


Abstract
Introduction: Peritoneal carcinomatosis (PC) is one of the routes of dissemination of abdominal neoplasms and is generally considered a lethal disease, with a poor prognosis by conventional chemotherapeutic treatments. While systemic chemotherapy has little impact on the treatment of peritoneal disease, some centers have reported encouraging results with cytoreduction and hyperthermic intraperitoneal chemotherapy (HIPEC). This approach is based on surgical cytoreduction of the primary tumour, peritonectomy (stripping of implants on the peritoneal surface) and HIPEC. The rationale of this treatment, after macroscopic disease removal, is to obtain an elevated and persistent drug concentration in the peritoneal cavity, with limited systemic effects. Many studies have reported encouraging results on overall survival (OS) and the disease-free interval in patients affected by PC. Patients and Methods: From October 1997 to November 2008, 411 operations for PC were performed in our institution; in 232 cases, cytoreduction plus HIPEC was carried out. Out of 72 operations for colonic cancer: 40 cytoreductions plus HIPEC, 12 cytoreductions+ EPIC (early postoperative intraperitoneal chemotherapy) and 16 debulking or explorative laparoscopies/laparotomies were performed. For the present study, the 40 patients who had undergone cytoreduction plus HIPEC for PC of colorectal cancer (CRC) were considered. Results: The complication rate was 55% (22/40) and mortality rate 2.5% (1/40). The specific features of both groups were considered for the survival curves and complication rates, with special reference to the peritoneal carcinomatosis index (PCI; range 0, absence of disease to 39) and completeness of cytoreduction score (CCR; 0, no residual tumor, to CCR 3, residual nodules greater than 25 mm). In Group A, patients operated on prior to 2002, the median survival time was 16.7 months compared to 24.6 months for Group B, those operated on after 2002. The poor survival of Group A seemed to be related to higher PCI and CCR scores. Conclusion: Correct patient selection based on a maximum PCI of 16, associated with complete cytoreduction (CCR-0), produced encouraging results in our experience. To improve this encouraging survival outcome, it is very important to unify the surgical experience of expertise centres. Our results also suggest the need for an integrated approach to this condition to identify the correct aspect of the surgical domain and results that may be influencing the prognosis and the evolution of this patients.
Peritoneal carcinomatosis (PC) of colorectal cancer (CRC) origin has been considered as a systemic disease and treated by systemic chemotherapy, often associated with palliative surgical operations. This approach has usually not significantly influenced the natural history of the disease which is characterized by poor prognosis with median survival ranging between 6 and 8 months (1). Modern systemic chemotherapy regimens with oxaliplatin or irinotecan in eventual association with biological agents, such as angiogenesis inhibitors, have improved survival rates; in some series the median survival reached 18-20 months. Some better results by systemic chemotherapy are reported by using new drugs, alone or in association with angiogenesis inhibitors but the reported overall survival (OS) is rarely higher than 18 months (1-8).
In the 1980s, a multimodal technique was developed to manage PC, based on surgical cytoreduction of the primary tumour, peritonectomy (stripping of implants on the peritoneal surface) and hyperthermic antiblastic peritoneal perfusion (HIPEC). Many studies reported an impact on OS and disease free-survival (DFS) in patients affected by PC from CRC (1, 2, 4, 5, 8-10). The combination of hyperthermia and locoregional chemotherapy has antineoplastic effects because the peritoneal cavity can be considered a pharmacological sanctuary due to the peritoneal plasma barrier. This barrier prevents leakage into the systemic circulation of high molecular weight drugs, providing dose-intensive therapy. Hyperthermia increases drug penetration into the tissues and the cytotoxicity of selected drugs (11-13).
In the semi-closed HIPEC technique (11-14) performed at our institution, the abdominal wall is partially closed and hung onto an autostatic retractor, with only the central part of the wound remaining open. Through this opening, the surgeon can mix the perfusate solution and examine the peritoneal cavity. This allows both the homogeneous distribution of temperature and drugs, and represents a low risk of drug leakage from the abdominal cavity.
In this study, preliminary results with this approach in 40 patients affected by PC from CRC are reported. These patients were treated by cytoreductive surgery and the semi-closed HIPEC technique, with special regard to postoperative complications and the survival impact of the peritoneal carcinomatosis index (PCI) and completeness of cytoreduction (CCR score) (13-15).
