


Abstract
Background: Hematoxylin and eosin (H&E) is not an optimal stain to discriminate chief cells from parietal cells in gastric biopsies Materials and Methods: Fifteen sets of biopsies from the gastric corpus were consecutively stained with H&E and toluidine blue stains; chief cells stained deep blue with toluidine blue, thus contrasting with lightly-stained parietal cells. In well-oriented sections, the continuity of the chief cell zone was studied at ×4 magnification and its thickness in one field at ×10 magnification. Results: Toluidine blue stained fundic sections that exhibited normal mucosa or chronic gastritis without glandular atrophy displayed a distinct deep-blue chief cell zone, intercalated between the lightly-stained parietal cells on top and the muscularis mucosae underneath (Group A). In chronic gastritis with focal glandular atrophy or focal intestinal metaplasia, at least one focally fragmented toluidine blue chief cell zone was seen (Group B). In one case with severe autoimmune gastritis and in a case with extensive intestinal metaplasia, an absence of toluidine blue chief cells zone was recorded in the entire section (Group C). Conclusion: This quick and easy staining method made it possible to group sections from the gastric corpus into those with a continuous chief cell zone, with fragmented or with an absent chief cell zone, modalities that seem to correlate with different stages of fundic mucosal inflammation. These preliminary results should be validated in a larger cohort of gastric biopsies from patients with various diseases affecting the corpus mucosa.
The stomach is classically subdivided into three different histological mucosal zones: (i) the cardia, a 0-9 mm long mucosal segment between the oesophagus and the stomach; (ii) the fundus, built with oxyntic glands, and (iii) the antrum, showing pyloric glands (1). It should be noted that the identity of the cardia mucosa has recently been questioned, under the hypothesis that it is not a normal phenotype of the gastric mucosa but rather a metaplastic transformation of the oesophageal mucosa following protracted acid reflux (2). This notion was recently substantiated by observations in non-human primates (3). The fundic or oxyntic mucosa is composed of mucus secreting foveolar cells, hydrochloric acid (HCA) and intrinsic factor-producing parietal cells and pepsin secreting chief cells. Gastrin (4) stimulates not only parietal cells to produce HCA but also chief cells to secrete pepsinogen (5). Two types of pepsinogens have been described: pepsinogen I (PGIs), expressed in chief cells and pepsinogen group II (PGII), expressed both by the oxyntic and the pyloric mucosa (5). Pepsinogen secretion is triggered by a series of signals such as acetylcholine, cholecystokinin, gastrin, gastrin releasing peptide, secretin, vasoactive intestinal peptide, epidermal growth factor, nitric oxide (6) and moesin (7).
The fundic mucosa is subjected to many noxious agents on a daily basis. Particular attention has been paid to Helicobacter pylori (8-10), a bacteria causing acute and chronic mucosal inflammation. The profound alterations in the fundic mucosa triggered by Helicobacter pylori usually lead to atrophy and intestinal metaplasia (11). Autoimmune gastritis (12), a less common malady, causes the destruction of parietal and chief cells through a cellular host autoreaction. Destroyed fundic glands are subsequently replaced by glandular hyperplasia of the neck cells, a phenomenon known as pseudopyloric metaplasia (13).
Diseases affecting parietal cells have been investigated thoroughly (14-18), whereas much less attention has been paid to those affecting the chief cell population.
In routine stains such as hematoxylin and eosin (H&E), chief cells, located in the lower part of the glands, are described as cuboidal with pale blue-gray (amphophilic) cytoplasm (1). Parietal cells, located in the upper part of the glands, are triangular in shape with a centrally located nucleous and eosinophilic cytoplasm (1). Despite differences in the topographical location in the glands, distinction between chief cells and parietal cells in H&E-stained sections is not always straightforward. In this respect, it has been postulated that H&E is not an ideal stain for the easy discrimination between the two main cell groups present in the fundic mucosa (19).

