


Abstract
Background: The present study was performed to determine the effect of amifostine in the prevention of radiation-induced acute and late period morphologic damages in rat kidney via light and electron microscopic examinations. Materials and Methods: Control rats (n=6) received saline solution 30 min before sham irradiation; the radiotherapy alone group (n=12) received saline solution 30 min before irradiation (a single dose of 15 Gy, applied unilaterally to the kidney) and a final radiotherapy +amifostine group (n=12) received 200 mg/kg amifostine 30 min prior to irradiation. Results: Microscopic examinations of irradiated kidneys revealed presence of glomerular tuft capsular adhesion, fusion of the foot processes and ballon-like cellular degeneration and loss of luminal brush border in tubules as early as eight weeks after irradiation. By 24 weeks post-irradiation, these changes were advanced and associated with focal mesangiolysis, segmental sclerosis and focal tubular atrophy. In addition, local irradiation caused interstitial fibrotic lesions in the kidney. Pretreatment of amifostine markedly prevented these glomerular and tubular changes, and interstitial fibrotic lesions. Conclusion: This study suggests that amifostine pretreatment may contribute to prevention of radiation-induced acute and late nephrotoxicity.
The kidney is one of the most radiosensitive organs and is dose-limiting in cancer patients treated with total-body or abdominal irradiation. Radiation nephropathy is characterized by a slow and progressive reduction of renal function that leads to renal failure (1).
In recent years, amifostine (WR-2721) has been introduced in cancer clinical trials to study its protective effects against normal tissue damage caused by irradiation and various chemotherapeutic agents (2-3). It has been shown that amifostine protects irradiated gastrointestinal mucosal tissue (4), salivary gland (5), bone marrow (6), testis (7), skin (8), lung (9), liver (10) and kidney (11-12) tissues in experimental animals. The mechanism of cytoprotection offered by amifostine is complex and not completely understood, but is most probably due to scavenging of free radicals in competition with oxygen (13). The effectiveness of amifostine at diminishing the histopathologic and functional damage in the irradiated kidney has been shown in a few studies (11-12), however, to the Authors' knowledge, there have been no morphological studies examining the kidney ultrastructure in rats treated with amifostine before irradiation to date. Therefore, the present study was performed to determine the protective effects of amifostine on morphology of irradiated rat kidney in acute and late period via light and electron microscopic examinations.
Materials and Methods
Animals. All experimental protocols were approved by the Local Ethics Committee and carried out in the Trakya University Experimental Animal Center. Thirty male Wistar albino rats, weighing 250-300 g, aged 8-12 weeks were included in the study. All animals were housed at 21°C under a 12-h light–dark cycle. They were fed a standard pellet diet for rats and were allowed tap water to drink ad libitum.
Experimental design. The animals were randomly divided into three groups: 1 (control, CL), 2 (radiotherapy alone, RT), 3 (radiotherapy +amifostine, RT+AMI). Group 1 (n=6) was treated with 0.9% saline solution (SS), by intraperitoneal (i.p.) injection 30 min prior to sham irradiation. Group 2 (n=12) received SS, i.p., 30 min before unilaterally applied kidney irradiation. Group 3 (n=12) received 200 mg/kg, i.p., amifostine (Ethyol, MedImmune Pharma BV, the Netherlands) which was dissolved in SS, 30 min prior to irradiation.
Irradiation. Prior to radiotherapy, the rats were anesthetized with xylazine/ketamine (10/90 mg/kg, i.p.) and restrained at their upper and lower extremities across a 30×30×6 cm styrofoam block (Med-Tec, Orange City, IA, USA) in prone position. Correct positioning of fields was controlled for each rat via a therapy simulator (Mecaserto, Simics, Paris, France). The left kidneys of the animals were visualized by intravenous pyelography (Omnipaque, Amersham Health, Cork, Ireland). Kidney dimensions were approximately 2×2 cm (length×width) on fluoroscopy and an irradiation field of 3.5×3.5 cm was traced on animals posteriorly with a central cross. A peripheral shielding block of 3.5 half-value layer was used in order to shape the irradiation field in respect to the kidney. To correct irregularities in contour and to compansate for skin sparing effects, a 1.5 cm elastogel bolus was used. RT and RT+AMI groups were irradiated individually with a single dose of 15 Gy with 6 MV photons using a linear accelerator treatment unit (Varian, Clinac, 2100 C/D, CA, USA) at a source-skin distance of 100 cm to the entire left kidney. Dose rate was 600 MU/min. The dose was calculated at a depth of 2 cm from the skin (3.5 cm from the surface of the bolus material) as the kidney depth was 1.5 cm posteriorly on computerized tomography. The control group received equal-field sham irradiation.