Patients and Methods
From a database of 411 operations for PC of varied origin (232 cases treated with surgical cytoreduction plus HIPEC), 72 patients affected by PC of CRC origin were extracted: of these, 40 had undergone cytoreduction plus HIPEC; 12 cytoreduction plus EPIC (early postoperative intraperitoneal chemotherapy) and 16 debulking or explorative operations. For the present study, the 40 patients who had undergone cytoreduction plus HIPEC were considered. The data were analyzed dividing the patients into two groups: the first group (Group A) comprising the patients operated on up to 2002 (23/40) and the second group (Group B) patients operated on from 2002 to 2008 (17/40). The preoperative evaluation always included thoracic and abdominal CT scan to stage the peritoneal disease and exclude distant metastases; upper digestive endoscopy and colonoscopy generally completed the tumor staging. A careful preoperative evaluation of the patient's general condition was always performed and included complete blood tests, electrocardiogram, cardiac ultrasound and spirometry. The presence of non-resectable hepatic metastases or extra-abdominal disease, massive ileum involvement and age over 70 years were considered exclusion criteria. Informed consent was obtained from all the patients.
Immediately after laparotomy, a complete intraoperative staging of the peritoneal disease was performed using the PCI that range from 0 to 39, where 0 means absence of disease (13-15).
The CCR was also classified according to Sugarbaker's criteria (1) as: CCR0 (no residual tumor); CCR1 (no residual nodules greater than 2.5 mm in diameter); CCR2 (no residual nodules greater than 25 mm) and CCR3 (residual nodules greater than 25 mm).
Patient features. The median age was 51.9 years (range: 19-70), 24 were male (60%) and 16 female (40%). The primitive cancer arose from the left colon and rectum in 26 cases (65%), from the right colon in 12 cases (30%), from the transverse colon in 2 (5%). For all the patients histology was colonic adenocarcinoma; 15 patients (37.5%) presented the histological feature of signet-ring cell. Thirty-six patient (90%) had undergone previous surgical procedures (8 diagnostic laparoscopy or laparotomy, 28 bowel resection or debulking operations). Twenty-two patients (55%) had received systemic chemotherapy before the HIPEC operation. Four patients (10%) had bowel obstruction before the operation. The overall median PCI was 13.4.
Surgical technique. The peritonectomy procedure was performed according to the Sugarbaker criteria: central peritonectomy; left upper quadrant peritonectomy; right upper quadrant peritonectomy; lesser omentum peritonectomy; pelvic peritonectomy with en bloc removal of pelvic peritoneum, sigmoid colon, rectum, uterus and salpingo-oophorectomy and peritonectomy of the lateral abdominal wall. Implants on the visceral serosa were removed by electrosurgical local dissection, the peritonectomies were variously combined with resections of the viscera with tumor involvement. A variable number of visceral resections (bowel, greater omentum, hystero-oophorectomy, cholecystectomy, spleen resection) were combined with multiple peritonectomies: in 6 (15%) cases to peritoneal area 3 (P1), in 15 (37.5%) cases from peritoneal area 3 to 6 (P2), in 10 (25%) from 6 to 9 area (P3) and finally in 9 patients (22.5%) from 9 to 12 (P4).
One bowel anastomosis was performed in 22 patients (55%), 2 bowel anastomoses in 11 patients (27.5%) and in 7 patients no bowel anastomosis was performed (17.5%). In 23 (57.5%) cases the anastomosis was protected with lateral temporary ileostomy, while in 5 cases, a definitive colostomy was performed.
HIPEC technique. The HIPEC was performed according to the original semi-closed abdomen technique (11-14) with 5 drain tubes placed in the abdominal cavity, the two y-shaped inflow tubes presenting multiple openings. The drugs used were: cisplatinum (CDDP) 100 mg/m2 plus mitomicin-C (MMC) 16 mg/m2 at a temperature of 41.5°C or oxaliplatinum 460 mg/m2+5-fluorouracil intravenous administration (12) at 42°C for 30 min or MMC 35 mg/m2 for 60 min at a temperature of 40.5°C, according to the Netherlands protocol (1), if the patient presented intolerance to platinum compounds. The mean duration of surgery (including HIPEC) was 10.3 hours (range 6-14). At the end of the operation, the patients were admitted to the intensive care unit and then returned to the surgical department when cardiovascular and pulmonary functions became normal.
