


Abstract
Background/Aim: Fractal dimension (FD) is widely used in medicine and biology as a tool for defining features of structure. This study aimed to compare pathological endometrium (simple-complex hyperplasia and endometrial carcinoma), as well as the endometrial changes, during the phases of the menstrual cycle. The main goal was the objective measurement of fractal dimension and to refrain from subjective evaluation. Materials and Methods: Two thousand cases of endometrial tissue from patients who underwent dilatation and curettage (D&C) were reviewed. Out of these, 137 cases were eligible for the study. In each case, immunohistochemistry with cytokeratin Ae1/AE3 was performed in order to simplify the evaluation of the FD. Results: Endometria with carcinoma, simple or complex hyperplasia showed significant differences only in the immunohistochemically stained fractal dimensions. As expected, significant differences were also found between atrophic and secretory endometrium and carcinoma. Conclusion: FD is an objective, rapid and simple procedure for the differential diagnosis between complex hyperplasia and endometrial adenocarcinoma.
Benoit Mandelbrot in his book “The Fractal Geometry of Nature” (1) was the first to demonstrate a mathematical approach on geometry, necessary in studying natural phenomena, structures and processes, which, until then, could only be approached by means of Euclidian geometry.
Classic Euclidian geometry is based on specific shapes being analyzed with simple equations, such as the surface area of a circle (πr2). However, the complex form of physical objects and living organisms could not be accurately investigated with Euclid's theorems only. For instance, the volume of a cloud cannot be calculated as a sum of spheres or the precise measurement of a coastal perimeter is practically impossible because, in every scale of a map, new details are depicted or revealed. The same applies to the limits of tissue or the periphery of a cell as, even though a cell can be described, it does not in fact have the shape of a cube, cylinder or sphere (2).
The Euclidian dimensions (DE) are 0, 1, 2 and 3 (3 dimensional space) characterize objects (length, width and height describing volumes). A surface has two dimensions (length and width), a line has one dimension (length only), whereas a point or sum of points in space is nil dimensional (0-dimensional sets). Topological dimension (TD) regards the shape and form of objects in an essentially quantitative form. Topology studies the way an object can transform without failing to maintain its basic structural properties. A straight line can be modified in a curve and, then, in a crooked line with the intermediate shapes being topologically equivalent. Specific elements and properties of structures may remain unaltered through appropriate modifications – for instance, the void area of a shape remains hollow regardless to whether the shape will be subject to alteration due to tension or compression. The topological dimension of shape does not alter from its transformations (2).
Mandelbrot introduced the term fractal (from the Latin fractua) that means irregular but, also, from fractional (dissented) and fragmented (disintegrated), in order to describe temporary phenomena or phenomena of space that may be continuous but could not be evaluated as an abstract.
From the fractals theory emerged the need to redefine the meaning of dimension so as to include non-integer values along with the integer dimensions of TD and DE. In need of such definition arose the term of Fractal Dimension (FD), which presents main subdivisions all of which share the same characteristic of having non-integer values. Therefore, fractals present with their own dimension i.e. the fractal dimension that usually (not always) has greater value than TD but lesser than DE.
Many fractal dimensions have been described and some of which are: the Similarity Dimension (DS), the Divider Dimension (DD), the Hausdorff dimension (DH), the Box-counting Dimension (DB), the Correlation Dimension (DC), the Information Dimension (DI), the Pointwise Dimension (DP), the Average Pointwise Dimension (DP), as well as the Lyapunov Dimension (DL). All of the above dimensions are in fact fractal dimensions with non-integer value, which is a main feature of fractal objects.
The Box-counting Dimension DB is the exponent D in the equation N(δ)=δ−D; N is the minimum number of boxes with a δ diameter required to cover an object. In order to estimate the dimension of an object with a general size V* (length, surface, volume or fractal dimension) that does not equal one, the following equation applies:

The method of box counting enables the analysis of objects or images by breaking them into smaller box-shaped pieces, thus analyzing them in a smaller scale, much like zooming in or out using optical or computer based methods as observation details change with scale. Box counting algorithms are being applied to patterns in 1-, 2-, 3-dimensional spaces on images extracted from digital media. The investigation of the patterns constitutes the fractal analysis.