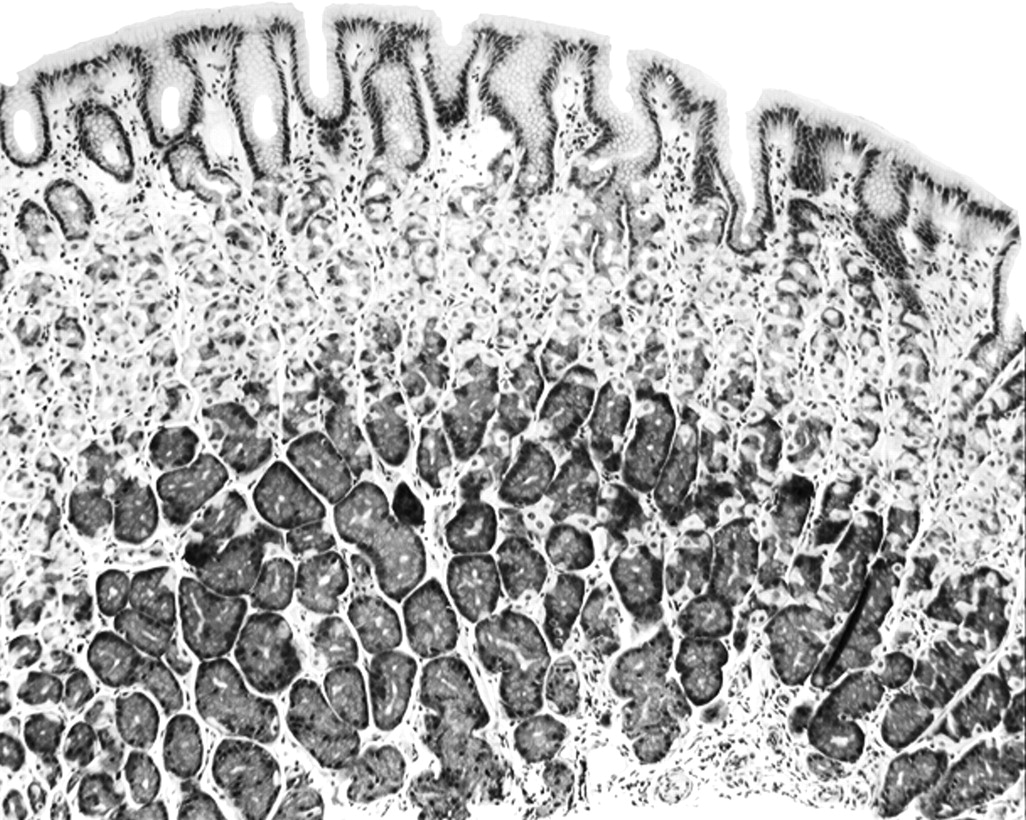
Normal fundic mucosa. Note the presence of a dark chief cell zone on the lower aspect of the mucosa (toluidine blue stain, ×20).