Group A (23 patients) had a median PCI of 15.4 (49% of the patients had a PCI higher than 16) and the CCR score was 2 for 9 patients. All these patients were treated with a protocol based on administration of CDDP 100 mg/m2 plus MMC 16 mg/m2 for 60 min, with a peritoneal temperature of 41.5°C. Due to preliminary experience with Group A, Group B (17 patients) patients were selected with a PCI≤16. The median PCI was 10.7 (only one patient had a PCI=16), the CCR score was 0 (no residual disease) for all the patients. Eleven of the patients were treated following the protocol of Elias et al. (9) combining administration of folinic acid at 20 mg/m2 plus 5-fluorouracil 400 mg/m2 intravenous associated with peritoneal administration of oxaliplatinum 460 mg/m2 for 30 min with a peritoneal temperature of 42°C (one patient in Group A and 10 patients of Group B).

Cumulative survival of all patients.
Statistical analysis. The statistical analyses focused on the postoperative complications using the clinical and follow-up data stored in the database. The presence of postoperative complications was considered according to gender, operative time, number of anastomoses, operation period, previous chemotherapy done vs. not done, extent of peritonectomy, PCI and CCR. The univariate analysis of the factors was performed by the Chi-square test. OS was dated from the day of surgery to the time of death due to any cause. The survival curves for OS were calculated according to the Kaplan-Meier method: a p-value <0.05 was considered significant. XLSTAT (Version 2009.4.03 Addinsoft New York 10013, USA) was used for statistical analysis.
Results
The overall morbidity rate was 55% (22/40) and the mortality rate 2.5% (1/40). The surgical complications associated with multiple complications were: wound infection in 5 cases, intestinal/biliary fistula in 4, abdominal abscess in 3, prolonged ileus in 1, bleeding in 1 and multiple organ failure in 1 patient who subsequently did. The medical complications were: 6 cases of hematological toxicity, 2 of arrhythmia, 9 of pleural effusion and 1 cutaneous rash. In 5 cases (23%) re-intervention was necessary (3 for bowel perforations, 1 for hemorrage, 1 for biliary fistula).