Box-counting Dimension DB is widely used in medicine and biology. The main purpose of its use arises from the capacity to introduce it in algorithms of electronic computers performing a great number of calculations.
Medical literature includes more than 500 article titles until today regarding the implementation of fractals in the study of the physiological structure of human organs, tissues or cells or, respectively, in pathological conditions. The assessment of the fractal structure of neoplasms (3-9) has led to histological and cytological studies for the diagnosis and differential diagnosis of neoplasms of the ovary (10), thyroid neoplasms (11), brain tumors (12, 13), of oral and head and neck cancer (14, 15), of the breast (16-19), laryngeal carcinomas (20) endometrial carcinomas (21), neoplasms of the uterine cervix (22, 23), of the lung (24, 25), cancer of the colon (26), of the kidneys (27), hepatocellular carcinomas (28), of molar pregnancy (29), of the skin (30), of tumoral mast cells in lymph nodes and bone marrow (31) in B lymphoblastic leukemia (32) and in prostatic carcinomas (33). In 2004, a study was published regarding endometrioid carcinomas' tissue with a limited number of cases (21). In 2012, accordingly, one study was published regarding the implementation of FD in endometrial tissue (34) and there have been no further published studies on the subject.
Materials and Methods
The aim of this work is to evaluate the use of FD in the differential diagnosis between complex endometrial hyperplasia and adenocarcinoma. In spite of the fact that cyclic endometrial changes or atrophic endometrium are easily diagnosed morphologically, sections from normal endometrial changes were included in our material in order to evaluate whether FD measurements would fluctuate according to the method of staining and to estimate whether values obtained from normal endometria could interfere in the diagnosis of endometrial pathology.
The hematoxylin and eosin (HE)-stained sections from 2000 patients who underwent dilatation and curettage between 2000 and 2004 at the Medical School of the University of Crete (Research program KA948) were reviewed. Sections comprising tissue, which was considered adequate for evaluation, were represented as follows: proliferative endometrium (32 cases), mid-secretory endometrium (36 cases), atrophic endometrium (14 cases), simple hyperplasia (20 cases), complex atypical hyperplasia (16 cases), low-grade endometrioid carcinoma (FIGO grade1-2) (19 cases), a total of 137 cases.
From each case, one representative paraffin block was selected and one 4-μm section was cut and stained immunohistochemically with pankeratin AE1-AE3 (liquid mouse monoclonal antibody Multi-Cytokeratin NCL-L-AE1/AE3, Dilution 1:200; Novocastra Leica Biosystems, Biodynamics S.A., Athens, Greece) in order to simplify the evaluation of the FD. Concurrently, digital images were obtained in order to standardize the program and to determine the appropriate combination of staining, magnification and optical field so as to obtain calculations and to apply the evaluation method of DB through the program's software. The measurement of the DB was completed in the total of the cases and the results were registered in 181 tables of the Excel program. The measurements were applied in both HE-stained and immunostained sections with the result of 688 values in total.
Methods of calculating FD. Image J logistics (https://imagej.nih.gov/ij/) was applied to calculate Fractal Dimension. After a demo application in a number of calculations, it was proven to be perfectly suitable. The box counting method was used in black/white images of histology sections. The software covers the image with consecutive reruns in squares (boxes) with the value δ spreading from 1, 2, 4, 8, 16, 32, 64, 128, 256 and 512 pixels. The numbers of “boxes” (N) of the above dimensions that cover completely the image are being counted and the values are applied to an equation for the calculation of the fractal dimension.
Statistical analysis. Analysis of variance (ANOVA) was performed for the statistical analysis of the samples. The ANOVA Field and Block differences of pathological endometrium are presented under the corresponding Tables I, II and III (Field Diff.) and Tables IV, V and VI (Block Diff.). Block differences were significant in cases where blocks were >2 (Tables for normal endometrium not shown).