Morphological asessment. At 8 and 24 weeks after irradiation, six animals from groups two and three, and at the end of experiment all animals from the control group, were sacrificied by cervical dislocation, and the left kidneys of each animal were removed immediately and weighed. The kidneys were cut into halves parallel to the long axis. The specimens of the all groups were processed for light and electron microscopic examinations.
Light microscopic examination. The kidney specimens were individually fixed in Bouin's solution, dehydrated in alcohol and embedded in paraffin. Sections of 5 μm were obtained, deparaffinized and stained with hematoxylin-eosin (H&E), periodic acid Shiff (PAS) and Masson trichrome. To evaluate interstitial fibrosis, 20 fields in one section from each animal were assessed on Masson trichrome-stained sections (×200). Semiquantitative analysis in each field was assessed as follows: 0=no fibrosis; 1=fibrosis in <10% of the area; 2=fibrosis in 10-25% of the area; 3=fibrosis in 25-50% of the area; 4=fibrosis in>50% of the area. Interstitial fibrosis grade was calculated as a percentage (%) for each group. These microscopic evaluations were performed in a random order under blindfold conditions with standard light microscopy.
Transmission electron microscopic examination. For electron microscopical observation, left kidney specimens of 1×2 mm size were fixed in 2.5% glutaraldehyde in 0.1 M phosphate buffer and after primary fixations tissues were washed in 0.1 M phosphate buffer overnight. The tissues were postfixed with 1% osmium tetraoxide in phosphate buffer for 1 h at 4°C. Then the postfixed tissues were washed in 0.1 M phosphate buffer and dehydrated by graded ethyl alcohol and finally with propyleneoxide. Dehydrated tissues were processed for making araldite blocks. Ultrathin section were obtained by ultramicrotome (RMC-MTX Ultramicrotome-USA) and collected on copper grids for double staining (uranyl acetate and Reynold's lead citrate). Stained sections were finally observed under a Jeol-JEM 1010 transmission electron microscope.
Statistical analysis.The quantitative data were expressed as mean± standard deviation (SD). Analysis of variance (ANOVA) followed by Post-hoc Tukey HSD test was used to determine statistical significance. Qualitative data between groups were compared using Pearson χ2 and Kolmogrov-Simirnov two samples tests. A p-value <0.05 was considered significant. Statistica (Tulsa, Oklahoma USA) 7.0 software was used for all statistical analyses.
Results
Kidney weight. As shown in Table I, local irradiation with 15 Gy caused no statistically significant alterations in left kidney weights in relation to the individual body weights at eight weeks post-irradiation. At 24 weeks after irradiation, irradiated kidney weight/body weight ratio was significantly less than that observed sham-irradiated controls (p<0.001). At this time, left kidney weights in relation to the individual body weights had decreased by approximately 60% compared with the controls. The pretreatment of amifostine partially prevented these decreases in kidney weights depending on irradiation (p≤0.05).