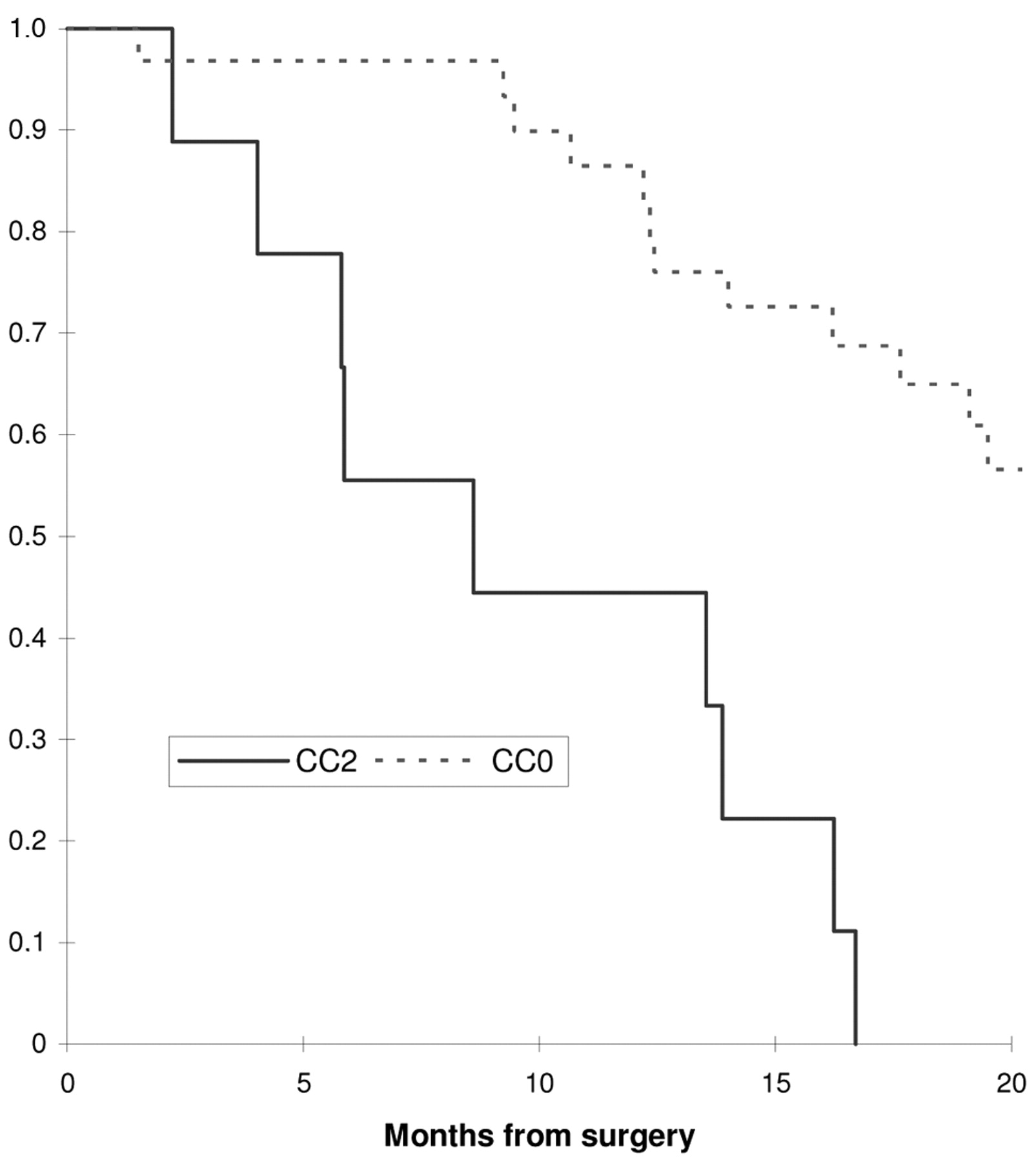
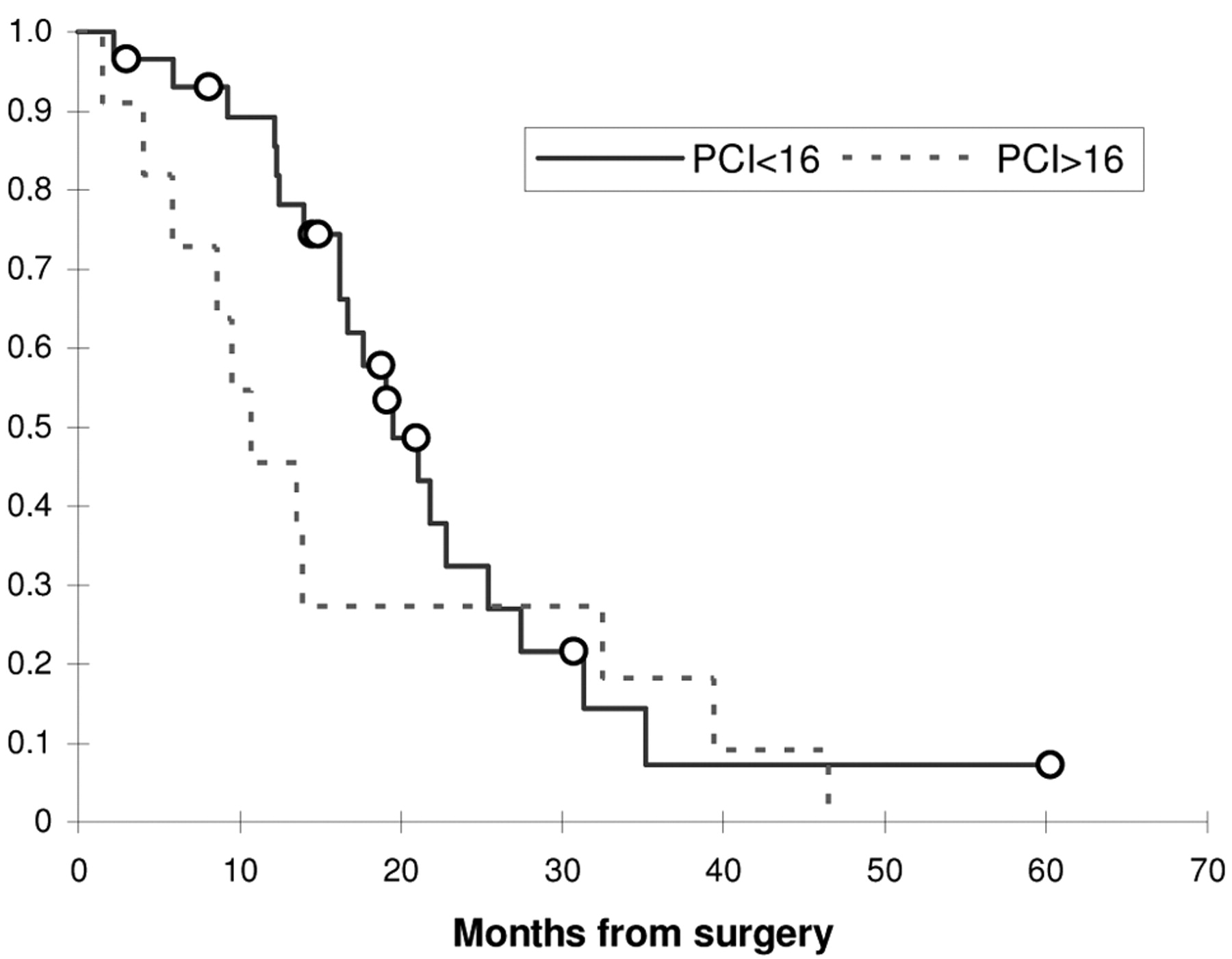
The OS of our database was 43 months (Figure 1): in Group A, the results were not very satisfactory, with a median survival time of 16.6 months, lower than expected, compared to 24.6 months in Group B (Figure 2). In the CCR0 patients (31), we found a mean survival time of 24 months compared to 9.7 months of CCR2 (9) patients; in fact, the CCR (CCR0 vs. CCR2 p<0.0001) was strictly related to OS (Figure 3). On the contrary, in our experience, PCI had no influence on OS (PCI>16 vs. PCI<16 p<0.290) (Figure 4).

Overall survival according to Group A and Group B (p<0.019).

Overall survival according to the completness of cytoreduction score (CCR) (p<0.0001).
The association between morbidity and the clinical variables was also evaluated (Table I) and only the different operative time between the two groups was associated with a higher incidence of postoperative complications. This particular aspect is likely linked to the learning curve of this surgical procedure and would confirm this as one of the most important aspects of this treatment and its feasibility only in a specialized center with long surgical experience. In fact, only in Group A was the high complication rate statistically confirmed if compared with Group B.

Overall survival according to the peritoneal cancer index (PCI) of all patients (p<0.290).
Discussion
In a phase III study of cytoreduction plus HIPEC with MMC reported by the Netherlands Cancer Center Institute (1), the patients with PC from CRC were preoperatively randomly assigned to standard treatment with palliative surgery followed by systemic fluorouracil and leucovorin, or to treatment with maximal cytoreductive surgery with HIPEC. After a mean follow-up of 24 months, the 2-year survival rates were 43% in the experimental group and 16% in the standard group. The study was stopped for ethical reasons.
