


Abstract
This report describes the clinical course of a female who developed an osteoma of the orbital floor. Initially, the patient noticed a pain in the left periorbital region, in particular in the region of the lower eyelid and the upper cheek. A radiograph of the midfacial region was taken that depicted a mushroom-like tumor of the orbital floor. The tumor was surgically removed. The follow-up over a period of 13 years revealed no recurrence of the osteoma.
Osteomas are benign tumors of the bone (1). In the skull, the paranasal sinuses, the jaws and the calvaria are predominantly affected (2). The incidence of skull osteoma is supposed to be less than 0.4%, as judged following retrospective analysis of skull radiographs (3, 4). It is understood that in most cases of orbital osteoma that the cavity is secondarily affected due to ingrowth of osteomas arising in adjacent structures, predominantly the paranasal sinuses (1). The differentiation of primary and secondary orbital osteoma is prudent in terms of surgical treatment planning and outcome assessment (1). The frequency of osteomas arising in the paranasal sinuses declines from the frontal sinus, the ethmoids and the maxillary sinus to the sphenoid sinus (2). Series on orbital osteomas are scant and low in number (1, 5-7).
Physical findings and therapy in a case of osteoma of the paranasal sinuses are usually published as case reports (8-13). The maxilla is a rare origin of osteoma extending to the orbit (14-16). Extension of osteomas to the orbit may cause severe morbidity, such as atrophy of optical nerve, ophthalmoplegia, cephalgia or papillitis (17), or abscess (18).
This report deals with a case of orbital osteoma that became symptomatic with dysesthesia of the second trigeminal nerve and subjectively estimated impaired eye mobility and which was followed over a long period of time. The localization of the orbital region giving rise to the osteoma classifies the tumor as a primary orbital osteoma. The findings are similar to those of reports presented by Roth and Hun (19) and Miller et al. (20) and appear to be rare.
Case Report
Three months prior to the time of diagnosis, a 53-year-old female occasionally experienced an unspecific compression in the region of the left eye. About three weeks before admission to the hospital, she noticed a movement-dependent pain of the left eye. At no point in time did she develop diplopia. A reddening of the lids and a superior position of the left eye compared to the right was intermittently noted. The patient ascribed the pain to the left frontal and periorbital region. This condition prompted her physician to perform a cranial computed tomogram. The intracranial findings were inconspicuous. However, a bone dense stucture of about 1×1 cm2 was identified at the bottom of the orbit, restricted to the maxillary part of the cavity wall (Figure 1). The structure was located in the region of the distal border of the vitreous body and displaced both the oblique inferior and rectus inferior muscles to the cavity. The tomograms revealed the tumor arising strictly from the maxilla in a pedunculated pattern (mushroom-like) and solely growing into the orbit with no extension to the maxillary sinus. The tumor was in close proximity to the infraorbital fissure (Figure 2). The soft tissue covering the roof of the maxillary sinus appeared to be thickened.
Further physical investigations revealed a superior position of the left globe of about 2 mm. The patient experienced pain following sight in any direction. However, no objective limitation of ocular movement could be verified. Neither an exophthalmos nor any intraocular pathological findings were diagnosed. The patient specified a discrete paresthesia of the left ala of the nose and pain following pressure of the supra- and infraorbital foramina of the affected side, without any visible signs of inflammation.

Coronal computed tomogram of the left orbit. The tumor, isointense to bone, is situated on the orbital floor. The volume of the maxillary sinus is not reduced. There is no visible extension of the bony tumor into the maxillary sinus.
The anterior-posterior radiographs revealed a deviation of the nasal septum. The patient interpreted this finding in conjunction with a fall that happened in her early childhood. At that event a fracture of the zygoma had been postulated but was never properly diagnosed.
Surgical therapy was enforced via an infraorbital incision of the skin, periosteal incision at the infraorbital rim and consecutively subperiosteal separation of the soft tissues from the osseous tumor of the orbital floor. The infraorbital nerve proceeded on the top of the mushroom-like tumor and was displaced laterally with the elevated periosteum (Figure 3). Following this maneouver, the tumor was excised with a chisel (Figure 4). The infraorbital nerve, spontaneously huddled against the defect of the orbital floor, was reconstructed with Ethisorb™ (Codman Inc., Raynham, MA, USA). Healing was uneventful. Over the following weeks, the patient noticed a stepwise recovery from paresthesia of the left cheek. In order to rule out intestinal polyposis (Gardner's syndrome), a colonoscopy was performed (21-23). The colonoscopy revealed no pathological findings (24).