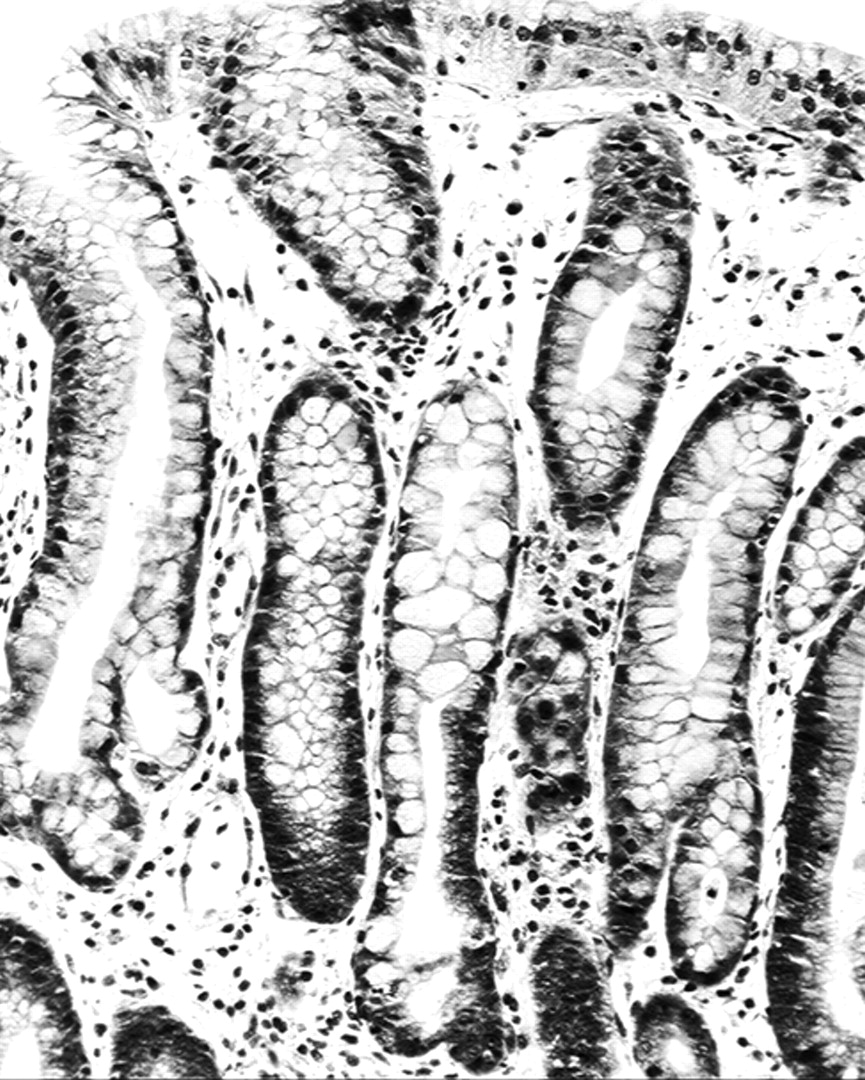
Fundic mucosa with focal glandular atrophy due to chronic gastritis. Note disruption of the chief cell zone due to inflammation (toluidine blue stain, ×40).
It was recently reported that parietal cells can easily be distinguished when gastric biopsies are stained with a modified Giemsa stain (19). More recently, while searching for Helicobacter pylori in fundic sections stained with toluidine blue (20), it became apparent that chief cells were readily highlighted by this dye.
The purpose of this study was to report this novel easy method of chief cell discrimination in a cohort of clinical gastric biopsies.
Materials and Methods
Fifteen consecutive sets of biopsies from the gastric corpus were investigated. Cases fulfilled the following prerequisites: normal fundic mucosa (n=3), fundic mucosa with active (acute) chronic inflammation without glandular atrophy (n=3), fundic mucosa with chronic gastric inflammation and glandular atrophy (n=3), or biopsies from the corpus showing intestinal metaplasia (n=3).
Fundic mucosa with absence of a chief cell zone due to extensive intestinal metaplasia (toluidine blue stain, ×20).
Sections were alternatively stained with H&E and with toluidine blue and scrutinised using a conventional microscope. Only well oriented mucosal fields were included.
Toluidine blue-stained sections showed a distinct chief cell zone (defined as a continuous field or band of chief cells) intercalated between the parietal cell band on top and the muscularis mucosae underneath. Chief cells were stained dark blue, thus contrasting against lightly stained parietal cells. The continuity of the chief cell zone was studied at ×4 objective magnification. By using an ocular microscale and ×10 objective magnifications, the thickness of the chief cell zone was assessed in one well-oriented field and the ratio chief cell zone/total mucosal thickness was calculated. In cases with chronic gastritis, fields showing spotty atrophic gastritis were selected for measurements.
Results
The continuity as well as the ratio of chief cell zone thickness/total fundic mucosa thickness was assessed in 15 gastric biopsies (Table I). Occasional lightly stained parietal cells were found within the chief cell glandular sector. These parietal cells were disregarded when calculating the chief cell zone thickness/total mucosal thickness.