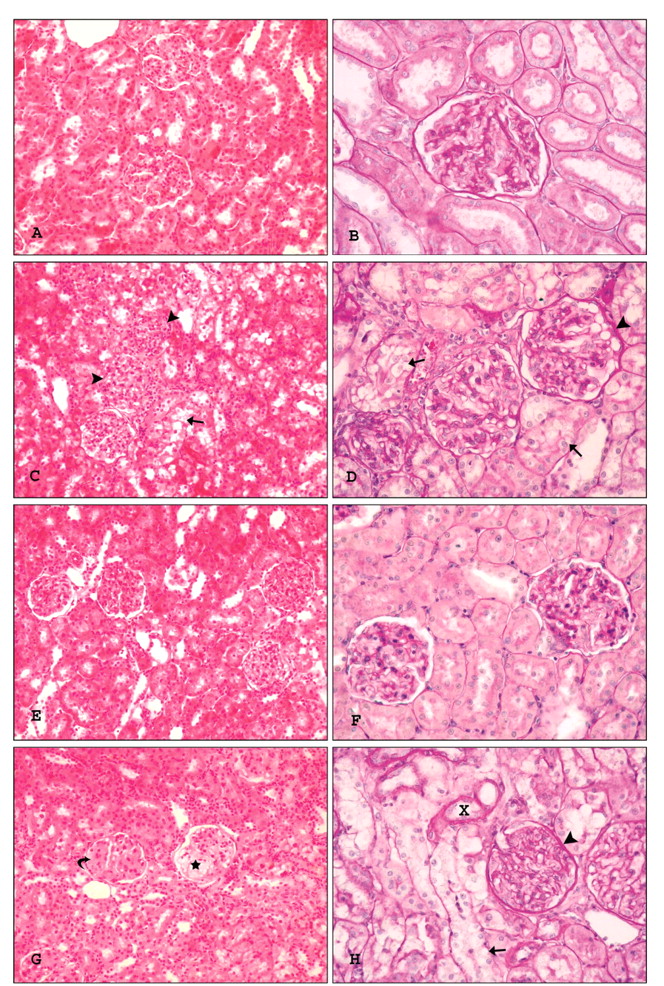
Light microscopic findings. There were no changes in glomerular or tubular structures of control sham-irradiated animals (Figure 1A, B). Morphologically, as compared to the control kidneys, examination of irradiated kidneys showed damage to glomeruli, tubules and interstitial tissue. Radiation-induced alterations at eight weeks postirradiation were limited to foci. At this time-point glomeruli showed glomerular tuft capsular adhesion and thickening of the basement membrane Bowman's capsule. No marked glomerulosclerosis or mesangiolysis was seen. Tubular injury was apparent as ballon-like cellular degeneration, cytoplasmic vacuolization and loss of luminal brush border (Figure 1C, D). The renal parenchymal findings at 24 weeks were similar to those observed at eight weeks, except for progression in the severity of glomerular and tubular cell damage. There was focal tubular atrophy with basement membrane thickening, at this time. In addition, there was clear evidence of segmental sclerosis and focal mesangiolysis in affected glomerules (Figure 1G, H). Pretreatment of amifostine significantly prevented the radiation-induced histopathological changes. Marked reduction of glomerular and tubular damage was seen in irradiated amifostine-pretreated animals (Figure 1E, F, J, K).
Masson trichrome staining of kidney sections did not reveal any interstitial fibrotic changes in the sham-irradiated control animals (Figure 2A), whereas interstitial fibrosis with inflammatory cell infiltrate was observed in the irradiated animals (Figure 2B, D). The area of interstitial fibrosis increased from eight weeks and expanded through 24 weeks post-irradiation in irradiated kidneys. In addition, the expansion of matrix in glomeruli was noted eight weeks after radiation (Figure 2B). By 24 weeks post-irradiation, there was a more prominent expansion or increase of mesangial matrix in glomeruli (Figure 2D). Amifostine pretreatment prominently reduced radiation-induced fibrotic lesions (Figure 2C, E).
Time-related changes in kidney weight/body weight in irradiated and amifostine pretreated kidneys of rats following irradiation of the left kidney alone with a single dose of 15 Gy X-rays.
Semiquantitative analyses of results related with interstitial fibrosis are summarized in Table II. Light microscopic examination of specimens from the radiotheraphy group revealed 12% grade 1, 10% grade 2 and 2% grade 3 interstitial fibrosis at eight weeks postirradiation. Interstitial fibrotic lesions in irradiated-kidneys were significantly improved by pretreatment of amifostine (p<0.05). At 24 weeks after irradiation, interstitial fibrosis grade increased significantly compared with that in radiotherapy (eight weeks) group (p<0.05). Semiquantitative analysis confirmed that amifostine significantly protected against radiation nephropathy. At this time, grade 2 and grade 3 kidney fibrosis were 31% and 3% in the radiotherapy group, while they were 4% and 0% in the amifostine pretreated group (p<0.05).
