


Abstract
Background: An evolution of CPH34 (CPH34 HV) for stapled transanal rectal resections was developed and tested to assess its safety and resection volume as compared to other staplers. Materials and Methods: A total of 16 pigs were randomly assigned to rectal prolapsectomy with CPH34 HV (n=4), CPH34 (n=4), PPH03-33 (n=4), HEEA (n=2) and PPH-01 (n=2). Measures and histological structure of specimens were assessed; transrectal echotomography (ETG) was performed on the third postoperative day, hence pigs were autopsied. Results: Significant differences of the volumes and weights of specimens were observed by type of stapler (p=0.0298 and p=0.0278, respectively) which were mainly due to CPH34 HV vs. PPH03-33 (p=0.0402 and p=0.0375, respectively). The average volumes were 17.1% lower for CPH34, 30.2% lower for HEEA, and 34.7% lower for PPH03-33 with respect to CPH34 HV. No significant increase of resection volume (7.5%) was observed between two PPH-01 units combined (two specimens together) vs. a single CPH34 HV unit. The highest percentage of muscularis propria was observed into the specimens collected with CPH34 HV and HEEA (50%). ETG detected three intra- and two extraparietal haematomata. Conclusion: The safety and higher volume of resection achievable with CPH34 HV correlated well with the specimen weight and percentage of muscularis propria.
Haemorrhoids and obstructed defaecation syndrome (ODS) are two of the most frequent diseases in the field of coloproctology. In the former, bleeding during or soon after evacuation, anal pain and/or discomfort and haemorrhoidal prolapse are the most common findings. ODS is an important clinical problem mainly affecting female patients with defaecation difficulty. These patients most frequently report a false sense of defaecation with failure, intense straining during defaecation and a feeling of incomplete evacuation. At times they are compelled to apply anal or vaginal digitation in order to complete defaecation. From the pathophysiological standpoint, ODS has been related to anatomical defects, such as internal rectal prolapse and/or rectocele, variably associated with functional alterations, such as paradoxical puborectalis contraction or spastic external sphincter contraction (1-7).
Several therapeutic approaches have been attempted but, unfortunately, most of them proved less than optimal, considering, for example, the painful postoperative course of patients undergoing haemorrhoidectomy or the unsatisfactory clinical outcome observed in patients with ODS, treated with traditional transvaginal and/or transanal surgical approaches (8-13).
According to the unitary theory of rectal prolapse, haemorrhoids and ODS share a specific pathophysiological feature which is represented by the internal rectal prolapse. It may be limited to the rectal mucosa (mucosal prolapse) but it may also involve the muscle wall (full-thickness rectal prolapse) (14). During defaecation, this internal prolapse may descend down to the anal canal, up to or even beyond the anal verge, thus pushing out anorectal mucosa and haemorrhoids. This dynamic prolapse over time weakens the supporting structures, such as Treitz's and Parks' ligaments, thus leading to haemorrhoidal prolapse primarily due to the internal rectoanal prolapse. By means of cinedefaecography (performed either radiologically or with magnetic resonance, MR), this internal prolapse has been shown to swell transversally, creating a rectocele and/or an intussusception causing a mechanically obstructed defaecation (5-7, 15). Moreover, rectal hyposensitivity (RH) has a definitive clinical impact in patients with infrequency of defaecation and/or obstructed defaecation symptoms, being reported with a prevalence of 23% as compared to 5% in patients without constipation (16, 17). RH may be even higher (29%) in patients with obstructed defaecation due to mechanical obstruction, such as rectocele and/or intussusceptions (16). This mechanical and functional obstruction causes straining during defaecation and the excessive efforts increase the pressure and the stress of pelvic muscles, fasciae and ligaments. The natural evolution of these structures is first a dynamic descent, followed by permanent perineal descent. In fact, these patients have a descending perineum syndrome first, followed by a firmly descended perineum.
Normal findings at transrectal echotomography (left) and autopsy (right).
Parietal haematoma at echotomography (left) with a diameter of 20 mm (arrow), confirmed at autopsy (right) shown as a circular haematoma with a diameter of 15 mm, in latero-dorsal position on the right.