A study by Glehen et al. (2), including a large population of 506 patients, showed interesting survival results using the combination of cytoreductive surgery and HIPEC for the treatment of PC from CRC. The median survival time was 19.2 months and the 3- and 5-year survival rates were 39% and 19%, respectively. Elias et al. (9), reported a median survival of 32.4 months, and a 5-year survival rate of 48% in patients affected by PC from CRC treated with cytoreduction plus HIPEC. These data support the idea that surgical removal of PC associated with HIPEC may change the natural history of PC.
Cytoreduction, peritonectomy and HIPEC were characterized, in all series, by high morbidity rate. In the present study, the overall morbidity rate was 55% (22/40) and the mortality rate 2.5% (1/40); these rates are similar to those reported in literature by the most experienced centers. In literature, the main morbidities associated with HIPEC combined with cytoreductive surgery are often caused by complications of surgery. The results of three multivariate analyses have shown that the independent factors of morbidity were the duration of surgery, the number of anastomoses, the extent of carcinomatosis (PCI) and the CCR score (16-18). The most dangerous surgical complication of this treatment is intestinal fistula, with a generic incidence ranging from 4% to 28%. This complication often determines the reoperative rate, as confirmed in our experience. To reduce the incidence of intestinal fistulas, we often protect the anastomoses by an ileostomy and perform a jejunostomy for early enteral nutrition. The extent and stage of the carcinomatosis has also been reported as an important predictive factor of morbidity. The medical complication related to the main morbidity from HIPEC is that of hematological toxic effects, reported in 8-31% of patients. Renal toxicity, when HIPEC is delivered with platinum compounds, has also been reported: in our experience this problem was resolved by hyperhydration and forced urination by furosemide continuous infusion during HIPEC, associated with Amifostine® administration. The high treatment morbidity rate, even if associated with an acceptable mortality rate, suggests that the strict selection of patients is necessary.
