


Abstract
Background: Apoptosis and cell proliferation in patients with adenocarcinoma of the lung have not been well described with relation to fine-needle aspiration biopsies (FNABs). To investigate the contribution of apoptosis to the growth of adenocarcinoma of the lung, both apoptosis and cell proliferation were analysed for correlation with the grade of the tumor. Patients and Methods: Fifty tumors from 50 patients with adenocarcinoma of the lung were studied. Twelve tumors were well-differentiated, 22 were moderately differentiated and 16 were poorly differentiated. The detection of DNA fragments in situ using the terminal deoxyribonucleotidyl transferase – mediated dUTP–digoxigenin nick-end labeling (TUNEL) assay was applied to investigate active cell death (apoptosis) and the MIB-1 antigen was used to investigate cell proliferation. Results: The TUNEL indices were 0.55±0.09, 0.90±0.33 and 3.1±0.99 in well-, moderately and poorly differentiated adenocarcinoma of the lung respectively. The MIB-1 antigen labeling indices were 7.1±0.12, 14.3±3.5 and 28.7±6.9, respectively, in the same order of tumor differentiation. The differences in both TUNEL and MIB-1 labeling indices were significant between well-, moderately and poorly differentiated adenocarcinoma of the lung and a positive correlation was found between the TUNEL indices and the MIB-1 indices. Conclusion: Apoptosis (cell death) and cell proliferation increases as the grade of differentiation decreases in adenocarcinoma of the lung, suggesting a rapid turn over of the tumor cells in tumors with a lower grade of differentiation.
Adenocarcinoma (AC) of the lung is a malignant tumor with poor prognosis. To improve the prognosis, it is important to establish biological markers, other than tumor, node, and metastasis factors, that determine prognosis and response toward a particular treatment (1).
Apoptosis, a mode of cell death clearly distinct from necrosis, is a physiological phenomenon that occurs spontaneously in the process of normal tissue growth (2). Apoptosis has also been shown to be closely associated with malignant tumors and abnormality in the process of apoptosis promotes malignant transformation and leads to tumor proliferation. The balance between apoptosis and cell proliferation may play an important role in carcinogenesis. Most of the previously reported results suggest that apoptosis is a form of cell death as a secondary result of active cell division and proliferation (3).
It is particularly important when discussing tumor progression to consider balance of both cell death and cell proliferation because an argument based on only one of these factors may lead to an incorrect or confusing conclusion. Nevertheless, attention has been focused in preceding investigations exclusively on whether the fraction of either apoptotic or proliferating cells is high or low in a particular malignant tissue.
In the present study, we conducted a detailed investigation on the balance of apoptosis and cell proliferation on fine-needle aspiration biopsy (FNABs) in patients with lung AC correlated with tumor grade in order to demonstrate that apoptosis and cell proliferation have a biologic significance as prognostic factors.
Patients and Methods
Fifty (50) patients (38 males and 12 females; median age 57 years) with operable lung AC were diagnosed and studied cytologically using FNABs and had their diagnoses confirmed histologically after the operation of these tumors. Twelve (12) tumors were well-differentiated, twenty-two (22) were moderately differentiated and sixteen (16) were poorly differentiated. For the cytologic diagnosis of the lung AC, the specimens from FNABs were stained using Papanicolaou and Giemsa stains.
Statistical analysis between TUNEL and MIB-1 (Ki-67) according to the grade of lung adenocarcinoma.
In situ detection of DNA fragmentation. In this study, DNA fragmentation was assessed using terminal digoxigenin-labeled dUTP nick-end labeling (TUNEL), a method that is based on the specific binding of O-TdT to the 3′-OH ends of DNA, ensuring the synthesis of a polydeoxynucleotide polymer. For this purpose, the In Situ Cell Death Dedection Kit (AP; Boehringer Mannheim, Indianapolis, IN USA) was used. The air-dried specimens were fixed with a freshly prepared paraformaldehyde solution 4% in phosphate-buffered saline (PBS) (pH 7.4) for 30 minutes at room temperature. The slides were then rinsed with PBS and incubated in permeabilization solution (0.1% Trion X-100 and 0.1% sodium citrate) for 2 minutes on ice at 4°C. The slides were rinsed again twice with PBS, the area around the specimens was dried, and 50 μl terminal digoxigenin-labeled dUTP were applied to the specimens, followed by incubation in a humidified chamber for 60 minutes at 37°C. The slides were then rinsed three times with PBS, dried, and 50 μl converter AP from the detection kit were applied to the specimens, followed by incubation in a humidified chamber for 30 minutes at 37°C. The slides were then rinsed three times with PBS, washed in 50-100 μl substrate solution, incubated for 10 minutes at room temperature, and rinsed three more times in PBS. Finally, the slides were mounted under glass coverslips (with PBS and glycerol) and analyzed under a light microscope. A very light hematoxylin counterstain was performed before counting, and, for a positive control, a tissue sample from a normal lymph node was used. Apoptotic cells were counted in ×40 high-power fields (HPFs), and the number was averaged in 10 consecutive HPFs.
