


Abstract
Background/Aim: The present study examined the utility of serum p53 antibody (Ab) for detecting colitis-associated cancer (CAC) in the era of immunosuppressive therapy. Patients and Methods: Two hundred and fifty patients were analyzed, 219 had no carcinoma or dysplasia (Group non-CAC), and 31 had carcinoma or dysplasia (Group CAC). Serum p53 Abs were detected with an enzyme-linked immunosorbent assay. Immunohistochemical detection was performed in Group CAC. Results: Immunosuppressive therapy was performed in 98.1% of Group non-CAC and 80.6% of Group CAC. There were no differences in serum p53 Abs positivity between Groups non-CAC and CAC (8.7% vs. 3.2%, p=0.30). p53 staining positivity was noted in 90.3% of Group CAC, and the rate of serum p53 positivity was significantly lower in patients with immunosuppressive therapy than in those without in Group CAC (0.0% vs. 16.7%, p=0.04). Conclusion: The utility of serum p53 Ab for detecting CAC is dubious in the era of immunosuppressive therapy.
Mutations in the p53 tumor suppressor gene are the most frequently reported somatic gene alterations in human cancer (1, 2). In the ulcerative colitis (UC)-associated dysplasia-carcinoma sequence, p53 gene mutations are early events compared to adenomas related to the typical adenoma-carcinoma sequence (3). Mutations in the p53 gene are observed in 50%-85% of colonic tissue specimens of UC with dysplasia or colorectal cancer (4). These mutations result in the accumulation of the p53 protein, which causes p53 overexpression in tissue. There have been many reports of p53 overexpression in cases of ulcerative colitis-associated colorectal cancer (CAC) (5).
Apart from the detection of p53 gene mutations and p53 overexpression associated with CAC, in the 1990's it was reported that serum anti-p53 antibodies are detected as serum IgG antibodies that are present due to an antigen-antibody reaction to p53 protein. The usefulness of measuring serum anti-p53 Antibodies (Abs) in various malignant tumors has been suggested (6-9). Compared to conventional tumor markers, anti-p53 Abs is useful for detecting early colorectal cancer (10-12). Yoshizawa et al. reported the usefulness of measuring serum anti-p53 Abs in CAC in 2007 (13), which constituted this assessment eligible for health insurance coverage in Japan during that same year.
Interestingly, since the spread of immunosuppressive therapy for UC treatment in the 2010s, we have experienced a low prevalence of anti-p53 Abs in UC patients with CAC. To our knowledge, no data are available in the literature concerning the usefulness of serum p53 Abs for CAC since immunosuppressive therapy became common for UC treatment. The present study therefore explored whether serum p53 Abs are useful for detecting CAC in the era of immunosuppressive therapy.
Patients and Methods
Study population. From April 2008 to March 2019, 320 consecutive patients who underwent surgical resection for UC were collected from the Yokohama City University Medical Center in Japan. The exclusion criterion was no data on serum anti-p53 Abs before the operation. A total of 250 patients were analyzed in this study. We divided the patients into two groups: i) group non-CAC included patients who underwent surgery for severe or intractable colitis and had not been diagnosed with carcinoma or dysplasia histologically by a biopsy or surgical specimen, and ii) group CAC included patients who had been diagnosed with carcinoma or dysplasia. Of these 250 UC patients, 219 (87.6%) were in Group non-CAC, and 31 (12.4%) were in group CAC (Figure 1). The history of other cancers, smoking and family history of colorectal cancer were reviewed. The clinicopathological features of UC, such as age at time of operation, duration of disease, extension of disease and medications, were collected from the medical records.
