


Abstract
Background/Aim: Leiomyoma is a rare benign tumor originating from smooth muscle fibres. In the respiratory tract, these tumors are rare and in the pleura, cases are exceptional, with only a few reported so far. This is the main reason we decided to present this case of primary leiomyoma of the visceral pleura. Case Report: We present a case of a 51-year-old asymptomatic patient who, during a routine medical examination using standard chest radiography, presented with a 3 by 2 cm homogenous mass in the right superior pulmonary area, tangent to the chest wall (same level with the 3rd rib). Further investigation using computed tomography (CT) in the chest confirmed the presence of a 31/18 mm solid mass in the right upper lobe, in contact with the parietal pleura. Surgery was performed for two reasons: i) removal of the tumoral mass and ii) establishing a histopathological diagnosis. Intraoperatively, a well-defined, homogenous, ivory white non-infiltrating mass was discovered in the right upper lobe on the visceral pleura and in close proximity to the minor fissure. The mass was removed with negative surgical margins and was left with healthy tissue. Histopathological examination and immunohistochemistry came as a surprise, establishing our diagnosis of leiomyoma. Conclusion: Primitive pleural leiomyoma must remain a possibility when considering the differential diagnosis of pleural tumors. The main course of treatment is complete surgical resection. In our case, long-term follow up did not present any local recurrence.
Leiomyoma is a tumor originating in smooth muscular fibres and can occur anywhere in the body where this cell type exists. Leiomyomas are part of the mesenchymal tumor category. Most often, these tumors are present in the uterus, esophagus and small intestine (1, 2). The first description of leiomyoma belongs to Wirshaw in 1854 (1) while Steinard reported the first case of pulmonary leiomyoma in 1939 in a patient that also presented with a uterine fibroma (3). In 1958, Kloepfer described the presence of hereditary leiomyomatosis (2). Other hereditary leiomyomatosis have since been described with multiple simultaneous locations (4); however, the presence in the respiratory tract of a leiomyoma is rare, representing 2% of benign tumors found in this region (5, 6).
Primary pulmonary leiomyoma was first described in 1907 as a standalone pathology (7), with the first case of pulmonary leiomyoma being reported by Forkel, in 1910 (8). Respiratory leiomyoma develops during the 3rd and 5th decade of life, with a median age of 35 years, and a two-fold higher frequency in women (5). On the other hand, leiomyoma of the great airways, such as the trachea and main bronchi, are more often found in men (5).
Case Report
A 51-year-old non-smoker, asymptomatic male patient, presented himself at our clinic for a routine medical examination. Physical examination discovered no obvious signs of illness; however, standard thoracic chest radiography revealed the presence of a 3 by 2 cm macronodular, well-defined, homogenous opacity in the right superior hemithorax, adjacent to the chest wall (3rd rib). Blood analysis consisted of complete blood count, biochemistry and clotting tests, all of which appeared normal. Additional examination consisted of thoracic and superior abdomen CT scan with contrast agent (Figure 1), which identified a solid, homogenous, well-defined tumoral mass in the right upper lobe with no infiltration of adjacent tissues, and in contact with the parietal pleura. The mass had a density of 45 Hounsfield units and a size of 31 by 18 mm. No hilar or mediastinal lymph nodes were detected as well as no secondary lesions in the liver or adrenal glands. Both the CT scan and the chest radiography pointed our diagnosis to a primitive right intrathoracic tumor, but with no knowledge of the histopathological background. Bronchoscopy, lung function tests, electrocardiogram and echocardiography results were all within normal parameters.

Computed tomography. View of lesion (arrow) on the right hemithorax.
