


Abstract
Background/Aim: Chronic Myeloid Leukemia (CML) is a clonal myeloproliferative disease, and a major challenge for the eradication of CML is to understand the cause of the permanence of minimal residual disease (DRM). This work aimed to induce the maturation of leukemic stem cells with All-trans-retinoic acid (ATRA), making them sensitive to treatment with Imatinib (IM). Materials and Methods: K562 cells were treated with IM and with the combined therapy of ATRA together with IM for 48 and 72 h. The expression of BCR-ABL gene and multidrug resistance gene ABCB1 were evaluated using RT-qPCR. Results: The combined ATRA and IM therapy showed a discreet cell differentiation pattern, evidenced by the panoptic morphology analysis at 48 and 72 h of treatment. The BCR-ABL expression showed no statistical difference when treated alone with IM, however in combination with ATRA, the expression was statistically significant in 48 and 72 h (p≤0.0001) and when the treatment groups were compared to each other (p≤0.001). The ABCB1 gene expression showed a decrease in isolated IM therapy (p≤0.05) and in the combination in 48 and 72 h (p≤0.0001). Conclusion: Combined ATRA and IM therapy was shown to be effective in decreasing BCR-ABL and ABCB1 genes, possibly through the differentiation of blast cells, demonstrating that the therapy could be potentially effective in the blast crisis of the disease and for those patients who develop resistance to available CML treatments.
Chronic myeloid leukemia (CML) is a clonal myeloproliferative disease cytogenetically characterized by the Philadelphia (Ph+) chromosome, which is the result of a reciprocal translocation between the long arms of chromosomes 9 (9q34) and 22 (22q11) (1, 2). This translocation is responsible for uniting the breakpoint cluster region (BCR) and Abelson leukemia virus (ABL) genes, forming the chimeric BCR-ABL gene in Philadelphia positive (Ph+) cells. The resulting protein of this chimeric gene is the oncoprotein p210 that has tyrosine kinase activity, which confers an intense proliferative activity and a consequent adaptive advantage to Ph+ cells (3-5).
The first-line drug most used in the treatment of CML is Imatinib Mesylate (IM), a tyrosine kinase inhibitor (TKI). Its mechanism of action consists of inhibiting the chimeric BCR-ABL gene by occupying the ATP binding site, thereby inhibiting the cell signaling cascade that leads to increased cell proliferation, halting cell differentiation and resistance to apoptosis (6, 7).
IM induces a complete haematological response in almost all patients in the chronic phase; in patients in the accelerated phase the percentage decreases to 50% and, in patients who are in the blast phase, the positive response to IM is quite small (<5%) (7, 8). Despite the effectiveness of IM treatment, relapses and resistance to therapy are frequent, mostly due to multiple drug resistance (MDR), which can be found in various cancer cells drastically limiting and complicating the healing effect of drugs for a variety of tumors (9, 10).
MDR is considered a multifactorial phenomenon and occurs mainly due to the hyperexpression of ATP binding cassette (ABC) superfamily protein transporters, a large family of proteins that uses the energy of hydrolysis of ATP to expel the active drug from inside the cells (11).
Multidrug Resistant protein 1/ATP Binding Cassette Subfamily B Member 1 (MDR1/ABCB1) is a carrier that was initially identified in cells related to resistance to multiple drugs and can expel a wide variety of structurally unrelated drugs that enter cells through passive diffusion and, as a result, the drug’s intracellular level fails to reach an ideal toxic concentration to become effective (12).
Studies have shown that those resistant cells are part of the undifferentiated compartment of leukemic stem cells (CD34+) (13-15). This demonstrates how challenging it is for therapies involving TKI to eradicate the permanence of minimal residual disease (DRM) and, consequently, to end the cases of disease recurrence (16, 17).
All-trans-retinoic acid (ATRA) is a metabolite of retinol and belongs to the class of retinoids. Studies with ATRA in vitro have demonstrated its great potential to induce differentiation and inhibition of cell proliferation in transformed hematopoietic cell lines, including those derived from human myeloid leukemia cells (18, 19).