An enzyme-linked immunosorbent assay (ELISA) for Anti-p53 Abs and conventional tumor makers. An ELISA for the detection of anti-p53 Abs in serum was carried out with a commercially available ELISA kit (MESACUP anti-p53 test; Medical & Biological Laboratories, Nagoya, Japan). In brief, serum samples and calibrators were added to each well of a 96-well microtiter plate coated with wild-type human p53 or control protein. Samples were incubated on the plate for 60 min (20-30°C). After washing, peroxidase-conjugated anti-human IgG anti-p53 Abs were added, followed by further incubation for another 60 min (20-30°C). After washing again, the substrate was added, and the plate was incubated again for 30 min (20-30°C). A stop solution was then added to each well to stabilize the color development. The value in each sample was determined by comparing the optical density of the sample to that of the anti-p53 standard. The cut-off value was 1.3 U/ml, according to a previous colorectal cancer study (11, 14). The carcinoembryonic antigen (CEA) levels were measured using a CEA-2 enzyme immune assay (EIA) kit (Elecsys CEAII; Roche Diagnostics K.K., Tokyo, Japan), following the manufacturer's instructions with a cut-off value of 5.0 ng/ml. The cancer antigen 19-9 (CA19-9) levels were measured using a CA19-9 EIA kit (Elecsys CA19-9; Roche Diagnostics K.K.) with a cut-off value of 37 U/ml.
Immunohistochemistry. For patients with dysplasia or CRC by colonoscopy, we also evaluated the p53 status using immunohistochemistry on biopsied or surgical specimens. In brief, paraffin-embedded tissue samples were cut in serial sections of 3-4 μm thickness, placed on coated slides and deparaffinized through a series of xylene and ethanol baths. The slides were then incubated with anti-p53 primary antibodies (DO-7; DAKO, Glostrup, Denmark), followed by biotin-conjugated goat antibody against mouse as a secondary antibody (E0433; DAKO). The following steps were performed using a standard ABC method (Elite ABC kit, Vectastain; Vector Laboratories, Burlingame, CA, USA): 3,3-Diaminobenzidine was used as substrate for the peroxidase enzyme reaction (Vectastain; Vector Laboratories), and all slides were counterstained with hematoxylin and observed under a microscope (CH40; Olympus, Tokyo, Japan).