From the clinical standpoint, symptoms of ODS are rather frequent in patients with internal rectal prolapse although they may be associated with bleeding, anal pain and/or discomfort, soiling and other typical symptoms of haemorrhoidal disease, all of them being related substantially to the extent and location (internal and/or external) of the rectal prolapse. Hence, patients with haemorrhoids and ODS share a continuity of symptoms which reflects the extent of the basic anatomo-functional alteration, which is the internal rectal prolapse. On these grounds, the surgical treatment of haemorrhoidal disease and ODS should be directed toward the correction of the internal rectal prolapse. This would allow not only a painless surgery but, most importantly, a pathophysiologically-driven correction of the rectal abnormality.
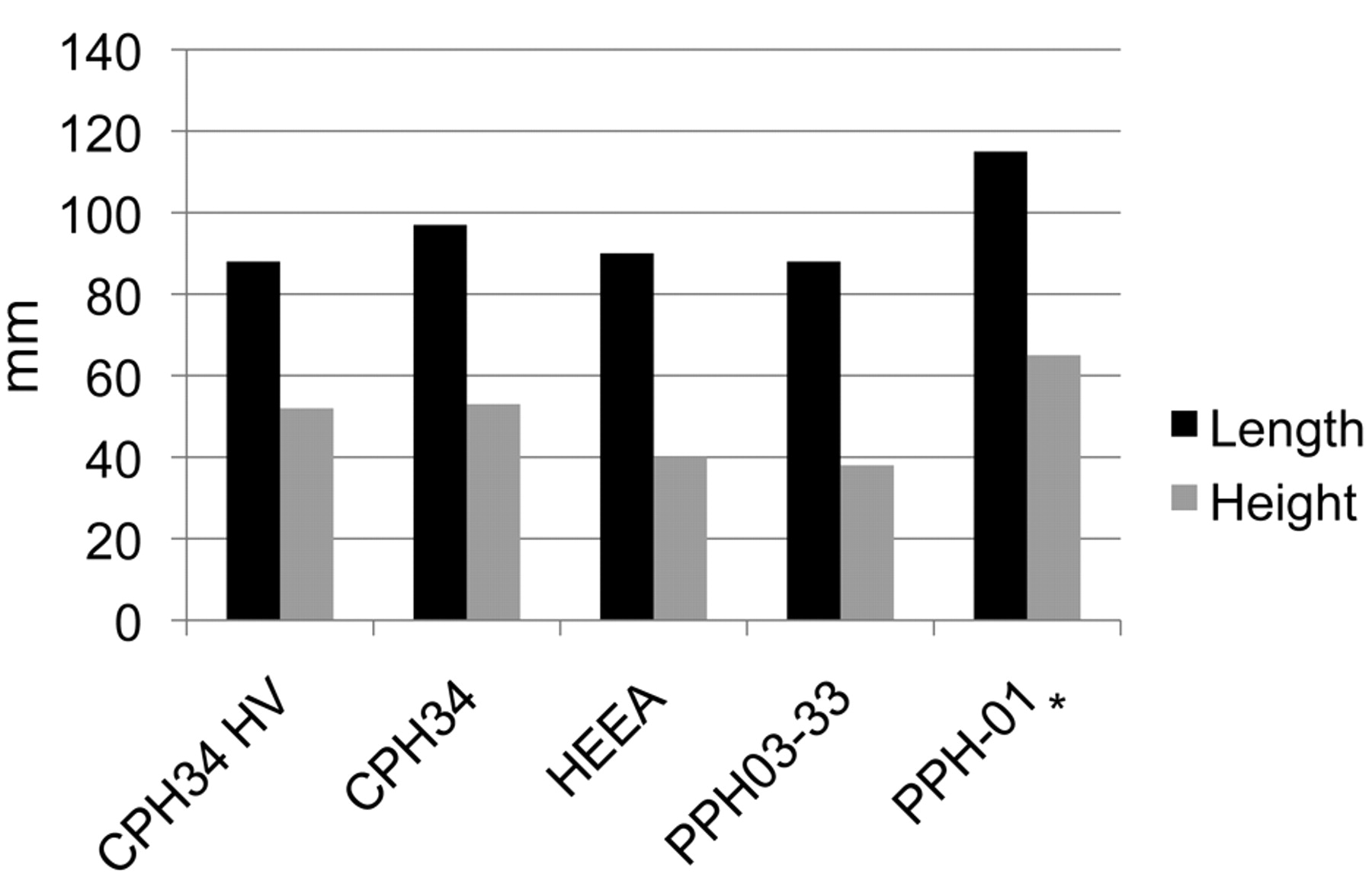
Measurements of the surgical specimens.