This work aims to circumscribe the resistance of immature hematopoietic stem cells (CD34+) to chemotherapy treatment; we propose to induce the differentiation of these cells with ATRA using the blast cell line model K-562, making these cells mature and sensitive to treatment with IM.
Materials and Methods
Cell culture. Chronic myeloid leukemia cells K-562 were kindly provided by Professor Vivian M. Rumjanek from the Federal University of Rio de Janeiro, Brazil and maintained in RPMI medium with 10% (v/v) fetal bovine serum (Gibco®, Carlsbad, CA, USA). All cells were maintained in media with 1% (v/v) penicillin (100 U/ml) and streptomycin (100 mg/ml) (Gibco®, Carlsbad, CA, USA) and incubated with 5% CO2 at 37°C.
Drugs. Imatinib mesylate (IM) and all-trans retinoic acid (ATRA) were purchased from Sigma Aldrich (St Louis, MO, EUA). The stock solutions of ATRA and IM were diluted in culture medium to reach final concentrations ranging between 0.195 and 25.0 μg/m, for both drugs. The maximum concentration of DMSO added to the cells was 0.33%.
Cell treatment. K-562 cells were seeded (5×103 cells per well) in a 96-well plate and treated with IM or co-treated with ATRA and IM for 48 and 72 h. For IM, the highest concentration tested was 50.6 μM and for ATRA 83.21 μM.
Panoptic stain. For the evaluation of differentiation pattern and morphological changes after ATRA treatment, with the highest concentration of 83.21 μM, about 100ul (5×10³ cells) of K-562 cells were placed in a cytocentrifuge for 10 minutes at 1,000 rpm with previously cleaned slides. Subsequently, the slides were stained using the Fast Panoptic kit (LaborClin®, PR, Brazil), following the manufacturer’s manual with modifications. To assess changes in cell morphology, the slides were analyzed and photographed under an optical microscope Evos® XL (Life Technologies, Carlsbad, CA, USA) in 40× magnification.
Cell cycle progression. To evaluate the cell cycle distribution after ATRA treatment, K-562 cells were seeded at 3×103 cells per well in 96-well plate and treated with ATRA at 83.21 μM, for 48 and 72 h of exposure. After this procedure, cells were fixated in 80% ethanol solution for 30 min at 4°C and then incubated with propidium iodide (50 μg/ml) for 30 min. A total of 20,000 cells were evaluated by flow cytometry (BD FACSVerse) and data were analyzed using FlowJoSoftware v.10 (Becton Dickinson, Franklin Lakes, NJ, USA).
Extraction of RNA and reverse transcription to DNA. RNA from the cells was extracted with TRIzol Reagent® (Invitrogen™, Carlsbad, CA, USA) according to the manufacturer’s instructions. From 20 ng of RNA, the cDNA was synthesized using the High-Capacity cDNA Reverse Transcriptase kit (Life Technologies, Carlsbad, CA, USA). The conversion step was performed on a Veriti® thermal cycler (Applied Biosystems®, Foster City, CA, USA). After this step, the samples were stored in a freezer at −20°C until further use.
Gene expression analysis by real-time quantitative polymerase chain reaction (RT-qPCR). The genes selected for evaluation were BCR-ABL1 (Hs03024784_ft) and ABCB1 (Hs00184500_m1), while the ABL gene (Hs01104728_m1) was used as an internal control. The detection method was the TaqMan® Gene expression assays (Applied Biosystems®, Foster City, CA, USA) and qPCR was performed using QuantStudio5® Real-Time PCR system (Applied Biosystems®, Foster City, CA, USA). For each sample, the following were used: 3 μl of cDNA, 1 μl of each primer/probe, 12.5 μl of TaqMan® Gene Expression Master Mix (Life Technologies, Carlsbad, CA, USA) and 8.5 μI of ultra-pure water. The gene-expression levels were based on relative analyses and calculated using the 2−ΔΔCT (delta delta threshold cycle) method (20). Each sample was analyzed in triplicate for experimental validation (21).