Immunohistochemistry was performed on air dried specimens using the alkaline phosphatase (APAAP) method. To estimate cell proliferation, MIB-1 monoclonal antibody (DACO, Carpinteria, CA, USA) was used, at an optimal dilution of 1:10 with 1 hour incubation in a microwave oven at 750 W for 3 cycles, and a very light hematoxylin counterstain was performed before counting. Normal lymph node was used as a positive control for MIB-1.Ten HPFs (500 cells at least) were examined in each case using a ×400 magnification. MIB-1 nuclear expression was considered as a positive observation. For statistical analysis, Student's t-test was used.
Results
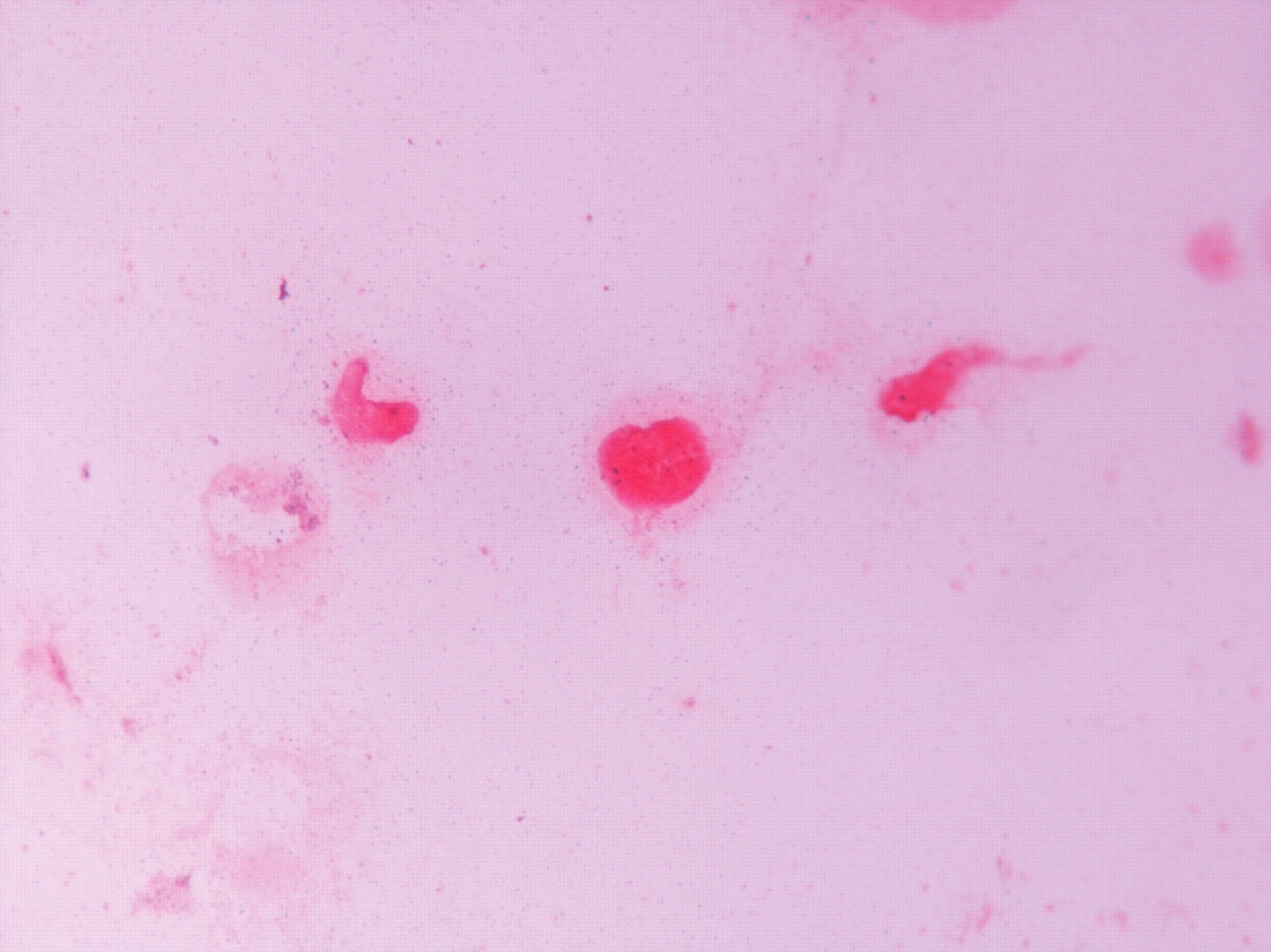
TUNEL staining was observed only in the nuclei as apoptotic bodies and under light microscopy. The cells displayed the characteristic features of apoptosis, exhibiting cell shrinkage, nuclear chromatin condensation and included membrane-bound fragments, known as apoptotic bodies (Figure 1). The TUNEL-positive lung AC cells were generally scattered and individual positive cells were sometimes clustered in well-differentiated and moderately differentiated tumors, but not in poorly differentiated ones.
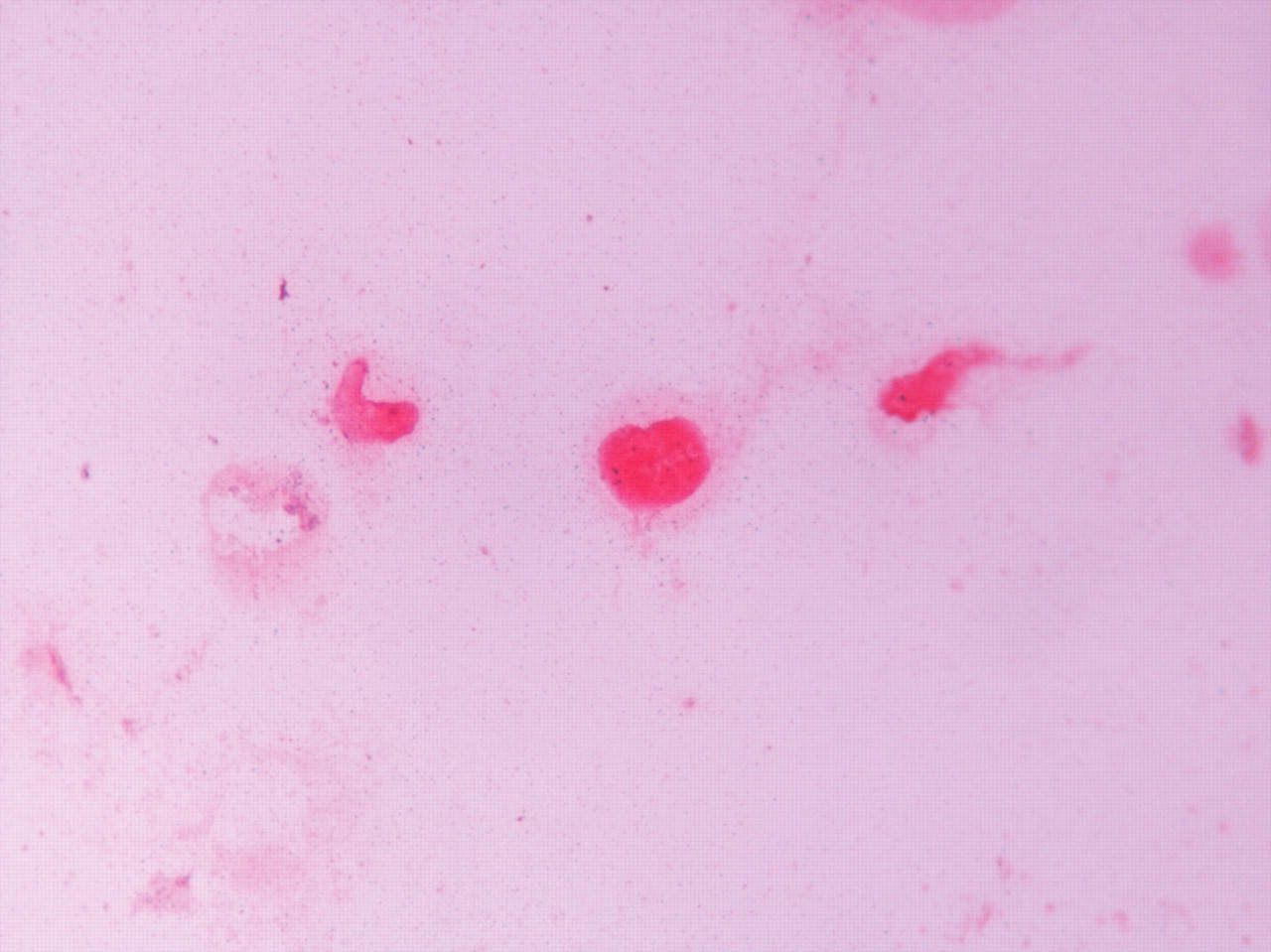
MIB-1 nuclear-positive lung AC cells (Figure 2) were also randomly and heterogeneously distributed. MIB-1 expression was significantly greater compared with TUNEL expression in all tumors. Although TUNEL-positive cells were not necessarily localized in areas that contained many MIB-1-positive cells, there was a positive correlation between TUNEL expression and MIB-1 expression (p<0.001).