Field differences of the hematoxylin & eosin staining (HE) and immunocytochemistry staining (IHC) for carcinomas.
Field differences of the hematoxylin & eosin staining (HE) and immunohistochemistry staining (IHC) for complex hyperplasia.
Field differences of the hematoxylin & eosin staining (HE) and immunohistochemistry staining (IHC) for simple hyperplasia.
Block differences of the hematoxylin & eosin staining (HE) and immunohistochemistry staining (IHC) for endometrial carcinoma.
Block differences of the hematoxylin & eosin staining (HE) and immunohistochemistry staining (IHC) for complex hyperplasia.
Block differences of the hematoxylin & eosin staining (HE) and immunohistochemistry staining (IHC) for simple hyperplasia.

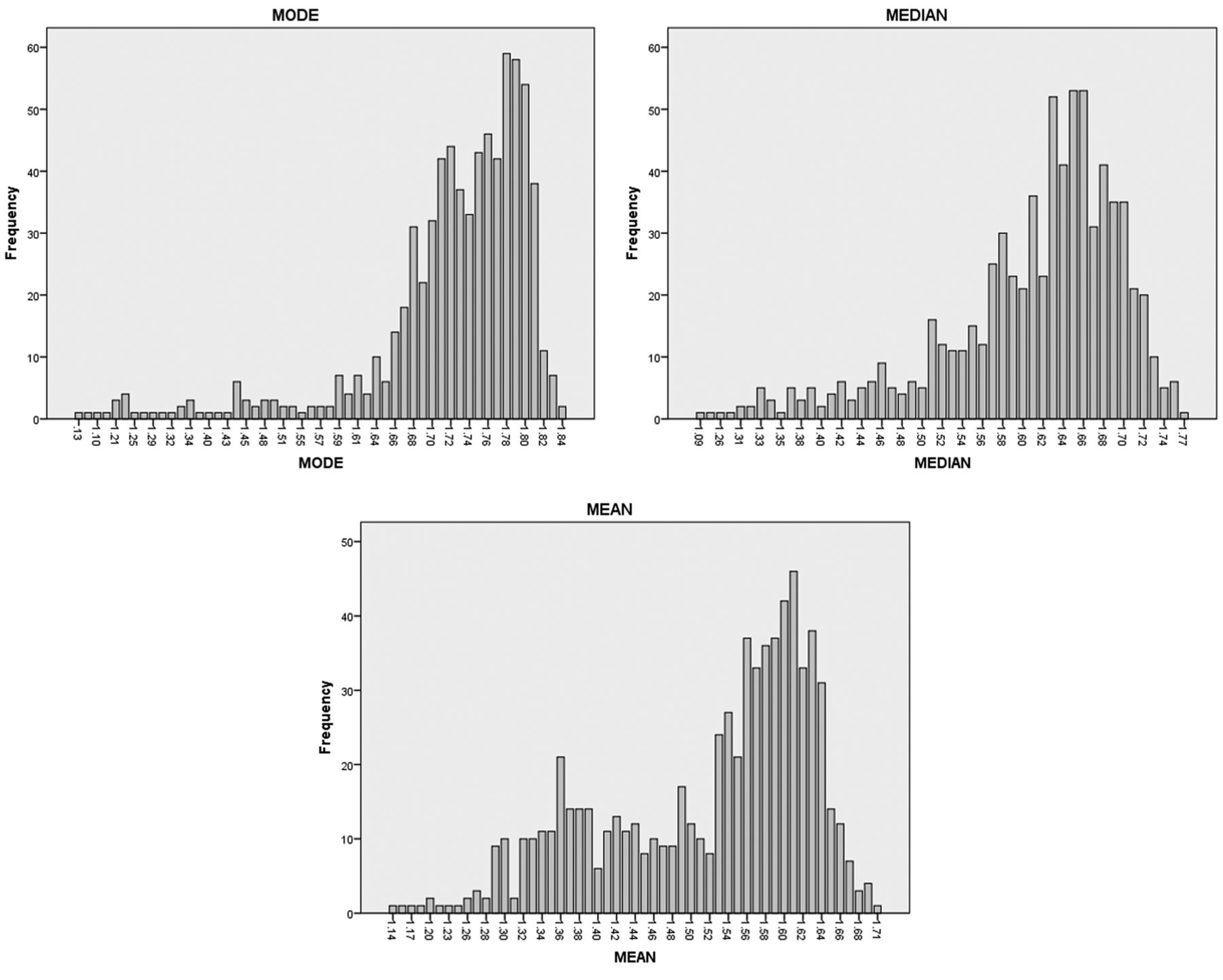
Distribution of mode, median and mean values. A different distribution of values is shown, suggesting that maximum values (mode) are significantly higher than the median and mean values, which are closer.