PCI, Peritoneal cancer index; CCR, completeness of cytoreduction score. Association between clinical variables and complications in 40 cases of peritoneal, carcinomatosis from colon cancer treated with HIPEC.
The PCI and CCR score are strictly related to the complications rate and OS in the world literature (1, 2, 9, 16, 17).
The PCI is directly related to the required aggressiveness of surgery and then to the morbidity rate and the patient's outcome. The CCR score is also related to patient's outcome (2, 9). Fewer complications and a higher survival rate are achieved in patients with no residual disease at the end of cytoreduction (1, 2, 9).
In the present study, in Group A the median PCI was 15.4 (49% of the patients had a PCI higher than 16) and the CCR score was 2 for 8 patients, meaning an incomplete cytoreduction, indicating a large diffusion of carcinomatosis, requiring aggressive visceral resections, linked to a high postoperative complication rate. The observations from our early experience, together with data from the literature (9, 16-18) suggested the option of making a better selection of the patients and treating only the patients with a maximum PCI index of 16, in which was possible to reach a CCR0 cytoreduction. For these reasons, the last 17 patients (Group B) were selected with those criteria. The first 10 patients were treated by protocol of Elias et al. (9) (later abandoned due to budget limitations), the other 7 by CDDP plus MMC. The median PCI was 10.7 and complete cytoreduction (CCR0) was achieved in all the patients. In this selected group, the median survival then climbed to 24 months. The uniformity of the clinical response in Group B patients suggested that the type of drug used did not significantly influence the results. We believe there is a relationship between the PCI index and the incidence of complications from our experience; it is possible although we have not yet found it such a relationship probably due to the small number of cases resulting in the data having no statistical significance. But the better patient outcome in Group B, in our opinion, also seems to be related to the selection criteria for this group (no other variables were changed in patient selection between Group A and Group B), specifically to patients with PCI<16 and those in whom it was simpler to obtain a CCR0. The aim of a new study, now in progress, is to evaluate if other variables were involved in the better survival of Group B (previous chemotherapy, tumor differentiation/mucinous type, relationship between complications and prognosis, gender, EGFR expression).
PC is usually detected late in disease progression because symptoms occur at an advanced stage and current imaging is unable to detect PC at an early stage. Elias et al. (19) analyzed the impact of second-look surgery in an attempt to treat PC at an early stage in a series of patients at high risk of developing carcinomatosis from CRC. High-risk patients (resected minimal synchronous macroscopic disease, synchronous ovarian metastasis, perforated primary tumor) were treated by second-look surgery and HIPEC 12 months after the resection of their primary tumor. PC was found in approximately 55% of the patients and preliminary results at follow-up at 27 months seem to be encouraging. This evidence may suggest a future method of addressing the treatment of PC from CRC: the literature data and our experience suggest that advanced carcinomatosis, with a higher possibility of incomplete cytoreduction due to disease diffusion is linked to a higher complications rate and worse prognosis. In selected high-risk patients, second-look surgery plus HIPEC should allow the treatment of patients with minimal peritoneal disease, wich may result in a low complication rate and effective improvement of the survival rate.
Conclusion
Complete cytoreduction associated with HIPEC shows encouraging results for OS in the treatment of PC from colonic cancer compare to systemic chemotherapy. Lower complication rates and better patients outcome are achieved in patients with low peritoneal diffusion of disease and complete cytoreduction, confirming other reported findings. In the future, correct patient selection (PCI<16 and optimally cytoreductable) and programmed second-look surgery in high-risk patients may change the approach to this disease and lead to lower complication rates, this representing the cornerstone for real improvement in disease-free and OS. Moreover, these results should be confirmed by randomized trials able to analyze the effective impact of this technique in OS compared to the standard therapy with multidrug systemic chemotherapy.
Footnotes
- Received July 11, 2009.
- Revision received November 24, 2009.
- Accepted November 27, 2009.
- Copyright © 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Outcomes for Colorectal Cancer Cases With Peritoneal Metastases Treated With Cytoreductive Surgery With or Without Hyperthermic Intraperitoneal Chemotherapy: A Comparative Analysis of Survival Between Peritoneal Carcinomatosis Scores - PCI in a Single Centre
- DDR2 Expression Is Associated with a High Frequency of Peritoneal Dissemination and Poor Prognosis in Colorectal Cancer