High values for TUNEL expression and MIB-1 expression were seen in moderately and poorly differentiated lung AC cells and were 0.90±0.33, 3.1±0.99, 14.3±3.5 and 28.7±6.9 (means±standard deviation), respectively, and both were significantly higher (p<0.001) compared with the values in well-differentiated lung AC (0.55±0.09 and 7.1±0.12 respectively). There were also significant differences between moderately differentiated lung AC and poorly differentiated lung AC for both TUNEL and MIB-1 expression (p<0.05 and p<0.01 respectively) (statistical analysis by Student's t-test), (Table I).
Discussion
The significance of apoptosis and cell proliferation in cancer as biological markers, and especially as prognostic factors, has not been established. Many previous investigations conducted on this subject yielded contradictory results; some reports demonstrated that high apoptosis led to poor prognosis, some reported high apoptosis led to good prognosis and others demonstrated that apoptosis was not related to prognosis.
Apoptosis is reported to occur more frequently in colorectal adenomas with severe dysplasia (containing cells proliferating more rapidly) compared to those with mild dysplasia (4). Apoptotic cells are observed more frequently in undifferentiated carcinomas (where cells are proliferating more actively) than in differentiated tumors.
In the current study, application of the TUNEL method on FNABs specimens from patients with lung AC showed that apoptosis occurred more frequently in tumors with lower differentiation compared with the apoptosis found in well-differentiated tumors, a result that is in accord with the above results. There is another reported study on histological material which indicates that peripheral small-sized invasive lung AC with low apoptosis (low AI) carry an increased risk of distant metastasis (5).

