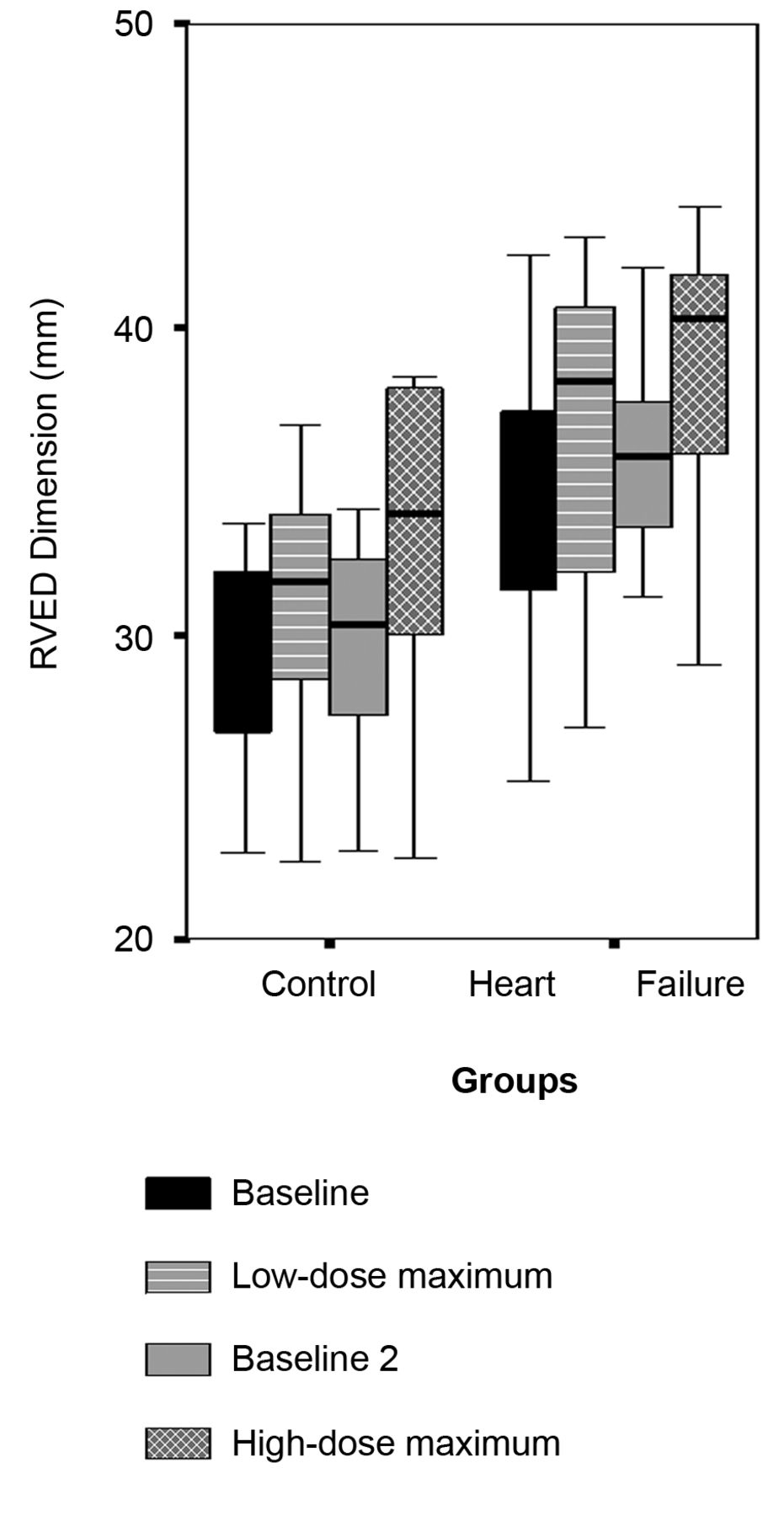
The effect of low- and high-doses of SonoVue on right ventricular end-diastolic dimension (RV-EDD) in patients with heart failure and controls. Both low- and high-doses of SonoVue produced a significant increase in RV-EDD from the baseline values in the control group and in patients with heart failure. Baseline, RV-EDD before low-dose contrast administration; Baseline 2, RV-EDD before high-dose contrast administration; Low-dose maximum, the maximum RV-EDD during the low-dose administration; High-dose maximum, the maximum RV-EDD during the high-dose administration.