Statistical analysis. One-way analysis of variance (ANOVA) was performed to analyze gene-expression data, with a significance level of 5% (p<0.05). Data were analyzed using the mean and standard deviation of three independent experiments. The Bonferroni correction was used for multiple comparisons.
Results
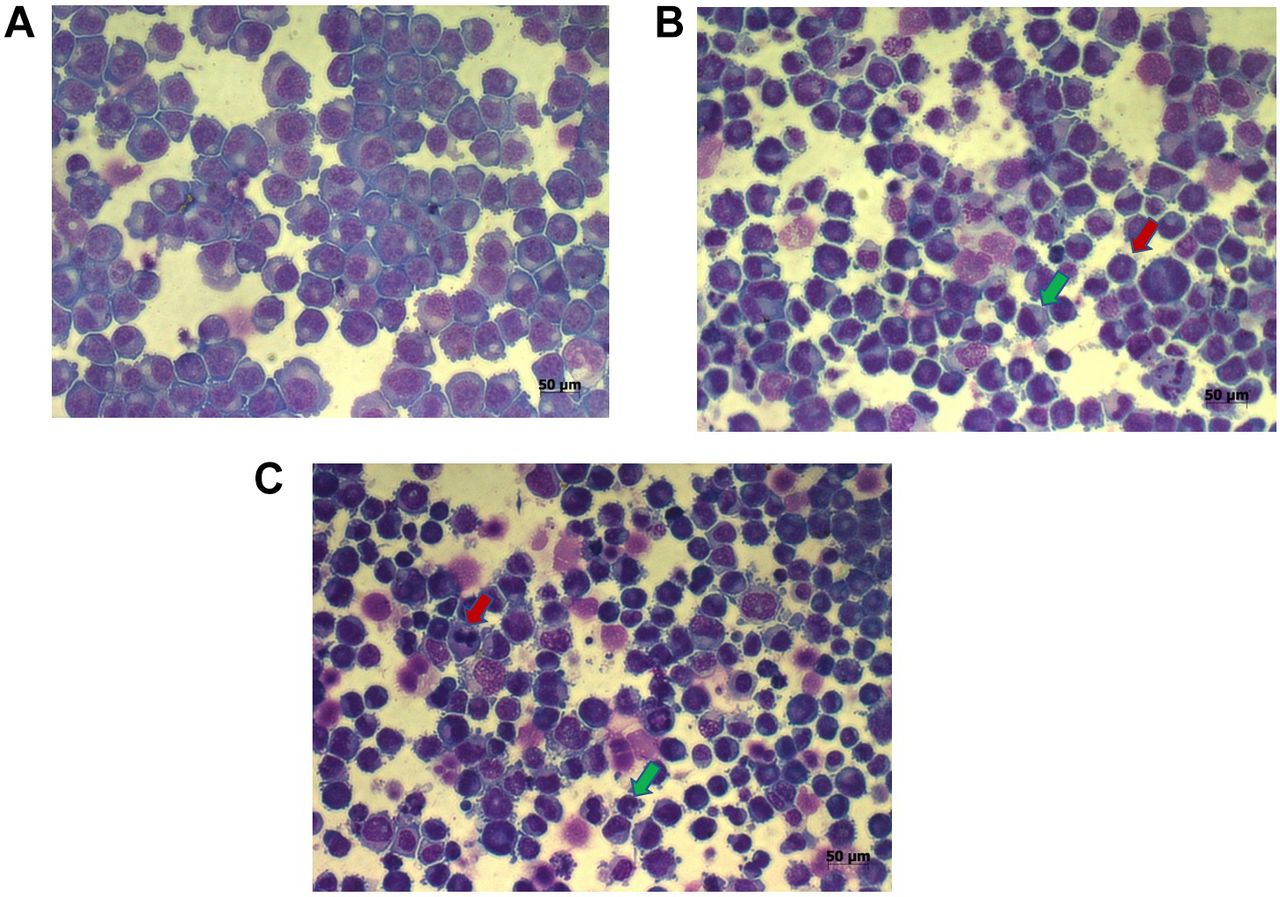
The analysis of cell morphology by Panoptic staining showed a discrete pattern of cell differentiation after ATRA treatment, with exposure at the highest tested concentration (83.21 μM) after 48 and 72 h of treatment in K-562 cells (Figure 1A-C). The cells after treatment demonstrated a pattern of cell maturation and differentiation compatible with that seen in the hematopoietic process, showing a slight differentiation of cell maturation and the presence of myelocytes and metamyelocytes after 48 h of treatment (Figure 1B). The analisys after 72 h of ATRA and IM exposure, showed a proeminent hematological cell differentiation and the presence of band forms and granulocytes (Figure 1C).

