


Abstract
Secondary diffuse leptomeningeal gliomatosis, in which a glioma of the brain or spinal cord infiltrates the leptomeninges, is an uncommon clinical metastatic complication of malignant glioma, for which there is no consensus regarding treatment. In an ante mortem series in which the diagnosis of leptomeningeal gliomatosis was based on neuroradiological results, an incidence of 2% was reported. The appearance of leptomeningeal gliomatosis is a pre-terminal event. Case Report: A 44 year-old woman rapidly developed intracranial pressure and impairment of cognitive function. A huge right temporal tumor was diagnosed and an incomplete resection performed. Histology showed it was a glioblastoma and a concurrent radiation therapy with temozolomide was administered. Her clinical status was subnormal. A first course of adjuvant chemotherapy, temozolomide, was administered, and her neurological status suddenly worsened in days: deterioration of cognitive function status, inability to walk, and aphasia were reported. The cerebrospinal fluid showed an elevated protein content of 2 g/l, and glucose concentration was low. Cytology of cerebrospinal fluid showed no malignant cells. Systemic nitrosourea chemotherapy (fotemustine) was administered. Intrathecal sustained-release cytarabine, Depocyt®, was initiated (an induction cycle followed by a consolidation). After a second intrathecal infusion, her clinical status significantly improved, and she was discharged to a medical unit. The duration of response was approximately 6 months. Conclusion: Intrathecal infusions of Depocyt®, recommended for the treatment of lymphoma neoplastic meningitis, seems to be effective in treatment of secondary diffuse leptomeningeal gliomatosis.
Glioblastoma multiforme (GBM) accounts for 45 to 50% of all gliomas and is the most common primary central nervous system neoplasm, as well as being among the most aggressive tumors (1-4). Median survival is generally less than one year from the time of diagnosis, and even in the most favorable of situations, most patients die within two years (1-4). Leptomeningeal gliomatosis of GBM has been reported in 15-27% of glioma patients in a post-mortem series (5). The appearance of leptomeningeal gliomateosis is a pre-terminal event but symptomatic leptomeningeal gliomatosis is found in only 2-7% of patients with supratentorial malignant glioma (6).
Secondary leptomeningeal gliomatosis usually results from dissemination from a parenchymal tumor via the cerebrospinal fluid (CSF) (7-11). Patients with leptomeningeal gliomatosis typically present with headache, confusion, and multifocal signs, including cranial nerve palsy (6, 11-12). The treatment of patients with glioma and leptomeningeal gliomatosis is particularly challenging because most patients have compromised neurological functions attributable to both treatment and the topography of their primary tumors (7-11).