Currently, when a mucosal prolapse is found in patients with haemorrhoidal disease, a mucosal prolapsectomy (stapled anopexy) is performed by means of a circular stapler (18). In most cases, the resection also includes muscular fibres of the rectal wall, although it may not be regarded as a full-thickness rectal wall resection. Patients with specific symptoms of ODS, showing rectocele and/or rectal intussusceptions, usually undergo a stapled transanal rectal resection (STARR) procedure. This technique may remove a larger amount of internal/external rectal prolapse by means of two half purse-string sutures and, more recently, with the parachute technique, where two half purse-strings are performed with three separated stitches (one anterior and two lateral for the anterior prolapse, and one posterior and two lateral for the posterior one) (19, 20).
Nevertheless, currently available stapler devices pose some questions regarding the extent of rectal prolapse that may actually be resected and the possibility of performing the STARR procedure in a single step, using just one stapler. Recently, a new high volume (HV) stapler device has been developed with a stapler casing of CPH34 HV=22968.4 mm3, that should guarantee higher volumes of prolapse resection compared to currently available stapler devices. For this reason, an experimental study on pigs was performed in order to assess the safety of CPH34 HV and to compare the volume of resection obtained with CPH34 HV to that obtained by other stapler devices such as CPH34, PPH03-33, PPH-01 and HEEA.
Materials and Methods
A total of 16 pigs (mean weight, 40 kg; standard deviation (SD), 1.5 kg) were selected to undergo a stapled transanal rectal resection at the Experimental Center of Vila do Conde (Centro de Cirurgia Experimental Avancada, Portugal). They were randomly assigned to rectal prolapsectomy with PPH03-33 (Ethicon Endo-Surgery, Inc., Rome, Italy) in four cases, CPH34 (Chex Surgical Staplers; Frankenman International Limited, Hong Kong) in four cases, CPH34 HV (Chex Surgical Staplers) in four cases, HEEA (Covidien; Tyco Healthcare Group LP, Norwalk, CT, USA) in two cases and PPH-01 (Ethicon Endo-Surgery, Inc.) in two cases, performing an anterior and posterior rectal resection using two stapler devices in one procedure. The stapler casing or tissue storing volume was calculated and gave the following measures: 22968 mm3 for CPH34 HV, 20607 mm3 for CHP34, 22500 mm3 for HEEA and 15524 mm3 for PPH03-33 and PPH-01.
The pigs were monitored for three days before autopsy in order to detect early and delayed postoperative complications such as suture bleeding, intraparietal or extra-wall haematoma, suture dehiscence, pelvic infection and damage to surrounding organs. In each case, the length, height, weight, and volume of the resected specimen were determined by the same examiner; the volume was calculated using a graduated ampulla filled with saline solution, by measuring the volume increase when the surgical specimen was put into the ampulla. A histological examination was blindly performed regarding the type of stapler used, and the pathologist also calculated the percentage of mucosa, submucosa and muscularis propria within the surgical specimen. Moreover, transrectal echotomography (ETG) was performed on the third postoperative day to check for the development of extrarectal haematoma or surrounding organ damage (Figure 1 and 2). The study protocol was submitted and approved by the Ethics Committee of the Institution.

Length and height of resected specimens by type of stapler. *Two specimens together.