Thirteen years later the patient appeared for re-evaluation of the situs. She declared that sometimes an unspecified compression appeared in the left cheek, but there was no paresthesia. A plain radiograph of her left orbit excluded local recurrence of osteoma (Figure 5). The woman had no history of cancer during the follow-up period.

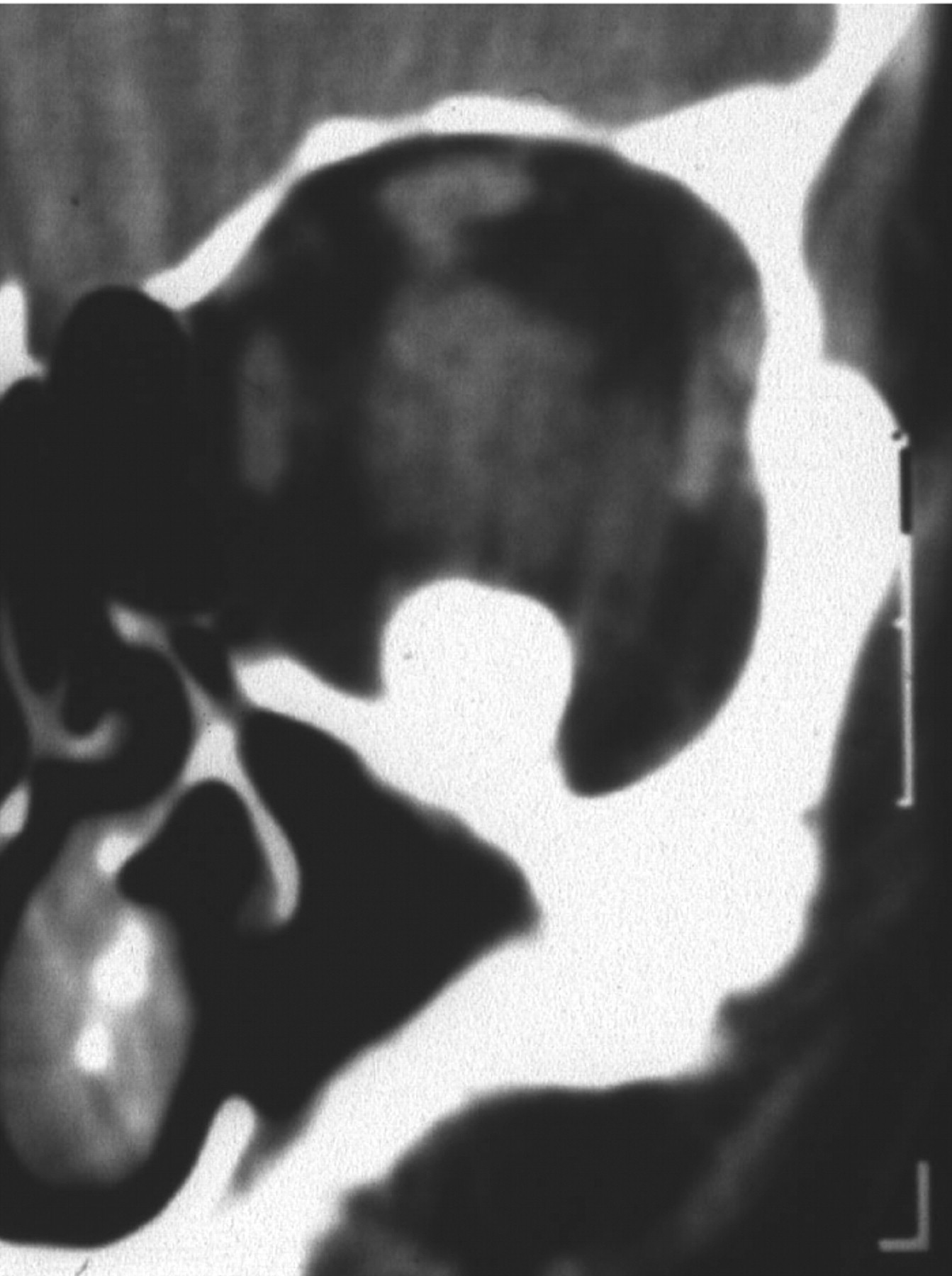
Hypocycloideal tomogram of the left orbit reveals the pedunculated osseous tumor close to the infraorbital fissure.