We describe the case of a woman who developed a secondary leptomeningeal gliomatosis four months after tumor resection and who went into temporary clinical remission after intrathecal infusions of Depocyt®.
Case Report
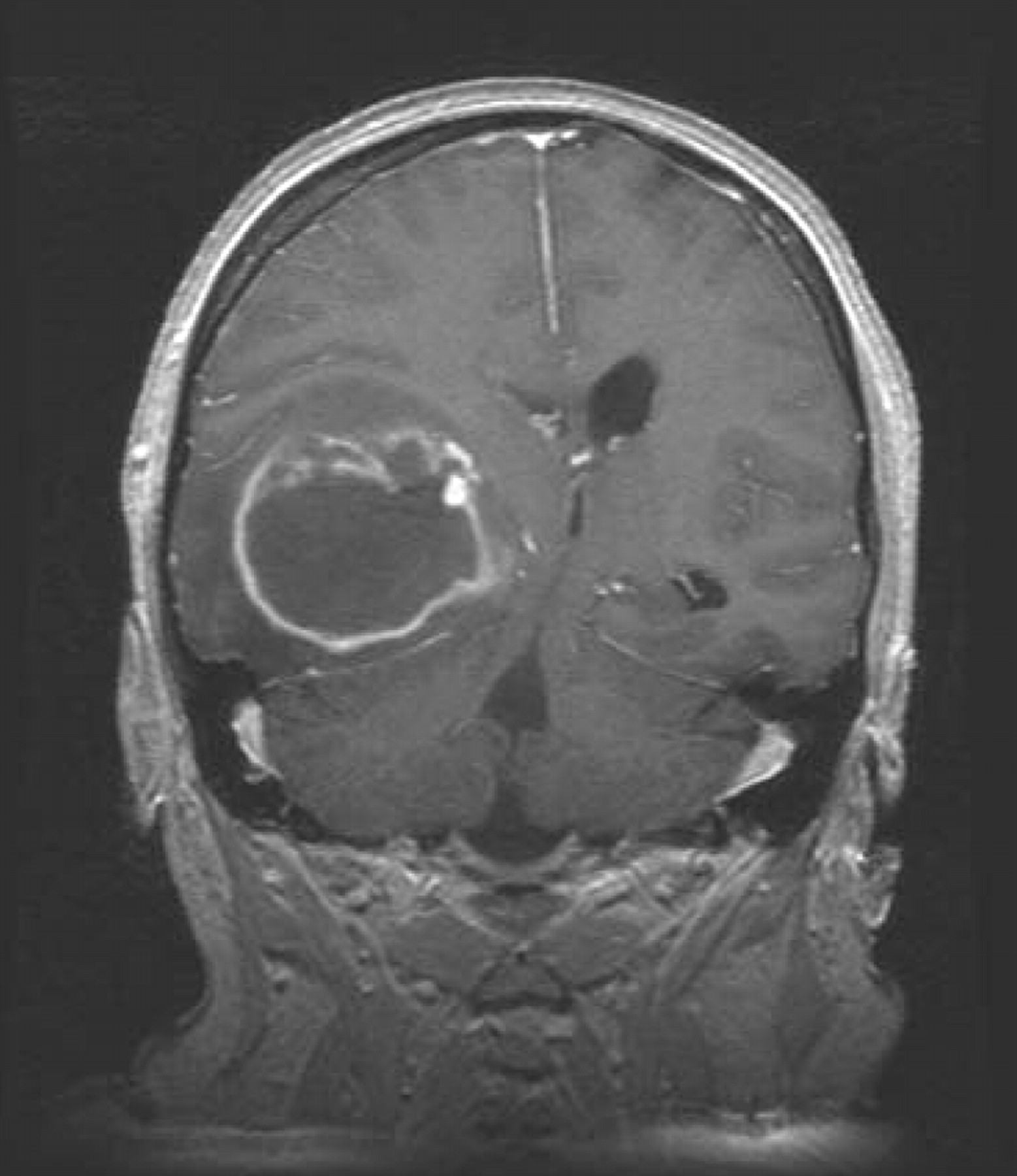
A 45-year-old, right-handed, woman presented with a 3-week history of progressively increasing headache and cognitive disturbance. She was a lifelong smoker. She was afebrile and confused. Nausea and vomiting were noted. Examination revealed raised intracranial pressure syndrome, confusion and a slowing down to ideomotor status. Cranial magnetic resonance imaging (MRI) revealed a large heterogeneously enhanced mass in the right temporo-occipital area, with edema and compression of the right lateral ventricle (F1). In December 29, 2006, a craniotomy followed by incomplete tumor resection was performed. A glioblastoma multiforme (GBM) according to the WHO classification was diagnosed after examination of a tissue sample. The postoperative course was marked by the disappearance of both confusion and the intracranial pressure syndrome. A concurrent administration of temozolomide with fractionated cranial irradiation was delivered over a period of six weeks. One month after the end of radiation therapy, the first course of adjuvant chemotherapy, temozolomide, was administered.

Magnetic resonance imaging revealed a large enhanced tumor of the right temporal area with major compression of right lateral ventricle.
During the first cycle of adjuvant chemotherapy, the patient's neurological status progressively worsened; confusion, aphasia and unsteadiness with frequent falls, were noted. She was admitted as an emergency case to the Neurooncology Department. Examination reported bilateral limb weakness, walking disabilities, raised intracranial pressure syndrome, confusion, drowsiness, and aphasia. No cranial nerve palsies were noted. Computered tomography scan (CT) displayed a heterogeneously enhanced tumor in the right temporo-occipital area, with suggestion of enhancement of the right temporal ventricular surface. Leptomeningeal gliomatosis was suspected and a lumbar puncture was performed; the CSF showed an elevated protein content of 2 g/l, and glucose concentration was low. Cytology of CSF showed no malignant cells. The PCR assay for M. tuberculosis, Ziehl-Neelsen stain, cryptococcal antigen, cytology and culture were negative. Despite the absence of glioma tumour cells in the CSF, secondary leptomeningeal gliomatosis was diagnosed.