Stapled transanal rectal resection. Surgery was performed under general anaesthesia, with the pig placed in a lithotomy position. Controlled digital stretching was performed initially with two fingers (index fingers) introduced carefully inside the anus, to perform a moderate traction laterally (gradually separating the two index fingers) and in an anteroposterior direction, in order to ease the introduction of the circular anal dilator (CAD) that was fixed with four silk stitches to keep it in place. Once the obturator was removed, the operative anoscope was inserted into the lumen of the CAD and a 2-0 Prolene purse-string suture was performed approximately 2 cm above the dentate line. The circular stapler was inserted fully open and the purse-string suture was secured to the central axis. The suture threads were then retrieved through the suture conduits positioned on either side of the head and secured in a manner to allow gentle digital pressure on the suture to draw the tissue into the stapler casing. When the HEEA stapler was used, the lowest anchor point (more proximal with respect to the surgeon) was selected on the central rod of the anvil and the purse-string was secured and knotted. The stapler was then fired in order to perform the prolapsectomy and rectopexy. Once the stapler was removed, the integrity of the mucosal cylinder removed (doughnut) was checked. After prolonged observation for five minutes to check that haemostasis was complete, an absorbable plug was placed in the anal canal. This concluded the intervention.
Statistical analysis. The comparison between the different types of staplers was performed using analysis of variance (ANOVA) with Scheffe internal comparisons and the non-parametric Kruskal-Wallis test. The differences between CPH34 HV and PPH1 were analysed using the unpaired Student's t-test. The level of significance was set at p=0.05. Statistical analysis was carried out with StatView (SAS Institute, Cary, NC, USA).

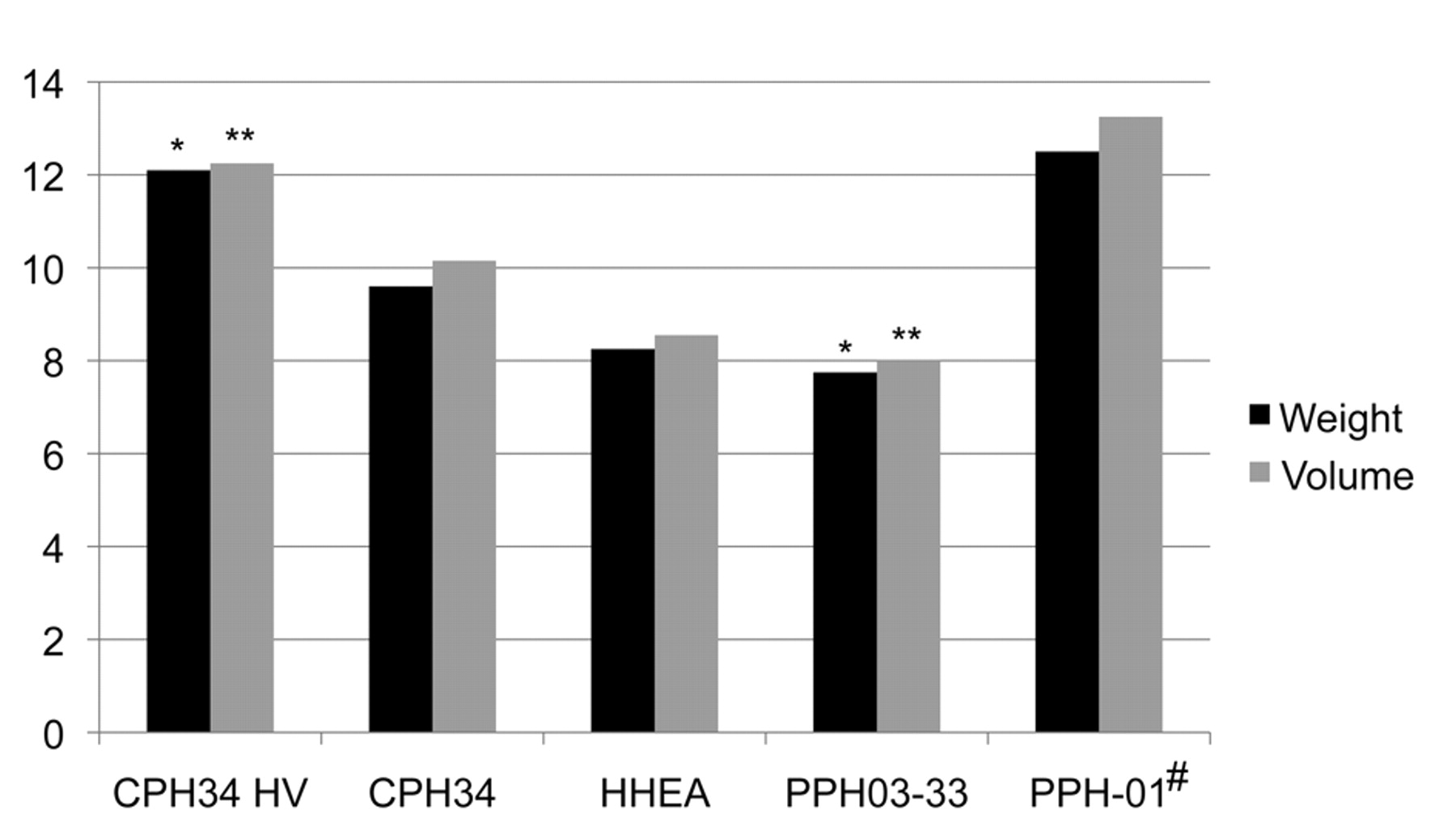
Weight (g) and volume (ml) of resected specimens by type of stapler. *p=0.0375; **p=0.0402 for CPH34 HV vs. PPH03-33; #two specimens together.
Results
The operations were always carried out by two surgeons (G.R. and T.T.) and the mean operative time was 20 min (standard deviation=2.5 min). The measurements of the surgical specimen are reported in Table I. Significant differences of the volumes and weights of the resected specimens were observed by type of stapler (p=0.0298 and p=0.0278 with ANOVA test, respectively, confirmed with non-parametric test). Notably, for both volume and weight, this observation was mainly due to the staplers CPH34 HV and PPH03-33 (by means of internal comparison: p=0.0402 and p=0.0375, respectively) (Figure 3 and 4).