Discussion
Osteomas of the orbital floor are rare findings in this group of tumors and have only been occasionally reported (19, 20, 25, 26). Osteomas are the most frequent osseous neoplasms of the orbit (1). In a large survey on 740 tumors or tumor-like lesions, osteomas constituted 5.1% [n=38; (27)]. The histological differential diagnosis of osteoma and exostoses was probably more difficult in earlier times. Given this hypothesis, the current lower prevalence of osteoma in orbital tumors (<1%) is not considered to be due to a lower rate of tumors (1, 28).
Differential diagnosis of osteoma includes fibrous dysplasia, ossifying fibroma, benign osteoblastoma, giant cell granuloma and osteosarcoma (29, 30).
A characteristic finding in fibro-osseous lesions of the orbit is the secondary involvement of the orbital soft tissues following ingrowth of the tumor arising in the bones surrounding or constituting the cavity (31). The ranking of periorbital regions giving rise to orbital osteoma, in particular the paranasal sinuses, is a matter of debate. In general, the bony walls of the frontal and ethmoid sinuses are considered the predilection sites of orbital osteomas (15, 16, 20). Beyond the relative frequency of origin in orbital osteomas, these sites are the most frequent origin of osteoma in general. On the other hand, Fu et al. (30) noted that the maxilla was the origin of paranasal osteoma in 15 out of 31 consecutive cases. The maxilla gave rise to more osteoma than the nasal bones and other paranasal sinuses.
The predominant symptom is localized pain, including headache. This symptom is probably dependent on the topography of osteoma. Headache was noticed in about 20% of patients with frontal sinus osteoma (32), but increased to 80% in those with osteoma of the sphenoid sinus (28). Maxillary osteoma in close proximity to the trigeminal nerve branches might prompt neuralgiform pain (33). A further frequent finding in maxillary osteoma is a superior position of the globe, diplopia and exophthalmos (15, 31). The proportion of osteoma with orbital involvement becoming symptomatic due to ophthalmic symptoms is estimated at 20-30% (1). Slow growth is characteristic for osteomas of this region (16); a rapid course of growth is rare (34). Pedunculated osteomas of the orbital floor were also reported by Miller et al. (19) and Roth and Han (20). Secondary invasion of the orbit from adjacent bones is the most common pathogenesis of orbital osteoma and is more difficult to treat than isolated primaries (1). Isolated maxillary osteomas of other parts of this bone, such as the tuber (35), the molars (36) and frontal teeth (37), or central parts of the bone (33, 38) were also noted but usually do not infiltrate the orbit (1). Multiple osteoma of the maxillary sinuses are rare (39). Extensively growing osteoma of the skull base and mandible with remarks on the differential diagnosis of Gardner's syndrome have been described in detail (40, 17). Surgical therapy of orbital osteoma depends on localization, extension and symptoms. Osteoma of frontal sinus and maxillary sinus are purportedly detected at a late stage of development, frequently being an incidental finding. Therapy is recommended in tumors involving the retromaxillary space and brain (15), tumors causing eye symptoms including orbital abscess (18, 33) or for differential diagnosis of the osseous lesion, e.g. hyperostosis in the course of extracranial/orbital meningioma (1, 8, 14, 16). Sphenoid sinus osteoma is advised to be resected due to the risk of sudden blindness in the course of untreated growth (16, 28, 41).

Orbital situs prior to tumor extirpation, showing the displacement of the infraorbital nerve due to the extension of the tumor to the cavity (arrow indicates lateralized nerve).