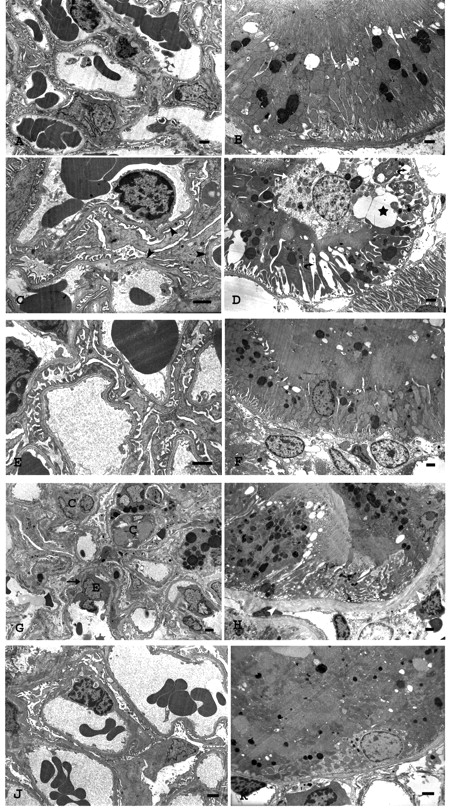
Electron microscopy findings. Electron microscopy study of kidneys from sham-irradiated control rats showed normal glomerular and tubular architecture (Figure 3A, B). Significant pathologic changes were observed in glomerules and tubules of irradiated rat kidney. At eight weeks after irradiation, most of the glomerules were close to normal, although in some areas effacement of podocytes foot processes was observed (Figure 3C). In contrast, ultrastructural findings were of tubular cells characterized by swelling or vacuolization of the cytoplasm, expansion in basal infoldings and partial loss of luminal brush border (Figure 3D). By 24 weeks post-irradiation, lesions of affected glomerules showed sub-endothelial expansion, capillary endothelial cell edema, capillary wall thickening and collapse of capillary loops (Figure 3G). The electron microscopy findings revealed focal tubular atrophy accompanied by markedly thickened and irregular basement membranes at this time-point (Figure 3H). Electron microscopy in the amifostine-pretreated irradiated rat kidney indicated noticeable improvement in both tubular and glomerular ultrastructural lesions. The glomerular endothelium was intact and capillary lumens were normally patent (Figure 3E, J). Tubular changes were also reduced and there was no tubular basement membrane thickening (Figure 3F, K).
Semi-quantitative analysis of interstitial fibrosis in renal tissues.
Discussion
In the kidney, irradiation leads to a progressive reduction in function associated with concomitant glomerulosclerosis and/or tubulointerstitial fibrosis, which largely depends on the total radiation dose, dose per fraction, irradiated volume, and age at the time of irradiation (1).
Amifostine specifically protects normal cells from radiation and antineoplastic drug toxicity by scavenging free radicals, donating hydrogen ions to free radicals, depleting oxygen, and by binding to active derivatives of antineoplastic agents without protecting tumours (13-14). Amifostine is administered as a pro-drug and is rapidly dephosphorylised in the endothelium of capillaries by alkaline phosphatase to its active form, WR-1065 (15), which is instantly taken up into the cells. Thirty minutes after administration, tumours have up to a 100-fold lower WR-1065 concentration compared with healthy tissue, e.g. the kidney (16). Intrarenal amifostine accumulation has been previously demonstrated in experimental animals (17-18). In the present study, the dose and administration schedule of amifostine (200 mg/kg, i.p., 30 min before irradiation) was chosen on the basis of dose–response effects in other preclinical animal studies (9, 18).
The main results of the present study were as follows: (i) the histopathological changes were observed in both glomeruli and tubular epithelium as well as interstitium in the irradiated rat kidney; (ii) the type and severity of these changes increased from 8 to 24 weeks post-irradiation; (iii) at 24 weeks after irradiation, fibrotic lesions increased while the irradiated kidney weight/body weight ratio significantly diminished; (iv) pretreatment with amifostine considerable prevented histopathologic and fibrotic changes in irradiated rat kidney.

