


Abstract
Angiomyolipomatous hamartoma is a variant of angiomyomatous hamartoma (AMH), a rare nodal smooth muscle proliferation, first identified as a distinct entity by Chan et al. in 1992. To date, several cases have been described, mostly involving inguinal lymph nodes. We present two cases of angiomyolipomatous hamartoma, in a 52-year-old male and 67-year-old female patient. Both patients were surgically treated. Microscopically, in the affected nodes, the parenchyma was mostly replaced with bundles of smooth muscle cells, fibrous tissue and lobules of mature adipocytes. Only a few atrophic lymphatic follicles were maintained in the subcapsular area. The presence of smooth muscle cells and endothelial cells was confirmed immunohistochemically by staining for smooth muscle actin, desmin and CD31. The hilus contained numerous thick-walled vessels extending to the medulla. Pleomorphism, mitoses and necrosis were absent. Considering there are no reported recurrences of AMH, it probably has benign behaviour; thus extensive resection may not be needed. Nevertheless, we believe that recognition of AMH is important in the differential diagnosis of other pathological conditions that may affect lymph nodes.
Angiomyomatous hamartoma (AMH), a rare primary tumor of lymph nodes characterized by replacement of nodal parenchyma by a mixture of blood vessels, smooth muscle cells and fibrous tissue, was first described in 1992 by Chan et al. (1). Originally classified as a vascular tumor, it was later included in smooth muscle proliferations of lymph nodes, along with hilar smooth muscle proliferation, angiomyolipoma, lymphangiomyomatosis, leiomyomatosis and intranodal leiomyoma (2). Although it seemed that AMH only occurs in inguinal and femoral nodal regions, isolated cases in submandibular, cervical and popliteal lymph nodes were subsequently described (3-7). The hamartomatous nature of the lesion was postulated owing to disorganized growth pattern of smooth muscle cells and blood vessels, rather than fascicle formation (1). Typically, AMH is a pathological condition starting in the hilum with extension towards the cortex. Allen and Hoffman (8) were the first to report the presence of an adipose tissue component in AMH, while Magro and Grasso (9) suggested such variants should be termed angiomyolipomatous hamartoma (AMLH). Here, we report two cases of AMLH in the inguinal lymph nodes.
Case Reports
Patient 1. A 52-year-old male was admitted to the hospital due to a painful swelling in his left groin which had grown in a few weeks. On clinical examination, besides a palpable tumour, there were no other abnormalities. The tumour was surgically removed. According to the surgical report, the lesion was deeply infiltrating the muscles, tendons and other surrounding tissue. Grossly, the tumour mass measured 9 cm in diameter and contained two lymph nodes measuring 4.7 and 1.1 cm in diameter. The nodes had a yellowish-brown cut surface, and appeared to have been almost completely replaced with adipose tissue. Allong with tumorous tissue, adjacent muscles and normal appearing lymph nodes were received. The pathohistological findings were compatible with the diagnosis of AMLH (see below). At present, ten months after diagnosis, the patient is well and without any signs of recurrence.
Patient 2. A 67-year-old female patient was incidentally found to have a tumour in the right inguinum during an ultrasound examination performed for leg varices. The tumour measured 1.4 cm in diameter and appeared to be well vascularised. Clinically, the patient had only a minor swelling in her right groin, without any signs of inflammation or oedema. The tumour was surgically removed. Grossly, the material consisted of adipose tissue with a lymph node measuring 1.6 cm in diameter. The diagnosis of AMLH was made by pathohistological analysis (see below). Three months after the diagnosis, the patient is well and without any signs of recurrence.
Cases of angiomyomatous hamartoma with or without fat tissue component, reported in the literature to date.
Pathohistological findings. Microscopically, the tumorous lymph nodes from both patients had only partially-preserved parenchyma. Lymphoid tissue had been almost completely replaced with bundles of smooth muscle cells, fibrous tissue and lobules of mature adipocytes, growing in a disorganized fashion. Only a few atrophic follicles in the subcapsular area were maintained (Figure 1). Smooth muscle cells were confirmed immunohistochemically by positive reaction for smooth muscle actin (SMA) and desmin, while endothelial cells were positive for CD31 (Figure 2). Reaction for human melanoma black 45 (HMB-45) was negative in both cases. The hilus contained numerous thick-walled vessels with extension to the medulla. Cellular pleomorphism, mitoses and necrosis were not observed.