The distribution of mode, median and mean values are presented in Figure 1. A different distribution of values is shown, suggesting that maximum values (mode) are significant higher than the median and mean values, which are closer.
ANOVA of the analyzed fields in each slide did not show significant differences between the examined groups of lesions, either in HE or IHC staining (Figure 2). Therefore, for the subsequent analyses, we have grouped values of the two fields in each section and further analyzed these values. In complex hyperplasia and adenocarcinoma, no significant differences were found by ANOVA among the examined sections from blocks of each lesion. In cases of secretory and proliferative endometrium, there was a significant discrepancy among sections of the same patient (Figure 3). Therefore, since no differences were found in the aforementioned cases, we have grouped values from blocks and analyzed the means in each lesion.
Analysis of normal endometrium. In Figure 2, the Fractal Dimension in cases of secretory and proliferative phase is presented, together with cases of atrophic endometrium. All three modes, medians and means were compared (ANOVA Tables for normal endometrium not shown).
ANOVA analysis did not show a significant difference of modes, medians or means in HE-stained samples. In contrast, significant changes (ANOVA FD (2.78)=11.76, p<0.0001, Kruskal-Wallis p<0.0001) were found in modes of the three different endometria. However, neither medians nor means showed any statistical differences.
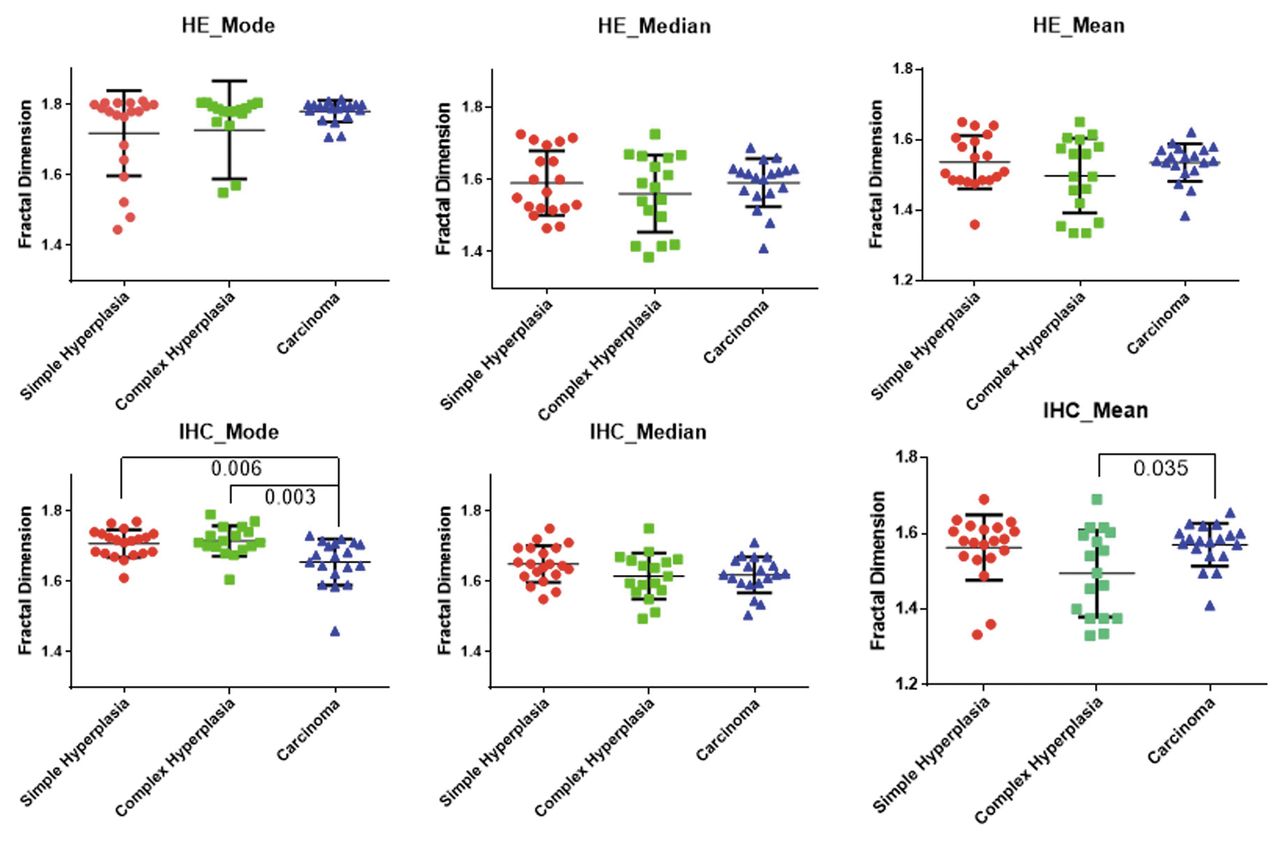
Analysis of endometrial lesions. Three lesions were investigated: simple and complex hyperplasia and adenocarcinoma (Figure 3; Tables VII, VIII). As a general finding, IHC gave more homogeneous results as compared to HE. Another interesting result was the discrepancy in Fractal Dimension changes between IHC and HE staining; for example, in cases of adenocarcinoma, mode and median values were increased in HE and decreased in IHC. Interestingly, a significant difference was found only in IHC fractal dimensions: mode values of hyperplasia (both simple and complex, which do not differ between them) and adenocarcinoma were significantly different, both in parametric ANOVA and non-parametric Kruskal-Wallis non-parametric test (p<0.003). Moreover, mean values (which do not represent a good representation of data, see Figure 1), present also a significant difference (although the fractal dimension seems increased in this case).

Analysis of normal endometrium. HE, hematoxylin & eosin; IHC, immunohistochemistry.
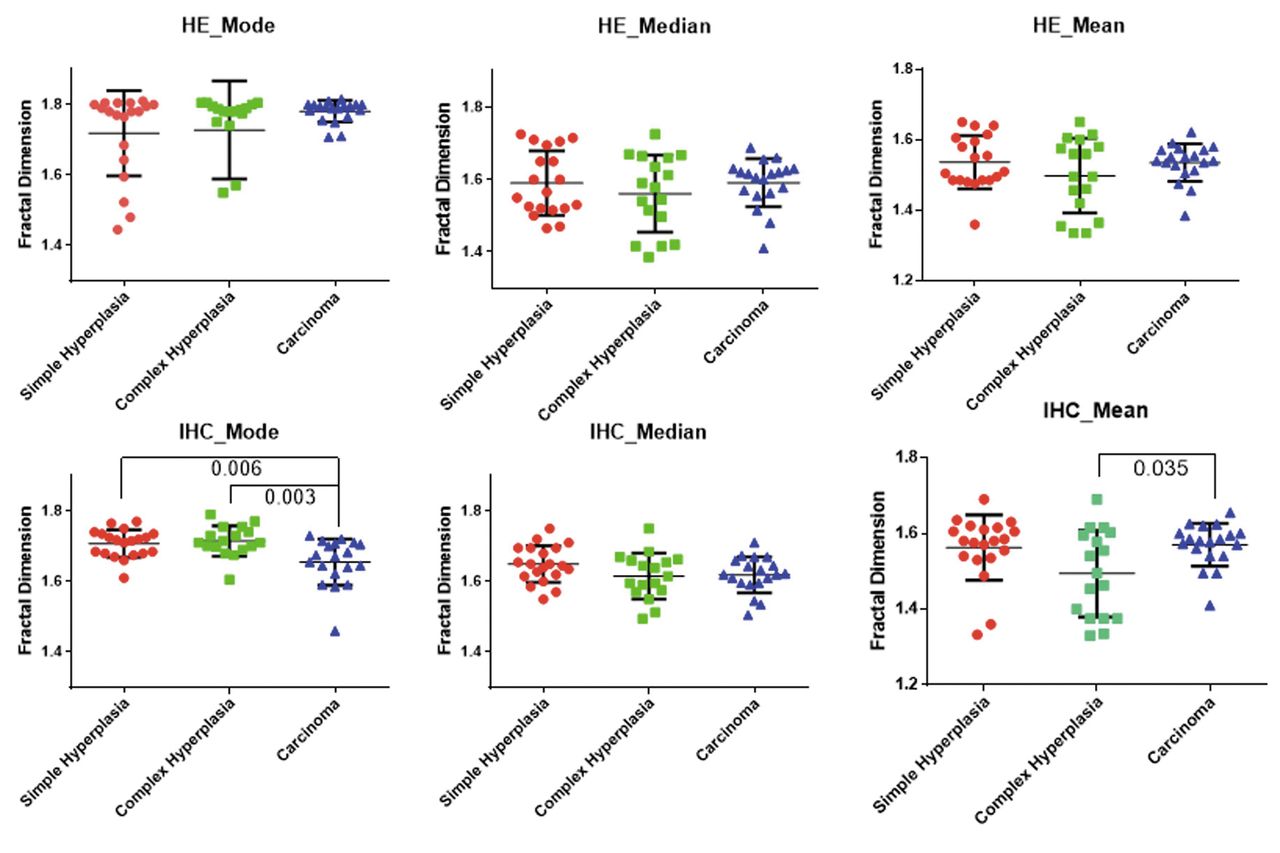
Analysis of pathological endometrium. HE, Hematoxylin & eosin; IHC, immunohistochemistry.
Hematoxylin & eosin staining (HE) of the pathological endometrium.
Immunocytochemistry staining (IHC) of the pathological endometrium.
Analysis of all histological appearances. Comparing all six groups, only mode (in IHC staining) showed a significant difference (FD (5,131)=9.06, p<0.0001, Kruskal-Wallis p<0.0001). Group comparisons revealed additional significant differences between atrophic and secretory epithelium and adenocarcinoma. From the statistical analysis presented it appears that measuring of FD can be of value in the differential diagnosis between complex hyperplasia and endometrial carcinoma.
Results
The modes, medians and means of all normal endometria in secretory, proliferative and atrophic phase were compared. The modes of HE-stained sections showed significant changes in all three normal endometria. Their medians and means, on the contrary, had insignificant differences. Pathological endometria with carcinoma and simple or complex hyperplasia showed a significant difference only in the IHC-stained fractal dimensions. Mode and median values demonstrated an increase in carcinoma in HE staining, whereas a decrease was marked in IHC.
Mode values of complex hyperplasia and carcinoma demonstrated significant differences. Within the 6 groups, only the mode in IHC demonstrated a significant difference. Moreover, significant differences were found between atrophic and secretory endometrium and carcinoma.
It appears that the contrast obtained by IHC staining, in the histological appearances, gives better results in the estimation of FD.