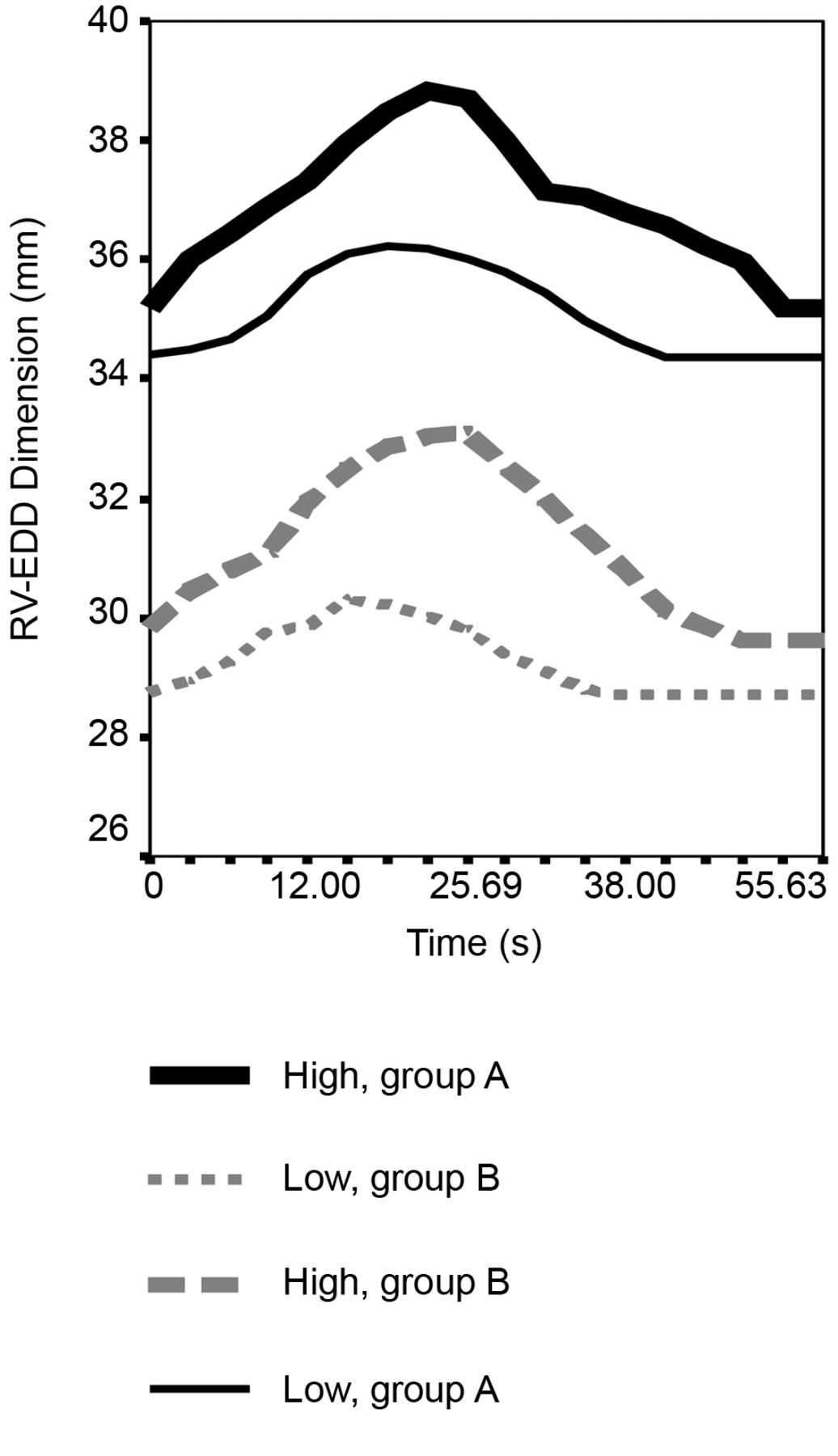
Diagram depicting the effects of low- and high-dose on right ventricular end-diastolic dimension (RV-EDD) and its time course pattern to maximum and to recovery in patients with heart failure (group A) and to the control group (group B). High-dose administration in both groups produced a significantly greater change in RV-EDD, time duration to maximum and time duration to recovery of RV-EDD in comparison to low-dose administration (Table III).
A large post-marketing analysis of SonoVue revealed severe fatal reactions in 0.002% and non-fatal in 0.019% of patients who received this contrast agent (16). Geleijnse et al. found that the frequency of adverse reactions after sulphur hexafluoride echo contrast agent administration was higher than in some previous reports (17). The combination of these findings with the EMEA recommendations has raised questions regarding the safety of SonoVue (2, 8). In other words, the risk-benefit ratio of contrast use must be taken into account, as well as the possible destabilization of critically ill patients. In our study, the patients with heart failure were in a steady state, without severe RV failure or symptoms of congestion. However, administration of the contrast agent directly caused a significant and dose-dependent effect on RV dimensions and TRPG, without signs of left ventricular failure. This raises the question of what might be the impact of SonoVue on patients with RV failure. Therefore, the warning of EMEA regarding the use of SonoVue in patients with pulmonary hypertension, must be taken into consideration, especially for those under unstable hemodynamic conditions (2).
Limitations. An inherent limitation of our study was the improvement of the Doppler signal after contrast infusion, which may have affected the accuracy of TRPG measurements. Moreover, a blinded analysis of images was difficult to conduct because the images before and after contrast administration were quite different.
Conclusion
The administration of GUCA-IIs in patients with heart failure creates an acute, transient, dose-dependent increase of RV-EDD dimension and TRPG, without any effect on RV contractility. Therefore, the use of SonoVue in patients with pulmonary hypertension must be taken into consideration, especially for those under unstable hemodynamic conditions.
Footnotes
-
Conflicts of Interest
All Authors have read and approved the manuscript. We declare that no Author has any commercial associations that might pose a conflict of interest in regard with the submitted article.
- Received March 28, 2012.
- Revision received May 29, 2012.
- Accepted May 30, 2012.
- Copyright © 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.