The average volumes were 17.1% lower for CPH34, 30.2% lower for HEEA, and 34.7% lower for PPH03-33 with respect to CPH34 HV, with a relative differential increase ranging from 20% to 53%. No significant increase of the resection volume (7.5%) was observed between two PPH-01 (considering the two operative specimens together as if used in conventional STARR) vs. a single CPH34 HV. Moreover, CPH34 allowed resection volume increases of 15.7% compared to HEEA and 21.1% compared to PPH03-33. Finally, HEEA gave a resection volume increase of 6% compared to PPH03-33.
With regard to the histological examination, the surgical specimens were always represented by normal anorectal wall, including mucosa, submucosa and muscularis propria, whose percentages are reported in Table II. The highest percentage of muscularis propria was observed into the surgical specimens collected with CPH34 HV and HEEA (50%), followed by CPH34 (47.5%), and PPH03-33 and PPH-01 (45%).
No intraoperative or early postoperative complications occurred. Transrectal ETG detected three intraparietal haematomas ranging from 3 to 15 mm (one with each of CPH34 HV, PPH03-33 and PPH-01) and two extrarectal haematomas (one with each of CPH34 and HEEA) which were always confirmed at autopsy.
Percentage of mucosa, submucosa and muscularis propria within the surgical specimen by type of stapler.
Discussion
In the last decade, the role of rectal prolapse in the pathogenesis of haemorrhoids and ODS has received sound clinical and experimental validation. In fact, patients with haemorrhoids usually present typical vascular signs, such as bleeding, thrombosis, oedema, strangulation and necrosis, which may be associated with various symptoms of obstructed defaecation (such as straining, incomplete and extended evacuation time, painful evacuation efforts, digital assistance and evacuation failure) or even of incontinence (such as moist anus, soiling, dermatitis, itching, perineal discomfort or pain and faecal incontinence) due to the type (mucosal or full-thickness) and extent (internal and/or external) of rectal prolapse. For these reasons, stapled anopexy is not only associated with less postoperative pain and earlier return to normal activity than conventional haemorrhoidectomy but it may also significantly improve outlet obstruction symptoms thanks to the correction of rectal prolapse (21).