Analysis of cell morphology. (A) K-562 cells without treatment, showing the huge and exclusive population of immature cells of blast origin; (B) K-562 cells after 48 hours of exposure to ATRA treatment, demonstrating a slight differentiation of cell maturation and the presence of myelocytes (red arrow) and metamyelocytes (green arrow); (C) K-562 cells after 72 hours of ATRA exposure presenting a proeminent cell differentiation and the presence of band forms (red arrow) and granulocytes (green arrow).
The cell cycle analysis showed a change in pattern distribution of cells after 83.21 μM of ATRA exposure, at 48 and 72 h after treatments indicating that ATRA induced the cell proliferation and differentiation (Figure 2A-C).

Cellular effects of 83.21 μM ATRA treatment in the leukemia cell line K-562. Graph represents the cell cycle distribution after ATRA exposure for (A) 48 h and (B) 72 h. (C) Table represents the mean±SD of the percentage of cells in Sub-G1, G0/G1, S and G2/M phase upon exposure to 83.21 μM ATRA.
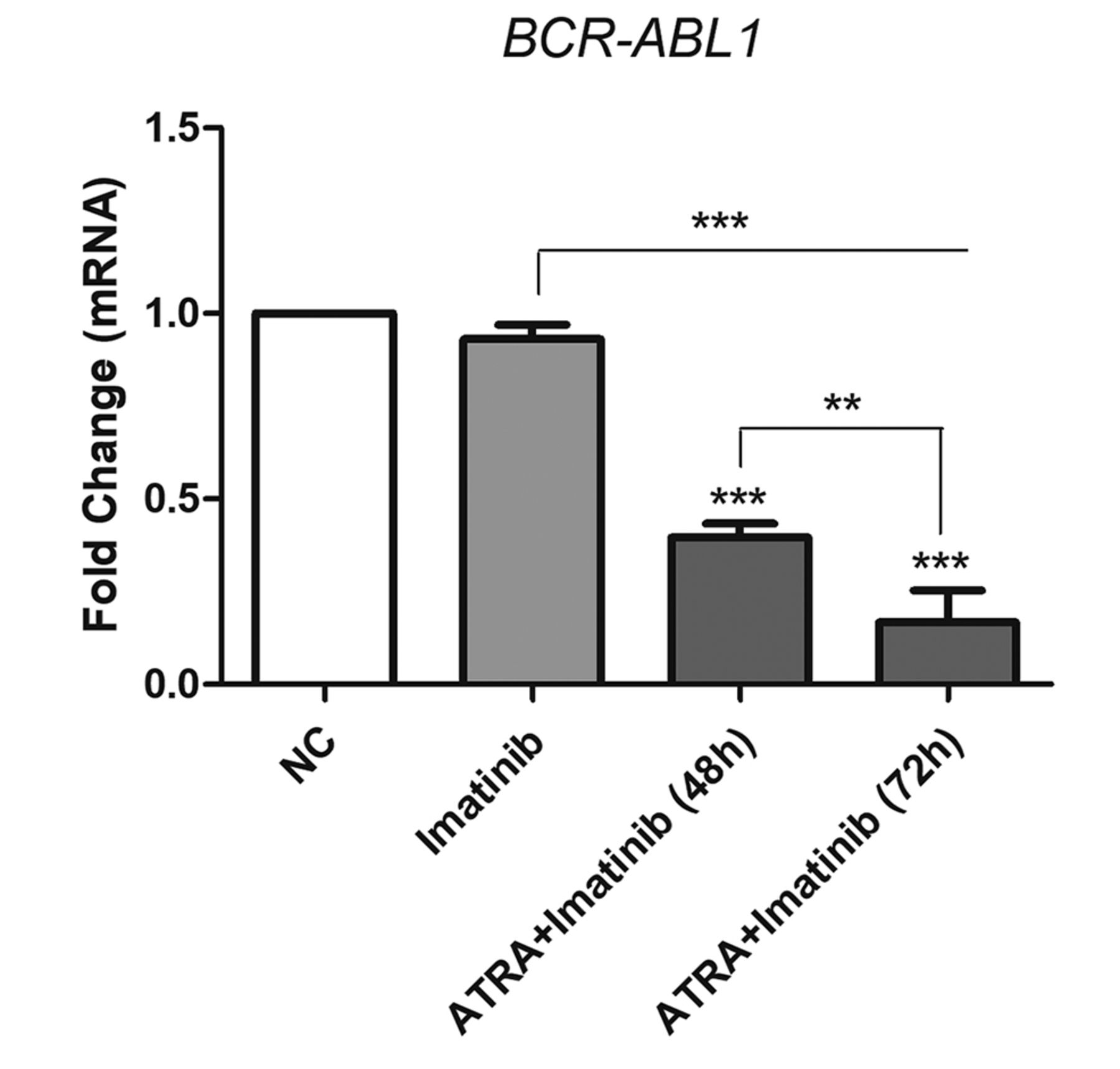