Magnetic resonance imaging showed a dissemination of gliomatosis along the wall of the right lateral frontal ventricle, despite the oncologic treatment.
A systemic nitrosourea-based chemotherapy of fotemustine was administered as a monthly intravenous perfusion of 100 mg/m2/day. A total of six cycles were performed. It was decided to initiate Depocyt®, an intrathecal sustained-release, a formulation of cytarabine as follows: an induction treatment of one injection every 15 days for five injections was given, followed by a consolidation treatment of one injection monthly for five injections. After the second injection, the clinical status of the patient dramatically improved; the confusion and aphasia disappeared, the walking disabilities improved, and bilateral limb weakness was moderate. The intrathecal infusions of Depocyt® continued, and the patient received a total of eight intrathecal injections of Depocyt® (an induction treatment and 3 injections of consolidation treatment). The patient was finally discharged to a medical unit. The duration of clinical response was approximately 6 months. Despite of the combined therapy (systemic chemotherapy and intrathecal chemotherapy), the patient's clinical course deteriorated (F2), and she died in October 2007. No post-mortem examination was performed.
Discussion
Leptomeningeal gliomatosis is a clinically uncommon metastatic complication of malignant glioma for which there is no consensus regarding the therapy (7-11). It is known that longer survival of glioma patients may account for the apparent increase in the incidence of leptomeningeal gliomatosis (14). The diagnosis of this leptomeningeal involvement remains straightforward, but it is difficult to distinguish leptomeningeal gliomatosis from other causes of chronic meningitis (4, 9, 11).
The clinical presentation of our patient was similar to other reported cases in the literature, but no cranial nerve palsy was noted and the time to appearance of secondary leptomeningeal gliomatosis was short (6, 11-13). The CSF showed a high protein concentration, but no glioma cells were detected (15). CT scan showed the residual tumor, and suggested an enhancement of the right temporal horn. The diagnosis of secondary leptomeningeal gliomatosis was finally evoked after taking into account the clinical, radiological and biochemical data.
Although the use of intrathecal chemotherapy (IT) is controversial, because of reported variable efficacy and neurotoxicity, studies have demonstrated that this therapy may extend survival in patients with leptomeningeal metastasis to 2–6 months (11-12). Sustained release cytarabine, Depocyt®, which is a liposomal formulation, is approved for the treatment of lymphomatous meningitis, and a few phase III studies have demonstrated that it improves quality of life and has a moderate efficacy for patients with neoplastic meningitis (16). The presentation of an antineoplastic drug in multivesicular liposomes reduces administration to once every two weeks. Drug concentration is diffuse in the CSF and high in the ventricular compartment, thus avoiding the need for an intraventricular reservoir (17). Depocyt® therapy is divided into two parts: an induction phase (one injection every two weeks for five injections) and a consolidation phase (one injection every month for five injections) (16-17). To prevent the main secondary effect of a meningitis reaction, corticoid therapy is recommended for a few days (16-17).
To the best of our knowledge, this is the first time that a clinical response has been obtained with sustained release cytarabine in secondary leptomeningeal gliomatosis. The dramatic clinical improvement of our patient was observed immediately after the second injection, i.e. approximately 3 to 4 weeks after the onset of secondary leptomeningeal gliomatosis. Clinical remission lasted five and a half months, and the patient was able to resume a nearly normal life during that time. Although the role of the systemic chemotherapy used here, fotemustine, is unclear, it is possible that it enhances the efficacy of Depocyt®.
Early diagnosis and aggressive treatment could improve the survival of patients with leptomeningeal gliomatosis and our understanding of this disease. Intrathecal infusion of Depocyt® seems to be effective in secondary diffuse leptomeningeal gliomatosis.
- Received May 19, 2011.
- Revision received June 24, 2011.
- Accepted June 27, 2011.
- Copyright © 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.