Certainly, the risk of recurrence is strictly related to an effective correction of rectal prolapse, as demonstrated by Boccasanta et al. (24), because, whenever the extent of prolapse exceeds the real volume of resectable tissue, there is a significant risk of residual disease at the end of the operation. Surprisingly, currently available staplers, such as PPH03-33, notwithstanding a stapler casing volume of 15.5 cm3, allow resection of a smaller tissue volume because the prolapsed tissue is patched up by the purse-string and the stapler casing is not a perfect cylinder (22). Moreover, only when the patient is under anaesthesia, may the real extent of rectal prolapse be appreciated, thanks to the relaxation of anal sphincters, thus allowing the definition of the real extent of prolapse resection that is required. For these reasons, the availability of a stapler device with a higher volume stapler casing may allow a more appropriate resection of the rectal prolapse, avoiding the use of two staplers in many cases.
The experimental findings of the present study suggested that CPH34 HV increased the volume of rectal wall resection from 20% to 53% compared to currently available staplers. Notably, if one considers just the superficial measures, such as the dimensions of the surgical specimens, these are almost the same irrespective of the type of stapler adopted, because they are essentially determined by the anatomical conformation of the anorectum more than the stapler features. Conversely, the higher the volume of the tissue storing area, the higher the weight, the volume and the thickness of the surgical specimen will be. This represents a remarkable piece of evidence lacking in most of published clinical trials because very rarely and exclusively after the STARR procedure, the dimensions of the surgical specimens are reported (19, 20, 23-25).
The larger resection volume obtained with CPH34 HV is well confirmed also by the corresponding weight of the specimens and their percentage of muscularis propria (50%) compared to the specimens of rectal resection collected with the other types of staplers (CPH34, PPH03-33, and PPH-01) ranging from 47.5% down to 45%. In any case, a thick muscular layer was observed in each surgical specimen so that the description of operation (namely, transanal rectal resection) fitted well with the histological findings. It should be noted that notwithstanding this rather deep and large rectal resection, no serious intra- or postoperative complications occurred, there being no damage to surrounding organs as observed by both transrectal ETG and autopsy, thus confirming the overall safety of the procedure.
Another important finding of this experimental study was the observation that in pigs undergoing STARR there was only a small and non-significant difference between the volume obtained with a single stapler (CPH34 HV) and the overall resection volume obtained with two staplers (PPH-01). This means that a single stapler may remove a large enough amount of tissue in patients undergoing stapled anopexy who are bearing a full-thickness rectal prolapse, which usually exceeds half the volume of CAD, and in patients undergoing STARR for ODS 25.
Conclusion
The results of this experimental study confirmed the safety and the higher volume of resection achievable with CPH34 HV, with an increase of the volume of rectal wall resection ranging from 20% to 53% compared to other currently available staplers. The higher volume of resection obtained with CPH34 HV correlated well with the corresponding weight of the specimens and their percentage of muscularis propria. Hence, notwithstanding the similar square surface, CPH34 HV guaranteed a thicker specimen of resection compared to the other types of stapler. As the weight and volume provide better information regarding the extent of prolapse resection compared to the resection dimensions (length and height), these parameters should always be collected when assessing the quality of resection and the efficacy of stapled anopexy or STARR procedures.
With regard to the STARR procedure, the negligible difference that was observed between the volume of resection with a single CHP34 HV and two PPH-01 confirms the possibility of performing a cheaper and easier operation with a single CPH34 HV. As a matter of fact, thanks to the higher volume of resection this new device is able to achieve, current differentiation between stapled anopexy and STARR procedures may be overcome by performing a tailored rectal resection with a single stapler, based on the intraoperative assessment of the type of prolapse; either mucosal prolapse, usually not exceeding half the volume of CAD, as frequently occurs in patients with symptomatic haemorrhoids, or full-thickness rectal prolapse, exceeding half the volume of CAD, as typically found in ODS patients, with or without haemorrhoidal disease. Such a hypothesis may be confirmed in an ongoing multicentre randomised controlled clinical trial comparing current standard of resection (stapled anopexy with PPH03-33, and STARR with two PPH-01) with prolapse resection by means of a single CPH34 HV.
- Received October 7, 2010.
- Revision received November 12, 2010.
- Accepted November 16, 2010.
- Copyright © 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}