The next step was to evaluate the gene expression levels of BCR-ABL1 and ABCB1 genes after cellulartreatment with Imatinib, ATRA and with the combined therapy at the highest concentrations. The BCR-ABL expression showed no statistical difference when treated alone with IM, however in combinationwith ATRA, the expression was statistically decreased in 48 and 72 h (p≤0.0001) and when the treatment groups were compared to each other (p≤0.001) (Figure 3).

Evaluation of breakpoint cluster region - Abelson murine leukemia (BCR-ABL1) gene expression in the K-562 cell line after treatment with IM alone or ATRA together with IM at the highest tested concentrations. Fold change data are represented as mean±standard deviation of three independent experiments. BCR-ABL gene expression was compared between the leukemia cell line K-562, relative to that in MRC-5 lung fibroblasts, using ANOVA with Bonferroni correction. **p<0.001 and ***p<0.0001. NC: Negative control.
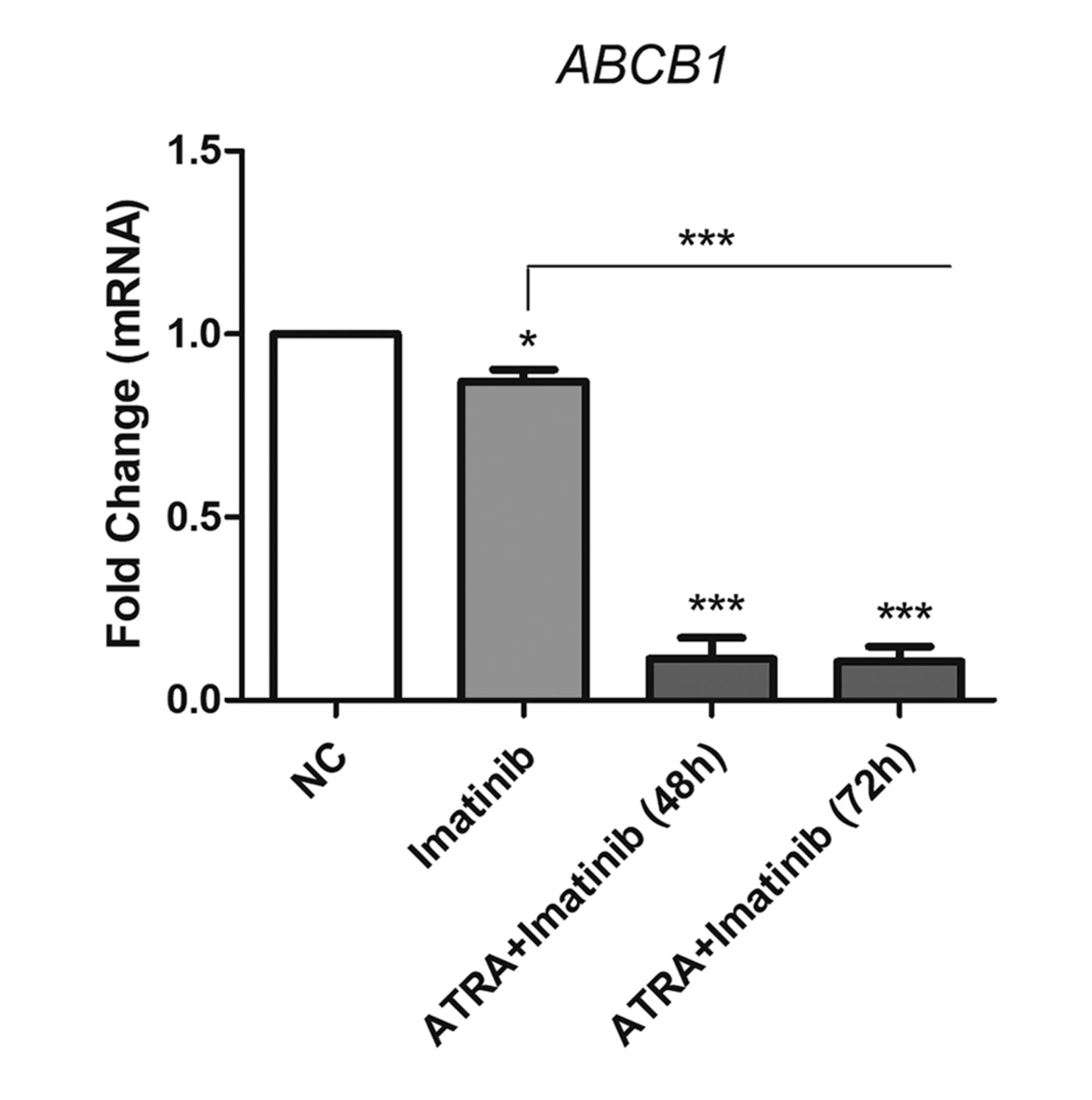
The ABCB1 gene expression analysis showed a significant decrease in IM therapy alone (p≤0.05) and a more significant decrease in the combined therapy of ATRA together with IM in 48 and 72 h (p≤0.0001). This shows that the co-therapy presented a greater inhibition of the ABCB1 gene transcripts (Figure 4).