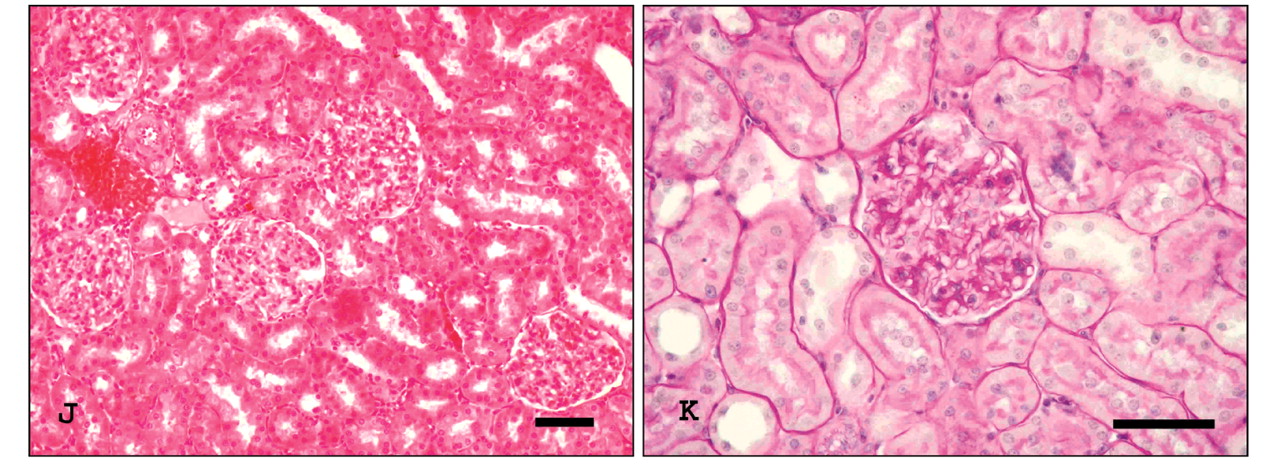
Representative photomicrographs of morphologic changes in rat kidneys. A, B: Control kidney. C, D: Irradiated rat kidneys at 8 weeks, showing glomerular tuft capsular adhesion, thickening of the basement membrane Bowman's capsule in glomeruli (arrowhead) and ballon-like cellular degeneration, cytoplasmic vacuolization and loss of luminal brush border in tubules (arrow). G, H: Mesangial sclerosis (curved arrow), segmental mesangiolysis (asterisk) and tubular atrophy (X) at 24 weeks postirradiation. E, F, J, K: Amifostine-pretreated rat kidneys at the relevant time point, showing marked reduction of glomerular and tubular damage. (A, C, G, E, J; H&E, B, D, H, F, K; PAS) Scale bar: 50 μm.

Representative photographs of Masson trichrome staining in the experimental groups. A: Control kidney. B: Irradiated rat kidneys at the 8 weeks (B) and 24 weeks (D) postirradiation. Interstitial fibrosis with inflammatory cell infiltrate (arrowhead) and increase of matrix in glomeruli (i.e., glomerulosclerosis; arrow) were observed in the irradiated kidneys. C, E: Fibrotic lesions were prominently ameliorated in amifostine-pretreated rat kidneys at the relevant time point. Scale bar: 100 μm.

Representative electron micrographs of ultrastructural glomerular and tubular changes in rat kidneys. A, B: Control kidney, showing normal glomerular and tubular architecture. C, D: 15 Gy single-dose irradiated rat kidney at 8 weeks, showing focal fusion foot processes of podocytes (arrowheads) and vacuolization of the cytoplasm (asteriks), expansion in basal infoldings (curve arrows), swelling of epithelial cell and partial loss of luminal brush border (white arrow) in tubule cells. G, H: At 24 weeks postirradiation, kidney showing glomerular capillary wall thickening with subendothelial expansion (arrow), endothelial cell edema (E) and collapse of capillary loops (C) and tubular atrophy with thickening basement membrane (white arrowhead). E, F, J, K: Amifostine-pretreated rat kidney at the relevant time point, showing markedly improvement in tubular and glomerular ultrastructural lesions. Uranyl acetate and lead citrate. Scale bar: 1 μm.
In this study, glomerular histological changes after local kidney irradiation were characterised by glomerular tuft capsular adhesion, expansion of matrix in glomeruli, and thickening of the basement membrane Bowman's capsule. Previous studies indicated that glomerular tuft to capsule adhesions occurred in a rat model of experimental radiation nephropathy (19-20) as in the current results. By 24 weeks post-irradiation, the glomerular lesions were advanced and were associated with focal mesangiolysis and segmental sclerosis. Pretreatment with amifostine clearly reduced the sclerotic changes due to extracellular matrix (ECM) accumulation or capillary wall thickening in the glomeruli. Glomeru-losclerosis, the process by which glomerular tissue is replaced by ECM, is the final common pathway for loss of functioning glomeruli. It has been reported that irradiated glomeruli show lesions that include variable capillary loop thickening with subendothelial expansion and basement membrane thickening (19-20). The mesangium shows lysis of cells and matrix in continuity with the expanded subendothelial space: capillary loop collapse and mesangial sclerosis eventually develop. These various lesions may affect either a portion of the glomerular tuft or the entire glomerular tuft (1). It has been reported that prominent mesangial and endothelial alterations are observed consistently in radiation nephropathy, however, the podocytes appear less affected (1, 19, 21), as in the current results.