Discussion
Classification of endometrial hyperplasia as simple and complex with or without atypia, adopted by WHO in 1994, is based on the study by Kurman and colleagues (35) and is the one, even by 2015, most commonly used by pathologists (36). Atypical endometrial hyperplasia is the precursor lesion of endometrioid carcinoma that represents the majority of uterine malignancies (37). Diagnosis of complex atypical hyperplasia is based on the degree of gland architectural complexity, as well as the presence of nuclear atypia, features also distinguishing atypical endometrial hyperplasia from well-differentiated endometrial carcinoma (38). Nevertheless, the WHO classification is descriptive and diagnosis is subjective, while a poor reproducibility of the individual case classification has been reported (39, 40). It is, therefore, prone to over- or under-diagnostic errors that can lead to wrong therapeutic interventions with fatal results specifically in young women who wish to preserve fertility.
In 2003, the International Endometrial Collaborative Group (41) developed the endometrial intraepithelial neoplasia (EIN) diagnostic classification, which stands for the histopathologic presentation of a monoclonal endometrial “pre-cancer” (42, 43). Pathologic criteria were used to develop three categories: (i) benign (benign endometrial hyperplasia), (ii) premalignant (endometrial intraepithelial neoplasia), and (iii) malignant (endometrial adenocarcinoma, endometrioid type, well-differentiated).
In May 2015, the “Committee on Gynecologic Practice” of the “Society of Gynecologic Oncology” of the American College of Obstetricians and Gynecologists, suggested the use of EIN classification since “By applying the endometrial intraepithelial neoplasia schema to routinely obtained endometrial tissues, pathologists present the clinician with a disease-specific classification that informs treatment decisions” (36). Diagnosis using the EIN classification has been confirmed as prognostic in retrospective studies and one prospective study (44-47).
Yet, while helpful in identifying pre-cancers, the EIN classification should be used with caution since several times EIN lesions need to be distinguished from well-differentiated endometrial carcinomas. FD differs from these criteria by depicting the abnormal, irregular pattern of glandular architecture. Furthermore, the image analysis system by which it is calculated is an objective, automated method with minimal human interference.
Dey and Rajesh (21), in a pilot study, assessed ten cases each of endometrial simple hyperplasia (without atypia), complex hyperplasia with atypia and endometrial carcinoma (well-differentiated, endometrioid) in order to provide objective assessment of the measurement of glandular margin irregularities. Statistical analysis showed that the fractal dimension of glands of simple hyperplasia were significantly different from that of complex atypical hyperplasia and endometrial carcinoma. However, there was no significant difference in fractal dimension between glands of complex hyperplasia and of endometrial carcinoma. Nevertheless, they concluded that fractal dimension of gland margin may have diagnostic potential in the future.
Distinction between simple and complex atypical endometrial hyperplasia is objective and presents no diagnostic difficulties, in contrast to differential diagnosis between complex atypical endometrial hyperplasia and well-differentiated endometrial carcinoma.
Barwad and Dey (34) measured multifractal spectrum in thirteen cases of complex atypical hyperplasia and sixteen cases of well-differentiated endometrial adenocarcinoma. They concluded that multifractal dimension is significantly different between the examined groups. Yet, in multifractal analysis, the fractal dimension is not enough to describe the dynamics of a fractal system. A continuous spectrum of exponents is needed (48). Moreover the method requires application of complicated calculations and appears not useful as a routine diagnostic tool.
Our morphometric findings are in accordance with the findings presented by multifractal analysis by Barwad and Dey, a distinction not achieved by Dey and Rajesh (34, 21). Fractal dimensions of normal endometria in secretory, proliferative and atrophic phase were also compared and significant changes in all three normal endometria were found. There are no difficulties in the histological diagnosis of normal endometria but, as already stated, FD was applied for the comparison of the staining methods and the estimation of the interference in the evaluation of endometrial pathology.
Conclusion
The present study highlights the advantages of using FD, specifically in immunohistochemically-stained sections, for the differential diagnosis between complex atypical hyperplasia and endometrial adenocarcinoma.
Acknowledgements
The Authors thank Professor G.S. Delides for obtaining the material from research program KA 948 of the University of Crete Medical School, Department of Pathology, Heraklion, Crete, Greece.
- Received May 23, 2016.
- Revision received June 14, 2016.
- Accepted June 16, 2016.
- Copyright © 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.