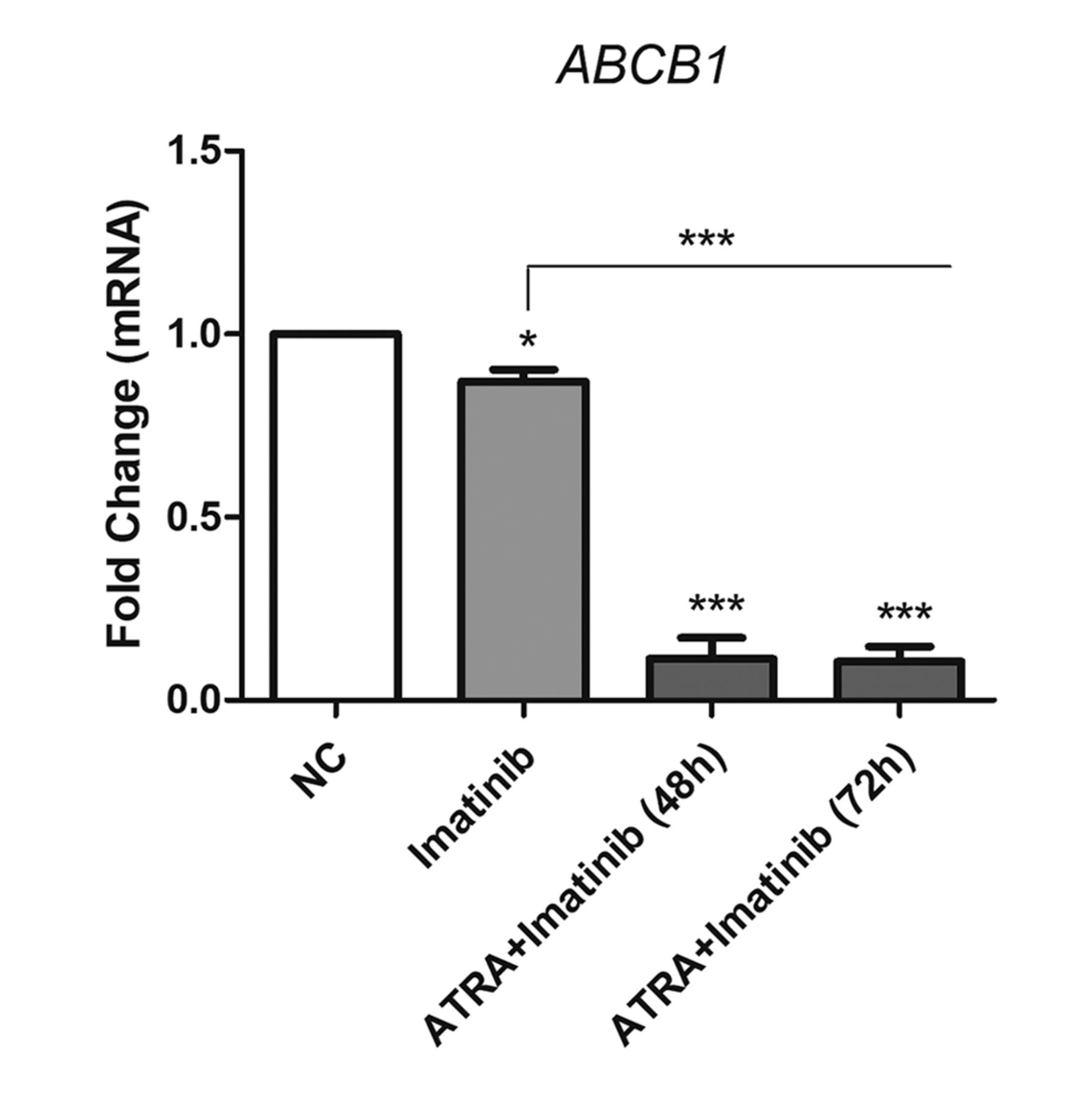
Evaluation of ATP Binding Cassette Subfamily B Member 1 (ABCB1) gene expression in K-562 cells after IM alone or ATRA and IM treatment at the highest tested concentrations. Fold change data are represented as mean±standard deviation of three independent experiments. ABCB1 gene expression was compared between the leukemia cell line K-562 relative to the MRC-5 cell line, using ANOVA with Bonferroni correction. *p<0.05 and ***p<0.0001. NC: Negative control.
Discussion
TKIs targeting the BCR-ABL protein, like IM, have brought a revolutionary change in the CML therapy (22) and although the generation of these TKIs has greatly improved the CML prognosis, a significant portion of patients have a response treatment failure due to resistance to these drugs (7, 23).
Our results demonstrated that the combined therapy of ATRA and IM was able to promote hematopoietic differentiation of the granulocytic lineage in K-562 cells, observed in 48 and 72 h after treatment (Figure 1A-C). The Panoptic stain demonstrated that ATRA may have had an influence on this role, since ATRA causes immature cells to develop into differentiated mature hematologic cells, which might contribute to mitigating the disease. Additionally the cell cycle progression analysis demonstrated that 83.21 μM of ATRA also induced a change in the pattern distribution of cells compared to untreated controls (Figure 2A-C).
ATRA, combined with other drugs, is used to treat acute promyelocytic leukemia (LPA), making immature promyelocytes capable of differentiating into mature granulocytes (24, 25). Knowing that the main characteristic of leukemias is the presence of highly proliferative immature cells, the ability of ATRA and its derivatives to induce cell differentiation in altered hematopoietic cell lines, such as the K-562 line, has been explored in several studies (26, 27). Previous studies have proven that pharmacological induction with ATRA was able to promote phenotypic changes of the K562 lineage in differentiated cells from the granulocytic and erythroid hematopoietic lineages (28, 29).