A distinct, continuous chief cell zone (Figure 1) was found in fundic biopsies exhibiting normal mucosa, acute gastritis or chronic gastritis without glandular atrophy or intestinal metaplasia (Group A in Table I). In contrast, one (or more) partially discontinuous chief cell zone was recorded in fundic biopsies exhibiting chronic gastritis with either focal glandular atrophy (Figure 2) or focal intestinal metaplasia reaching the muscularis mucosal aspect of the fundic mucosa (Group B). Finally, the complete absence of a chief cell zone in the entire section was found in one case of advanced autoimmune gastritis and in one case with extensive intestinal metaplasia (Group C) (Figure 3).
Continuity, discontinuity or absence of the chief cell zone in sections from 15 gastric biopsies stained with toluidine blue. The chief cell zone/total thickness of the fundic mucosa ratio is also given.
Table I shows that the ratio chief cell zone/total mucosal thickness varied between 0.39 and 0.43 in Group A, between 0 and 0.09 in fields with atrophic gastritis in Group B and was 0 in the entire section in Group C.
Discussion
In contrast to the vast literature on gastric parietal cells and Helicobacter pylori infection, only few workers have studied diseases affecting the chief population in gastric biopsies. One possible explanation for this might be the numerous commercial markers available to lable parietal cells (H+−K+ATPase, NA+−K+ATPase, lectins, carbonic anhydrase, aquaporin 4, Huntingtin-interacting protein 1-related (Hip1r), gastric parietal cell auto-antibodies of IgG class (GPCA-IgG) (14-18), and the scarcity of available markers to label chief cells (6-7).
Early experiments in rats demonstrated that high doses of 16,16-dimethyl prostaglandin E2 increased the number of chief cells (21). Ekman et al. (22) detected a slight atrophy of chief cells in rats treated with high doses of the antisecretory drug omeprazole.
Using clinical gastric biopsies, Sipponen et al. (23) performed morphometric (point count) studies on AB-PAS stained sections. These authors found that the chief cell/parietal cell (C/P) ratio was higher after partial gastrectomy for duodenal ulcer, suggesting a proportional loss of parietal cells than chief cells after operation. In non-operated control patients, the C/P ratio decreased with increasing degree of gastritis, suggesting that in the general population, the chief cells are more sensitive than parietal cells to those factors that lead to age-dependent progression of gastritis. The study by Sipponen et al. did not discuss the presence of focal fragmentation or absence of the chief cell zone in patients with chronic gastritis (23).
The present results showed a distinct chief cell zone in biopsies of the fundic mucosa stained with toluidine blue. This distinct chief cell zone was continuous in biopsies with normal mucosa or with chronic inflammation without mucosal atrophy, disrupted (fragmented) in biopsies showing chronic gastritis with spotty atrophy or spotty intestinal metaplasia, or absent from the entire section in advanced autoimmune gastritis and extensive intestinal metaplasia. The microscopic modality groups of the chief cell zone seem to correlate with different stages of chronic inflammation in the fundic mucosa.
The method of staining clinical gastric biopsies from the gastric corpus with toluidine blue has several advantages: (i) it is cheap, (ii) quick to perform (sections are stained in only 30 seconds), (iii) toluidine blue is commonly available in all pathology laboratories, (iv) the interpretation of the aforementioned three modality groups is unsophisticated, and (v) it improves the detection of Helicobacter pylori (20).
Toluidine blue stain has been used to diagnose Helicobacter pylori infection in gastric biopsies in the Author's laboratory since the beginning of 2010. Accordingly, archival toluidine blue-stained sections will be reviewed aiming to investigate the state of the chief cell zone in a larger cohort of biopsies from patients with various gastric disorders.
- Received October 14, 2010.
- Revision received November 4, 2010.
- Accepted November 5, 2010.
- Copyright © 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}
{kind=link}