Apoptotic bodies (TUNEL) in lung adenocarcinoma cells, ×250.
Another recent study suggests that progression of lung carcinomas correlates with the increase in tumor volume, which is accompanied by an increase in apoptosis rather than an increase in cell proliferation (6).
Furthermore, we found a positive correlation between TUNEL expression and MIB-1 expression. Moderately and poorly differentiated lung adenocarcinomas had a higher proliferation rate than highly differentiated and frequent incidence of apoptosis. However, the tumor cell proliferation rate in lung AC is always higher than the rate of apoptosis. Our results are consistent with the results of previous studies on apoptosis and cell proliferation in various tumors, as gastric carcinomas, prostatic carcinomas and non-Hodgkin's lymphomas, which demonstrated that the higher tumor malignancy is related to more active cell proliferation, as well as the higher proportion of apoptotic cells, implying that the observed increase in the number of apoptotic cells reflects the higher activities of cell division and metastasis (7-21).
In conclusion, we were able to use cytological specimens (FNABs) to study the role of cell proliferation and apoptosis in patients with lung AC. Our results show that tumors with higher rates of proliferative activity and apoptosis have a higher degree of biological aggressiveness and indicate a higher risk of distant metastasis and poorer prognosis.
MIB-1 nuclear expression in lung adenocarcinoma cells, ×250.
- Received March 26, 2010.
- Revision received July 7, 2010.
- Accepted July 14, 2010.
- Copyright © 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}