In this work, the results referring to the analysis of the gene expression of BCR-ABL1 transcripts were also positively affected by the combined treatment, which significantly demonstrated a decrease in expression levels in 48 and 72 h (p<0.0001) and with an increase in inhibitory potency after 72 h when treatment times were compared (p<0.001). In myeloid strains previously resistant to TKI, ATRA blocked the acquisition of BCR-ABL mutations and resistance to TKI (30, 31). In a recent study, a CML patient who progressed to a promyelocytic blast crisis treated with ATRA and arsenic trioxide achieved complete morphological remission (32).
Additionally, a study previously carried out by our research group showed that the expression of BCR-ABL1 levels between leukemic cell lines, including K-562, and patients with CML was similar. This validates the use of these cell lines as an indispensable tool for the knowledge of the particularities related to the development, differentiation, and susceptibility to the treatment of tumor cells (33).
After the induction of ATRA and IM co-therapy, we evaluated the MDR/ABCB1 gene expression. The data demonstrated that the combined therapy was able to significantly decrease expression levels at 48 and 72 h after treatment (p<0.0001), showing an important molecular effect in blocking the MDR phenotype. MDR mediated by members of the ABC superfamily has therefore become one of the greatest obstacles to overcoming tumor progression and the overexpression of these proteins results in an increase in the resistance of cancer cells to chemotherapy, which can be a determining factor for patients’ non-response to antineoplastic treatments (34).
The acquisition of resistance to chemotherapy treatments in cancer patients is a major clinical problem and remains a critical obstacle in antineoplastic treatment and, therefore, the elucidation of the molecular mechanisms underlying the MDR phenotype is important to identify possible targets in human cancers (9).
Moreira-Nunes et al. reported that there is a greater presence of drug influx and an absence of efflux channels in mature granulocytic cells (CD66b+) from CML patients and thus, mature cells tend to respond better to treatment with Imatinib. In contrast, stem cells (CD34+) showed a decrease in influx channels and an increased presence of drug efflux channels that are widely known in the literature as agents that cause resistance to chemotherapy. This may be the answer to why CD34+ cells are insensitive to IM treatment (17).
The data presented here emphasize the need and importance of further studies on hematopoietic progenitors’ cell differentiation and their role in therapeutic efficiency in patients with refractory leukemia with resistance to therapies available and persistence of DRM.
Conclusion
Combined ATRA and IM therapy has been shown to be effective in decreasing the expression of the BCR-ABL gene, possibly through the differentiation of blast cells, making them the target of IM therapy. In addition, the data demonstrated that the combination ATRA and IM also favors the decrease of the ABCB1 molecular chemoresistance mechanism, demonstrating that the therapy could be potentially effective in the blast crisis of the disease and for those patients who develop resistance to available CML treatments.
Acknowledgements
The Authors would like to thank the Multi-User Facility of Drug Research and Development Center of the Federal University of Ceará for technical support. This study was supported by Brazilian funding agencies of the National Counsel of Technological and Scientific Development (CNPq; to Burbano RMR, Moraes MEA and Moreira-Nunes CA) and Amazon Foundation for Support Studies and Research (FAPESPA, #122/2014 to Moreira-Nunes CA).
Footnotes
This article is freely accessible online.
Authors’ Contributions
Lemos JAR and Moreira-Nunes CA, performed the study design; Pinto CA, Barbosa MC, Portilho AJS, and Moreira-Nunes CA, performed the cell culture analysis; Pinto CA, and Moreira-Nunes CA performed the molecular and statistical analysis; Pinto CA, RMRB, Moraes MEA, and Moreira-Nunes CA wrote the article. All Authors read and approved the final article.
Conflicts of Interest
The Authors declare no conflicts of interest regarding this study.
- Received May 6, 2021.
- Revision received May 31, 2021.
- Accepted June 2, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.