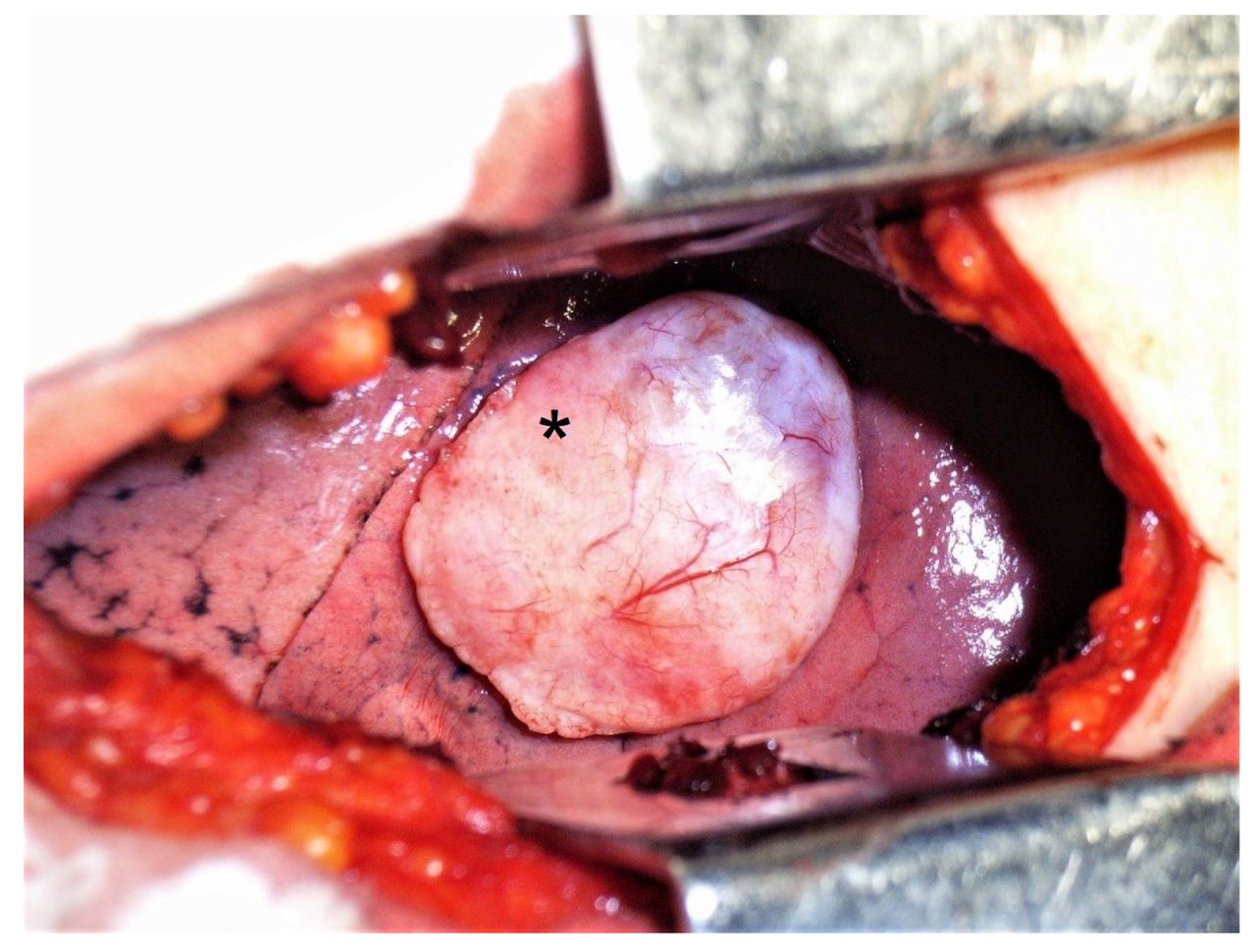
Under these circumstances, we decided to perform surgery using a right antero-lateral thoracotomy through the fourth intercostal space (Figure 2). Intraoperatively, we discovered an apparently encapsulated, well-defined, ivory mass on the upper right lobe with no signs of local invasion into adjacent structures. The mass had a small base of implantation on the visceral pleura of the right upper lobe, close to the minor fissure, with a size of 30/20/15 mm. Its presence there suggested a solitary pleural fibroma and, as a consequence, the resection was performed according to the guidelines for this pathology, with tissue excision up to healthy lung tissue, 2 cm in all directions from the base of implantation followed by suturing the pleura.

Intraoperative aspect of the tumor (asterisk).
Postoperative evolution was favourable with no complications, and the patient was discharged after 7 days. Histopathological examination using haematoxylin-eosin staining and a 10× magnification identified lung tissue with modified architecture (left side of Figure 3A by the presence of tumoral proliferation (right side of Figure 3A) consisting of fusiform cells with an intertwined disposition with no precise cellular limits. Using a 40× magnification (Figure 3B), we discovered tumoral proliferation of fusiform cells, with abundant, eosinophil cytoplasm and long nuclei, with no cytonuclear atypia. These histopathological findings plead for leiomyoma.

Histopathological aspect of the resected tumor. A) Histopathological aspect of the resected specimen showing normal pulmonary (arrow) as well as tumoral tissue (asterisk) – magnification: 10×. B) Histopathological aspect of the resected specimen showing normal pulmonary (arrow) as well as tumoral tissue (asterisk) – magnification: 40×.