Although some investigators propose predominant glomerular damage associated with less severe tubular changes (22-23), others report that parenchymal cells, and in particular tubular epithelium, represent the primary target of radiation injury (11-12, 24). Robbins and Bonsib (1) reported that this disagreement was due to to differences in the doses of radiation used, physiological status of the kidney at the time of radiation, the amount of kidney exposed, and the interval from radiation to morphologic evaluation. Kaldir et al. (11) and Caloglu et al. (12) reported that widespread tubular injury (dilatation, loss of brush border, and atrophy) and diffuse interstitial fibrosis were seen in the absence of any specific glomerular pathology in unilaterally irradiated rat kidney, in contrast to the findings of the current study. The reason for this lack of glomerular response was probably the low dose rates used in these studies (9 and 6 Gy as a single dose) compared with the current study.
Tubular interstitial injury is an additional feature of radiation nephropathy. In advanced stages of radiation injury, tubular atrophy develops, characterised by small tubular cells enveloped by a thick, irregular basement membrane. A distinctive form of tubular injury develops in mice and rats; which is termed ‘tubulolysis’, and is characterized by apparent lysis of tubular cells, leaving an empty or denuded profile of tubular basement membrane (1, 25). In the present study, renal irradiation caused some tubular changes, such as ballon-like cellular degeneration, cytoplasmic vacuolization and loss of luminal brush border. However, tubular atrophy was observed in the absence of tubulolysis 24 weeks after irradiation. These data are corroborated by previous studies which used a rat model of radiation nephropathy in unilaterally irradiated kidney (11-12, 24). In the current study, pretreatment with amifostine markedly decreased in the severity of tubular changes in irradiated rat kidney, similar to the findings of earlier studies (11-12).
One of the most important limiting factors for radiotherapy is the occurrence of normal tissue injury with collagen deposition and fibrosis of tissues with loss of function (19). The resultant fibrosis is thought to occur because of excessive synthesis of ECM and a concomitant decrease in its degradation. In vitro irradiation of rat mesangial cells and/or tubule epithelial cells leads to marked changes in the expression of gene products involved in both matrix degradation and synthesis (26-27). After irradiation of a single hypertrophied kidney, Robbins et al. (24) observed time- and dose-dependent increases in interstitial staining for α -smooth muscle actin (α-SMA), collagen III, and fibronectin, as well as in tubular cytokine transforming growth factor β (TGFβ) staining. Cellular mechanisms of fibrosis also involve activation of fibroblasts into myofibroblasts, contractile fibroblasts that express α-SMA and are the main source of increased ECM deposition seen in renal fibrosis and, indeed, in other forms of tissue fibrosis (28). In previous studies, radiation-induced activation of interstitial myofibroblasts with resultant collagen deposition has been reported in rat kidney (19, 29). The results of the present study demonstrated that unilateral kidney irradiation of 15 Gy as a single dose induced interstitial fibrosis with inflammatory cell infiltrate in rat kidney. The most significant fibrotic lesions occur at 24 weeks after irradiation, as shown in several studies (11-12). Increased numbers of mononuclear leukocytes have been demonstrated in different species as a result of local renal irradiation or total-body irradiation in studies used of higher doses radiation, similar to that in present study (1, 23). Detailed mechanistic studies suggest a causative role of oxidative stress in fibrogenesis after irradiation (30). Antioxidants have clearly proven to be effective both in terms of inhibiting and in reversing established fibrosis (31-32). This study showed that amifostine, free radical scavengers or antioxidants, effectively decreased irradiation-induced fibrotic lesisons in rat kidney, in agreement with previous studies (11-12)
There have been only a few previous studies to support the protective effect of amifostine in radiation nephrotoxicity (11-12, 33-34). In recent studies, this nephroprotective effect has found to be different. Kaldir et al. (11) indicated that amifostine had a significant protective effect on kidney function in irradiated rat. However, Caloglu et al. (12) reported that amifostine protected the kidneys against radiation-induced late toxicity not only functionally, but also histopathologically. In this study, electron microscopic analysis demonstrated that amifostine pretreatment preserved ultrastructure of kidney against acute and late radiation nephrotoxicity in rats.
To the Authors' knowledge, the present study is the first ultrastructural investigation concerning the protective effect of amifostine in irradiated rat kidney. The current results clearly establish that amifostine inhibits tubular changes, interstitial leukocyte infiltration and improves glomerulosclerosis and interstitial fibrosis in irradiated rat kidneys. In conclusion, in vivo administration of amifostine prior to radiotherapy may contribute to prevention of radiation-induced acute and late nephrotoxicity.
Acknowledgements
The Authors would like to thank to Dr. Fatma Nesrin TURAN for statistical analysis.
- Received October 11, 2010.
- Revision received November 10, 2010.
- Accepted November 12, 2010.
- Copyright © 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.