Discussion
AMLH of a lymph node is a rare benign condition primarily affecting the hilum, characterized by haphazardly arranged bundles of fibrous tissue, vascular spaces, smooth muscle cells and fat lobules. The lymphoid tissue is usually only preserved in the thin subcapsular area. According to reported cases, there is a male predominance of almost 2:1 and a predisposition for the lymph nodes of inguinal region. All the reported cases are summarized in Table I (1, 3-15). The pathogenesis of AMH remains unclear. Some authors suggest it is developed as a secondary reaction to nodal inflammation, considering lymph nodes can undergo vascular proliferation in response to various stimuli. This idea was supported by Kim et al. (5) in their case of concurrent AMH of popliteal lymph nodes and diffuse pigmented villonodular synovitis of the knee. They assumed AMH may have evolved as a proliferative reaction to the inflammatory process of the knee. To our knowledge, our patients did not have any condition of that kind, which could have predisposed to development of hamartoma. In general, patients with AMH have nonspecific symptoms, if any. Local tenderness and swelling, similar to those in our patients, are usually reported. It is obvious that this condition may interfere with lymphatic drainage, as ipsilateral limb oedema was reported in several cases (1, 10, 12-14). Our patients did not have any signs of oedema. We can assume that several lymph nodes should be altered, with fibrosis of adjacent tissue, or there should be a concomittant disease influencing the lymphatic drainage, in order for oedema to develop. Some authors suggest impaired lymphatic flow is not just a consequence of hamartoma but may actually play a role in its pathogenesis (15). Several authors reported additional histological findings in AMH. As mentioned before, the first was the presence of fat lobules (8), which we found in both of our cases. We believe adipose tissue is a component of hamartoma, although some authors argued it merely represents metaplasia, not being linked to hamartoma. Dargent et al. reported alterations in lymph node vascular supply which included an increased number of small blood vesssels with thickened walls, forming glomeruloid structures similar to those in primary pulmonary hypertension or glioblastoma multiforme (14). The thick-walled vessels were also prominent in our cases as well as in most cases reported so far, making this a characteristic feature.

In angiomyolipomatous hamartoma, apart from the thin rim of lymphoid tissue in subcapsular area, the majority of lymph node parenchyma can be seen to have been replaced by smooth muscle cells, blood vessels, fibrous and adipose tissue (HE, ×40). Case 1 (A); case 2 (B).
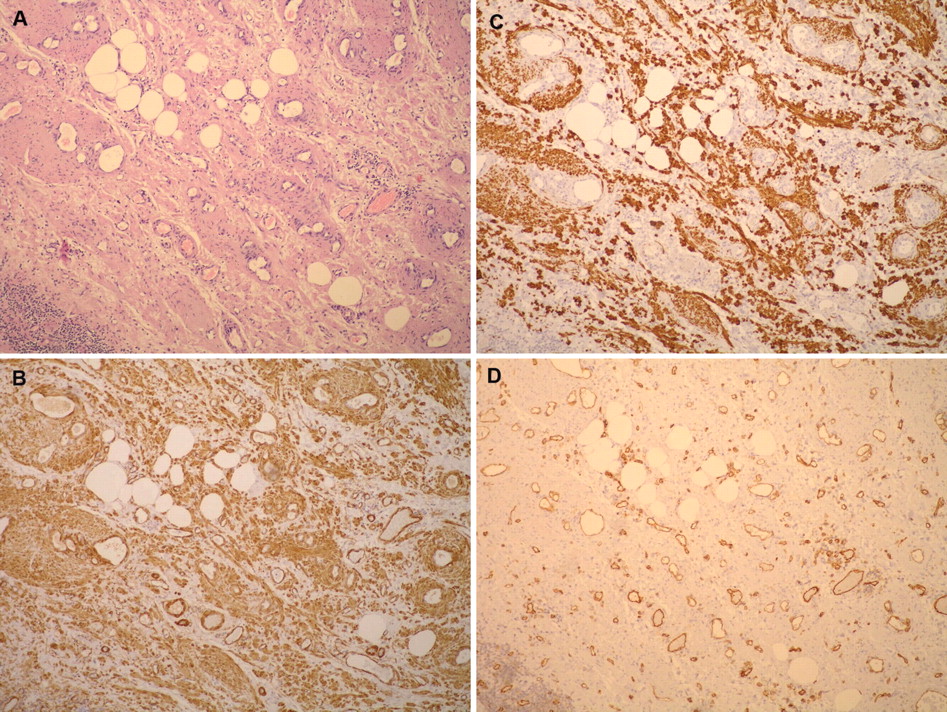
Angiomyolipomatous hamartoma on HE slide, under medium magnification (×100; A), and the same area showing positive immunohistochemical reaction for smooth muscle actin (B), desmin (C) and CD31 (D) (case 1).
The exclusion of smooth muscle proliferations, lymphangiomyomatosis and leiomyomatosis as differential diagnoses should not pose a problem, considering the characteristic histological features of AMH, lacking the fascicle formation typical of the aforemetioned conditions.
Angiomyolipoma most commonly occurs in retroperitoneal lymph nodes, in which AMH has not yet been reported. Moreover, it usually appears as a multifocal condition in conjunction with renal tumour of the same type (2). Angiomyolipoma can be usually diagnosed without histology, by a combination of ultrasound and computed tomography, but the simultaneous lymph node involvement may raise suspicion of metastatic disease. Although composed of the same tissue types as AMH, the smooth muscle component in angiomyolipoma may exhibit hypercellularity, pleomorphism and mitotic activity not reported in hamartoma. Moreover, angiomyolipoma has a typical immunohistochemical phenotype with HMB-45 positivity, which was negative in both of our cases (16).
In summary, AMH is a benign pathological condition, recognition of which is important in differential diagnosis of other benign and malignant tumours affecting lymph nodes. To date, there have been no recurrences reported, meaning that extensive resection may not be needed.
Acknowledgements
This work was presented in part at the 23rd European Congress of Pathology, August 27th to September 1st 2011, Helsinki, Finland. It was supported in part by the Ministry of Science, Education and Sports, Croatia, project number 108-1081870-1884.
- Received February 3, 2012.
- Revision received February 27, 2012.
- Accepted February 28, 2012.
- Copyright © 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.