Immunohistochemical stains were performed on formalin fixed paraffin-embedded tissue: MIB1/Ki-67 (monoclonal, Ki88, BioGenex), SMA (monoclonal, 1A4, Biocare), Desmin (monoclonal, D33, Biocare), S100 (polyclonal, Dako), Vimentin (monoclonal, SP20, Biocare) and CD117 (monoclonal, EP10, Biocare).
The slides were retrieved from the thermostat, deparaffinized and then rehydrated in three successive baths of ethyl alcohols (descending grades: 100%, 96%, 80%).
The inhibition of the endogenous peroxidase was made with hydrogen peroxide (H2O2) 3% for 10 min, at room temperature.
The technique used for immunohistochemistry was avidin-biotin-complex (ABC), Vectastain kit (Vector Laboratories, Burlingame, CA, USA), a three-step method that begins with the recognition of tissular antigen by the primary antibody. The incubation with the specific primary antibody is made at 4°C, overnight, in a moist chamber. After that, the slides were washed for 10 min in phosphate-buffered Saline (PBS), pH 7.4 and incubated for 30 min with secondary antibody (at room temperature). The biotinylated secondary antibody binds to the primary antibody. Then, the complex formed by avidin and the biotinylated enzyme attach to the secondary antigen. Slides were visualized using a 3,3’-diaminobenzidine (DAB) kit (Vector Laboratories).
The tumor was intensely positive for smooth muscle actin (SMA), vimentin and desmin and negative for cluster of differentiation 117 (CD117), S-100 protein, with a Ki67 index lower than 1%.
These results further confirmed our histological diagnosis of leiomyoma (Tables I and II).
Immunohistochemistry.
Antibodies used to confirm the presence of a pleural leiomyoma.
Follow up of the patient after 1-year using chest radiography and CT imaging showed no signs of local recurrence or secondary lesions.
Discussion
Leiomyomas of the respiratory tract are not that common, even more so the primary pleural ones, with only a few reported cases in the literature. With regards to the thoracic localization, leiomyomas are found in the pulmonary parenchyma, bronchi, trachea, parietal pleura, thoracic wall, diaphragm and the mediastinal or visceral pleura (9). There are also some reported cases involving the esophagus, or even the great intrathoracic vessels but, according to some authors, they are more commonly described in the urogenital tract, occasionally in the gastrointestinal tract and rarely in the respiratory tract (9).
Concerning the respiratory tract primary leiomyomas, approximately 51% of cases are found in the lung parenchyma, 33% are endobronchial and 16% are located at the level of the trachea (10). Especially for the tracheal localisation, leiomyomas represent 1% of all tracheal tumors (11). Primary localisation of leiomyomas in the thoracic wall or at the level of the mediastinal, visceral and parietal pleura are extremely rare (12). Parietal pleura is also considered as part of the chest wall, and so, in some authors’ view, the terminology of group chest wall leiomyoma can be described as if it includes both groups (13).
Some authors consider the histological origin of these tumors in the smooth cells of the vascular wall in blood vessels found in the thoracic wall or the pleura (13, 14). When it comes to the leiomyoma of the tracheobronchial tree, this seems to originate in smooth muscle fibres of the bronchial arterioles (6, 15). There are reported cases of leiomyomas originating from the vascular wall of the great vessels, such as the pulmonary vein or the inferior vena cava (16-18). A particular case of leiomyoma derived from the wall of the uterus vessels has been described to represent a form of intravenous leiomyomatosis. This leiomyoma eventually progressed through the left iliac vein along the inferior vena cava, then inside the heart chambers and in the branches of the right pulmonary artery (19).
Another particular type of this disease is pulmonary benign metastasizing leiomyoma (PBML), which appears alongside a uterine leiomyoma and manifests itself through the presence of multiple nodules of various sizes in both lungs (20). Positron emission tomography (PET-CT) scan in such cases does not identify any abnormal capturing of 18-fluorodeoxyglucose in the suspected nodules, with a standardized uptake value (SUV) smaller than 2.0, which points to a benign lesion. PBML develops primarily in women that have undergone hysterectomy or myomectomy for uterine leiomyoma (21).
There are several theories regarding the pathogenesis of this leiomyoma. There is the theory of cellular transport, which sustains the idea of cells migrating during the surgical manipulation of the uterus through the venous and lymphatic systems, ultimately reaching the lung (22). Then, there is the theory of distant metastasis, which considers that leiomyoma is actually a leiomyosarcoma with a low malignancy index and yet well differentiated histologically (20). The third theory, the multifocal one, refers to the situation in which the pulmonary lesions are discovered before or at the same time as a uterine fibroma (23). Moreover, certain authors consider that the evolution of pulmonary lesions are hormonally influenced; oestrogen favours tumor growth while progesterone inhibits it (24). PBML has been correlated with strong positive oestrogen receptors (ER) and progesterone receptors (PR) (24, 25).