Immunosuppressive therapy. In this study, we defined immunosuppressive therapy as one offered to patient with a medical history of i) prednisolone administration exceeding 20 mg per day for the equivalent of 2 weeks or more, ii) immunosuppressant drugs (including cyclosporine and tacrolimus), iii) immunomodulator drugs (including 6-mercaptopurine, azathioprine and methotrexate) or iv) biologic therapies (including infliximab and adalimumab) for UC treatment. According to a previous report, these therapies induce an immunocompromised state in inflammatory bowel disease patients (15).
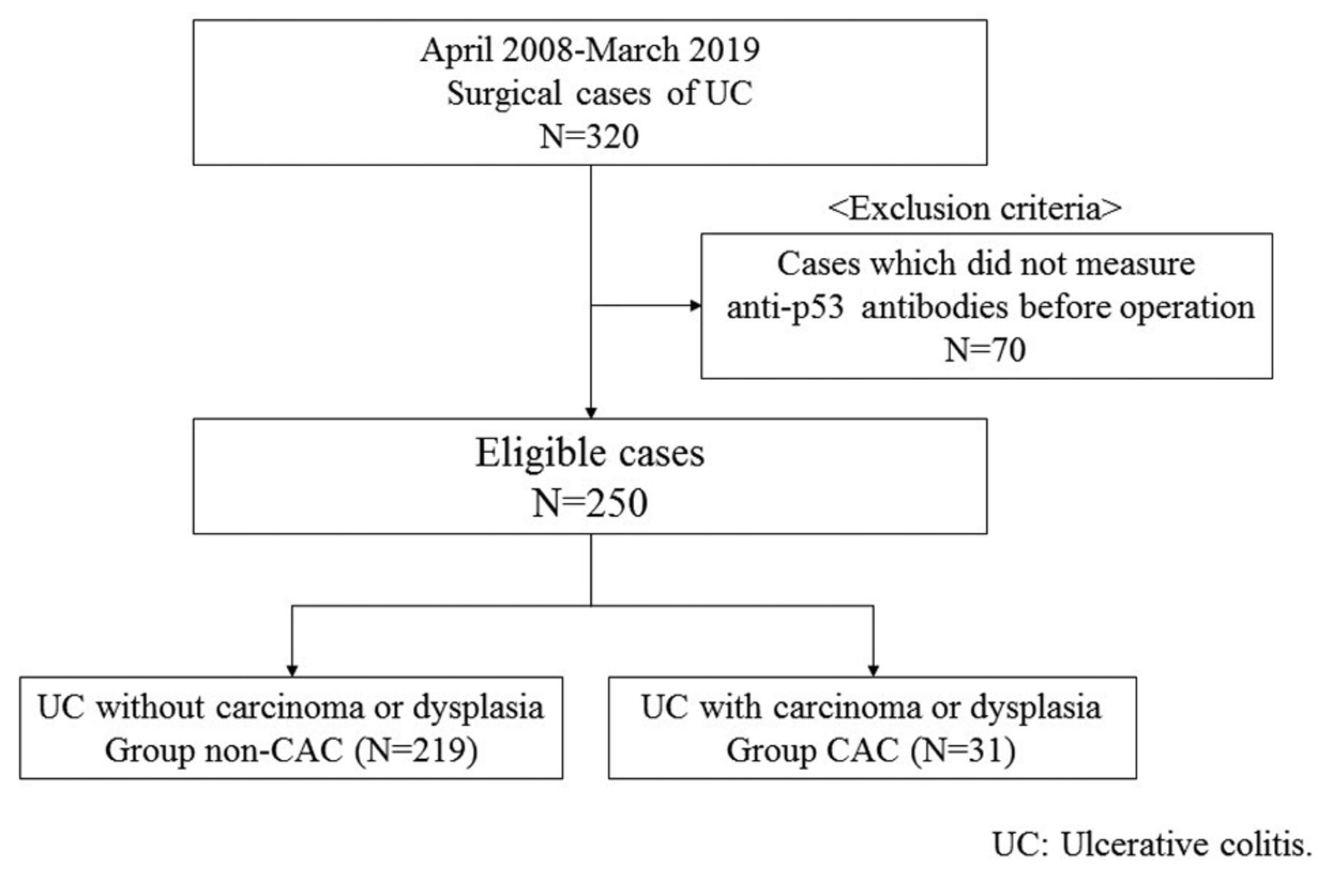
Outline of patient selection.
Statistical analyses. Differences between categorical variables were tested using Pearson's chi-squared test, and differences between continuous variables were tested using the Mann-Whitney U-test. Statistical analyses were performed using the SPSS statistical software program, version 22.0 (SPSS Inc., Chicago, IL, USA). All tests were 2-sided, and p-Values less than 0.05 were considered statistically significant.
Results
Serum anti-p53 Abs and the clinicopathological features of the study population. The demographic and biochemical characteristics of the subjects in all studied groups are shown in Table I. There were no significant differences in the positivity of serum anti-p53 Abs between Group non-CAC and Group CAC (8.7% vs. 3.2%, p=0.30). The age at the time of operation in Group non-CAC was lower compared to that of Group CAC (40 years vs. 50 years, p=0.02). The duration of the disease differed significantly between Group non-CAC and Group CAC (6 years vs. 17 years, p=0.01), and patients with >8 years since the UC onset were less frequent in Group non-CAC compared to Group CAC (25.1% vs. 87.1%, p<0.01). Immunosuppressive therapy was performed in 98.1% of Group non-CAC and 80.6% of Group CAC.
There were no significant differences between the groups in the gender, age at UC onset, disease extent, history of other cancer, smoking, family history of CRC, serum CEA or serum CA19-9.
Serum anti-p53 Abs and tissue p53 overexpression in Group CAC. The serum anti-p53 Abs and tissue p53 overexpression in Group CAC are shown in Table II. p53 overexpression in tumor tissue was noted in 90.3% of Group CAC. Both serum anti-p53 Abs and tissue p53 overexpression were positive only in Patient 3, who was diagnosed with CRC and did not undergo immunosuppressive therapy.
Characteristics of the study population.