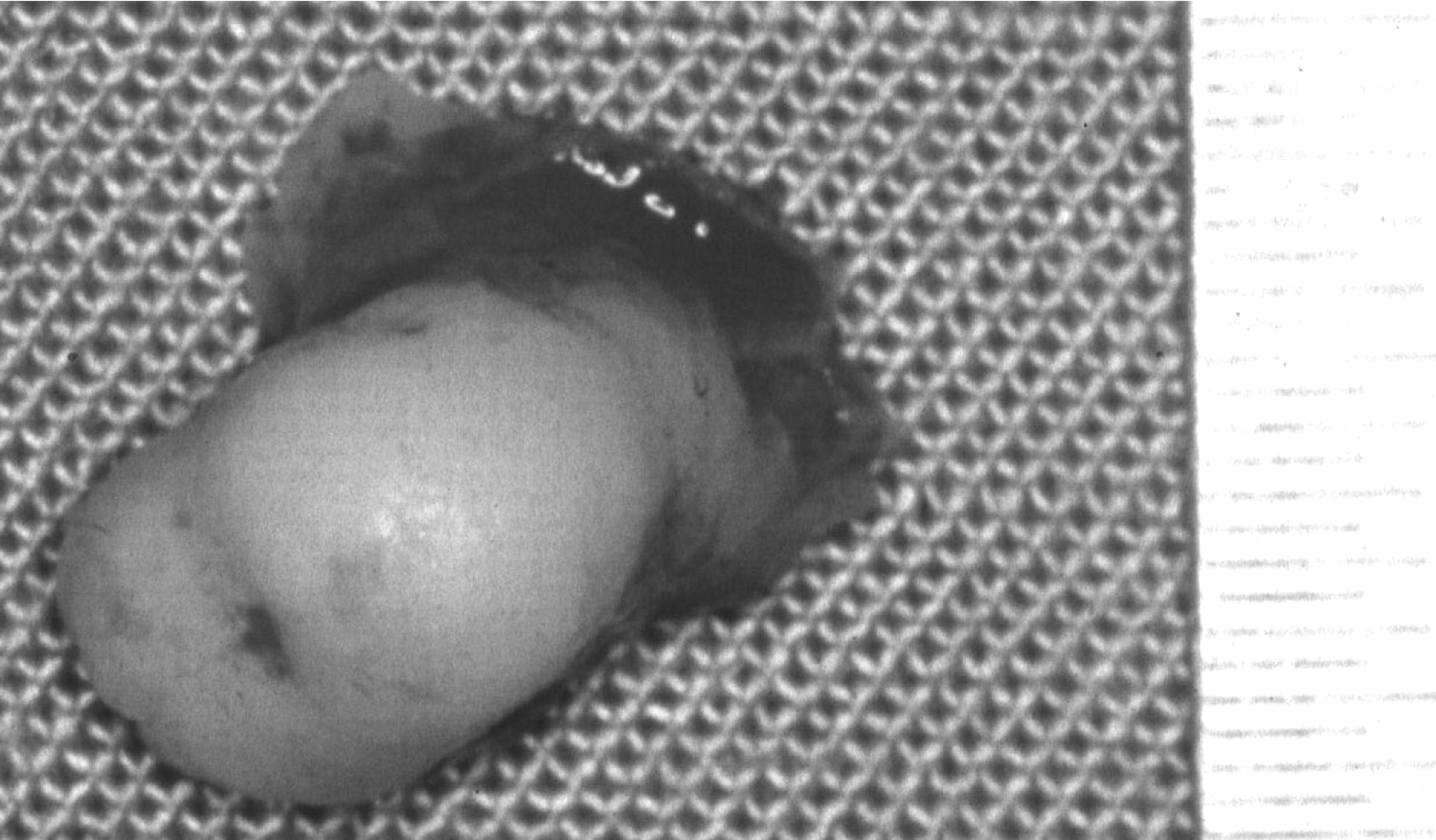
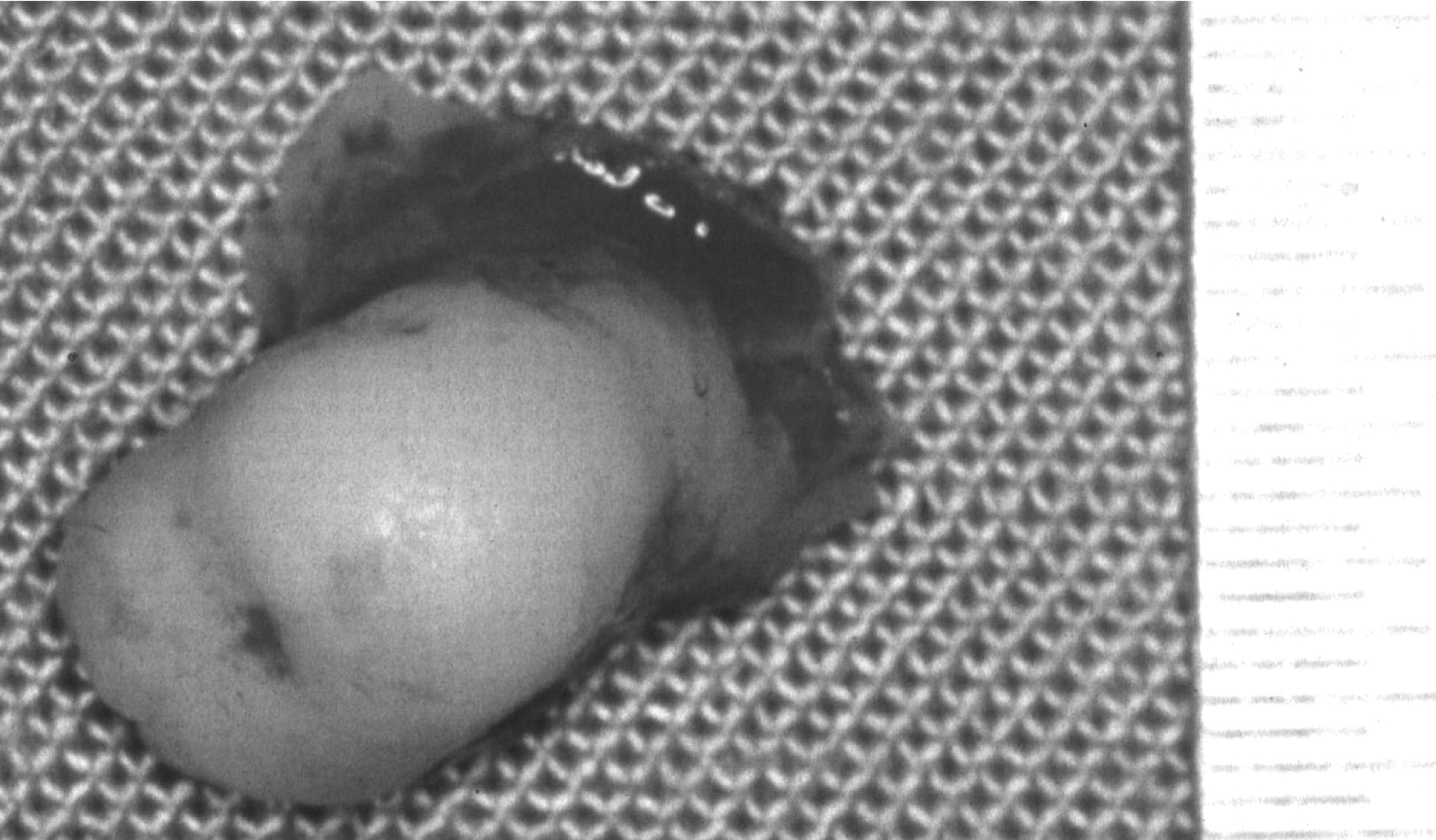
Extirpated tumor with a margin of the orbital floor.

Detail of a radiograph with occipitomental projection (Water's view) of the midfacial region, depicting the left orbit 13 years following surgery, demonstrating complete remission after tumor extirpation.
The etiology of osteoma is unknown (1). The history of trauma during childhood as a cause of tumor induction is repeatedly discussed in the literature (42). However, this putative pathomechanism is unlikely to establish pathogenesis due to the high number of facial traumas and the low number of osteoma. Other authors suggest that osteomas might be derived from cell complexes of indifferent periosteal layers (8).
In rare cases, osteomas might indicate a case of Gardner's syndrome (familiar intestinal polyposis), in particular incidental findings on skull radiographs (43). The frequent association of skull osteoma and Gardner's syndrome and the presumption that about half of patients with Gardner's syndrome lack any family history of this disease resulted in the recommendation for colonoscopy of all patients with osteoma, irrespective of age or familiar burden of the disease (24).
- Received June 30, 2008.
- Revision received November 28, 2008.
- Accepted December 2, 2008.
- Copyright © 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}