Genetic studies have demonstrated that metastatic lung lesions belong to the same malignant cellular lineage as those from the uterine leiomyomas and have the ability to develop new mutations during tumoral evolution (26). Another disease in which leiomyoma is present is hereditary leiomyomatosis, which is a dominant autosomal hereditary illness associated with increased risk of multiple uterine and skin leiomyomas, renal cancer and pulmonary lymphangiomyomatosis manifesting as chylothorax (27).
Due to the differences in biological manifestations when compared to other types of pleural malignant tumors, from a histological point of view, smooth muscle tumors must be taken into consideration when it comes to diagnosing primary fusiform cell tumors of the pleura (Pleural fibromas) (28-30).
Histology presents leiomyoma as being formed of smooth muscle cells with benign characteristics, no necrosis and reduced mitotic activity. Immunohistochemistry is intensely positive for smooth muscle actin (SMA), desmin and vimentin and negative for human melanoma black 45 (HMB-45), cluster of differentiation 117 (CD117) and protein S-100, with a low proliferation index Ki67 in the tumoral cells (31-33).
Clinically, cases of primitive pleural leiomyoma presented in the literature usually manifest through thoracic pain or are completely asymptomatic, similar to those found in the lung parenchyma. On the contrary, leiomyomas of the trachea or bronchi can manifest through obstructive or infectious symptoms (34). In our case, the patient was asymptomatic and the lesion was discovered incidentally during a routine medical examination.
Some authors consider that the most common primary pleural tumors are solitary pleural fibromas; however, leiomyoma must be included as an option during the differential diagnosis, even though it is a rare pathology (35). In fact, during the differential diagnosis other types of tumors should also be taken into consideration, such as neuromas, secondary lesions or other intrapleural tumoral masses (36, 37). In our case, we chose a cautious intraoperative approach using a wide resection with oncological margins, as if we were removing a solitary pleural fibroma. The histological diagnosis of leiomyoma came as a surprise.
Some authors consider that in order to establish the diagnostic of leiomyoma, an important role is held by a CT scan and a CT guided biopsy (38). On the other hand, other authors consider that CT-guided biopsy must only be considered for unresectable tumors or in cases which do not consent for surgery, due to the risk of dissemination and contamination of the needle path (39). In our case, we also considered surgery as the primary course of treatment and diagnosis. For PBMT, using PET-CT associated with CT-guided biopsy could help in performing a successful histological diagnosis.
Most authors agree that, irrespective of the localisation and clinical presentation of a leiomyoma, complete surgical resection should be the option of choice (38). In the case of pulmonary benign metastasising leiomyoma, hormonal treatment can be administrated as adjuvant therapy after hysterectomy or oophorectomy (38, 40).
Some cases with a parietal localisation of leiomyoma require complex resection with reconstructive surgery using a Goretex dual-mesh (41). However, in most cases of pleural leiomyomas, a simple complete resection alone or in combination with limited rib resection seems to provide a good control of the disease (12, 42).
For leiomyomas of the bronchial tree, some authors prefer electric or laser neodymium-doped yttrium aluminum garnet (ND-YAG) endoscopic resection (34, 43). In cases where there is a large endobronchial base of implantation surgical removal is recommended. For cases of malignant transformation of leiomyomas, irrespective of size, complete surgical resection is recommended (9, 44).
In large tumors it may be advisable to use preoperative embolization of the tumoral vessels, reducing the tumoral volume as well as the risk of bleeding during surgery (45). Even so, the use of video assisted, minimally invasive surgery is preferred as compared to open surgery (46, 47). Open surgery should be reserved for very large leiomyomas that cannot be fully removed using minimally invasive surgery.
In conclusion, primary pleural leiomyomas are rarely found but must not be omitted during the differential diagnosis of pleural tumors. They have a reduced malignant potential, with low risk of developing distant metastases but can locally invade tissues by tumoral growth. The main course of treatment is complete surgical resection, which seem to offer a good local and distant control of the disease, no local recurrence or distant metastases encountered during a year of follow up.
Footnotes
Authors’ Contributions
CS, AM, AG performed the surgical procedure, NB, CS, IB, BS reviewed literature data, CD performed the preoperative investigation the patient, IB, NB CS, MD prepared the draft of the manuscript, CS was the advisor of the surgical procedures; SV performed the histopathological examination; CS, NB reviewed the final version of the manuscript. All Authors read and approved the final version of the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest to declare regarding this study.
- Received January 29, 2021.
- Revision received May 15, 2021.
- Accepted May 17, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.