Association between anti-p53 Abs and immunosuppressive therapy. The association between anti-p53 Abs and immunosuppressive therapy is shown in Table III. The rate of positivity for anti-p53 Abs was significantly lower in those who underwent immunosuppressive therapy before their operation compared to those who did not undergo immunosuppressive therapy before their operation in Group CAC (0.0% vs. 16.7%, p=0.04).
Discussion
We analyzed a total 250 UC patients, including 31 patients with carcinoma or dysplasia. The rate of positivity for serum anti-p53 Abs was only 3.2% in patients with carcinoma or dysplasia and 8.7% in those without carcinoma or dysplasia. Our study clarified that serum anti-p53 Abs measurement does not aid in the detection of CAC.
Lu et al. have shown in their meta-analysis that p53 expression was positive in cases of UC associated with carcinoma and dysplasia (5). The frequency of anti-p53 Abs in patients with tumors is strictly correlated with the frequency of p53 mutations (16). There is generally a good correlation between the presence of anti-p53 Abs and the p53 accumulation and/or mutations in a tumor (17). Previous studies have reported that the presence of anti-p53 Abs in UC with carcinoma or dysplasia was significantly more frequent than in UC without carcinoma or dysplasia (40.0%-61.5% vs. 12.8%-13.3%) (17, 18). Therefore, measuring anti-p53 Abs may aid in the early detection of carcinoma or dysplasia in UC patients.
In the present study, the p53 expression was positive in 90.3% of UC patients with carcinoma or dysplasia, however, anti-p53 Abs was positive in only 3.2% of UC patients with carcinoma or dysplasia. The rate of p53 overexpression was, thus, high in tumors despite a low prevalence of serum anti-p53 Abs in UC with carcinoma or dysplasia. Some reports have demonstrated the high rate of p53 mutations in tumors and the low prevalence of anti-p53 Abs (19, 20). One factor associated with this observation is the immunological malformation that may influence the production of anti-p53 Abs in patients with p53 mutant tumors (20). Over the past decade, UC patients have tended to develop immunological malformation because immunosuppressive therapy has been used more frequently and earlier during the course of the disease to treat UC (21). In addition to steroid therapy, immunomodulatory and immunosuppressant drugs and biologic therapy [specifically anti-tumor necrosis factor (anti-TNF)] have been key to the treatment of UC, as the efficacy of immunomodulatory drugs for UC maintenance therapy is reported since 2012 (22), and that of biological therapies since 2011 (23).
Clinicopathological characteristics of ulcerative colitis with cancer or dysplasia.
Some reports have suggested that immunosuppressive therapy might induce a low antibody response rate to various vaccines, because immunosuppressive therapy during multiple steps of the inflammation cytokine cascade (21, 24-26). We considered that the low prevalence of anti-p53 Abs might be caused by a low antibody response to p53 protein induced by the immunosuppressive therapy in UC patients, as the positivity for anti-p53 Abs was significantly lower in UC patients with cancer or dysplasia with immunosuppressive therapy compared to those without.
Several limitations associated with the present study warrant mention. First, some cases did not have anti-p53 Abs measured before the operation, particularly emergency surgery cases. We therefore excluded these cases from this study. Second, this was a small-scale single-institutional study, wholly comprising Japanese patients. A large-scale multi-institutional study is, thus, needed.
Association between anti-p53 antibodies and immunosuppressive therapy.
In conclusion, there was no marked difference in the serum anti-p53 Abs between UC cases with carcinoma or dysplasia and those without. Serum p53 Abs were not associated with p53 immunoreactivity in CAC patients with immune-suppressive therapy. The usefulness of serum p53 Abs in detecting CAC is dubious in the era of immunosuppressive therapy.
Acknowledgements
None.
Footnotes
Authors' Contributions
KT and HK contributed to the study design. All Authors contributed to the data collection, data analysis, and interpretation. KT and HK contributed to the statistical analyses. All Authors contributed to the writing or review of the report and approved the final version.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no conflicts of interest for this work.
- Received November 7, 2019.
- Revision received November 16, 2019.
- Accepted November 26, 2019.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.