


Abstract
Background/Aim: The purpose of this retrospective study was to describe the benefits and risks of a diverting stoma (DS) in laparoscopic low anterior resection (LAR) for rectal cancer. Materials and Methods: A total of 140 and 167 patients without and with DS, respectively, were included in this study in a high-volume cancer center of Japan within an 8-year period. Results: Small bowel obstruction occurred more frequently in patients with DS (2.86% vs. 16.17%, p<0.001). The difference in anastomotic leakage rate was not statistically significant (11.43% vs. 10.18%, p=0.72). In multivariate analysis, the operating time was associated with a higher rate of leakage in LAR [odds ratio (OR) 8.772, 95% confidence interval (CI)=1.002–1.012, p=0.027]. Conclusion: Operating time was associated with a higher rate of leakage in LAR for low rectal cancer. A DS did not reduce anastomotic leakage but increased the risk of postoperative intestinal obstruction in laparoscopic LAR.
Laparoscopic lower anterior resection (LAR) is an effective treatment for low rectal cancer. It can overcome the limitation of a narrow pelvis, thereby improving the quality of the procedure (1). The most dreaded and destructive complication of LAR is anastomotic leakage, reported to be as high as 20% (2, 3) and is associated with morbidity and mortality (4).
It has been shown that male patients, or those with a previous history of pelvic radiotherapy, low tumor and low pelvic colorectal anastomosis rates, have a higher risk of anastomotic leakage (5, 6). Therefore, a diverting stoma (DS) is recommended for such high-risk patients (7). Although a DS may be of potential benefit to patients undergoing an anterior resection, stoma-related complications can also occur. These range from mild to devastating, with some patients requiring reoperation and long-term inpatient care, meaning a DS remains a controversial procedure (8-12).
A double stapler technique (DST) combined with a circular stapler is currently the most commonly feasible method for LAR anastomosis. However, anastomotic leakage often occurs at the overlap of the anastomotic staples (13). Therefore, some hospitals use a side-stapling technique (14).
The purpose of this retrospective study was to describe the benefits and risks of a DS in laparoscopic LAR for low rectal cancer with a side-to-end stapling anastomosis technique.
Patients and Methods
In this study, we retrospectively analyzed a total of 307 patients with low rectal cancer who underwent LAR with curative intent at the Division of Gastroenterological Surgery of Saitama Medical University from April 2007 to December 2015. LAR is defined as having an anastomotic site below the peritoneal reflection.
Laparoscopic LAR exclusion criteria were: 1) patient-related factors such as severe cardiopulmonary disease and other laparoscopic surgery contraindications; and 2) tumor-related factors such as obstructive tumors and intestinal perforation.
Operating procedures were as follows: After a total mesorectal resection or tumor-specific mesorectal resection of the lower rectum, the rectum was cut, and a transumbilical incision was made from which the proximal colon and rectum, together with the tumor, were exteriorized. After the proximal end was transected with cutting staplers, the staple line was buried with polydioxanone sutures. A circular stapler anvil was then inserted through a small colotomy on the contralateral side of the mesocolon and secured by a purse-string suture. A 25-mm intraluminal stapler (CDH 25, Ethicon Endo-Surgery, Cincinnati, OH, USA) was used for the anastomosis.
All patients were followed up regularly according to the Japanese Guidelines for Diagnosis and Treatment of Colorectal Cancer. All retrospective cohort studies were reviewed by the institutional ethics review board and published on the hospital's home page.
Patients' basic demographic data and clinical characteristics including gender, age, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, tumor size, preoperative carcinoembryonic antigen (CEA), depth of infiltration, postoperative morbidity and mortality, leakage of anastomosis and incidence of postoperative complications were investigated from medical records.
Rectal rectosigmoid (RS), rectum above the peritoneal reflection (Ra) and rectum below the peritoneal reflection (Rb) were defined according Japanese colorectal cancer statutes with preoperative computed tomography (CT) or magnetic resonance imaging examination.
According to Japanese colorectal cancer statutes, radical resection is divided into three categories: A, B, and C. Patients with no tumor residue were defined as radical Cur A, while those with an obvious tumor residue were defined as radical Cur C. Those for whom the presence of a tumor residue was uncertain were classed as radical Cur B.
The primary outcome of this study was anastomotic leakage. This includes CT imaging evidence of leakage, as well as the clinical drainage of feces, accompanied by signs of peritonitis infection. The second outcome was overall survival rate.
All statistical analyses were performed using the SPSS software package for Macs (SPSS version 22; IBM, Tokyo, Japan). Differences were tested using Chi-square and Fisher's exact tests for classification variables. Survival curves were plotted by the Kaplan–Meier method and analyzed with a log rank test. p<0.05 was considered statistically significant.
Results
Between April 2007 and December 2015, a total of 307 patients with low rectal cancer were enrolled into this study: 140 and 167 patients without and with DS, respectively. The total incidence of anastomotic leakage was 10.7% (33/307) in laparoscopic LAR. The long-term survival rate of the anastomotic leakage group decreased significantly compared with that of the group without anastomotic leakage (Figure 1). Basic clinicopathological parameters are presented in Table I. No significant differences were observed between the two groups with regard to age, BMI, ASA classification, preoperative complications, tumor size, tumor gross type, differentiation, CEA level and depth of infiltration. However, in the DS group, the proportion of male patients was significantly higher (76.05% vs. 55.71%, p=0.03) and the tumor location was relatively low (Rb: 14.29% vs. 55.69%, p<0.001); discharge was also apparent a few days later (15.4±1.5 vs. 11.4±1.2 days, p=0.04).
The type and frequency of postoperative complications and the frequency of reoperations are shown in Table II. Complication rates were significantly higher in patients with DS (40.72% vs. 25.00%, p=0.003). Small bowel obstruction occurred more frequently in patients with DS (16.17% vs. 2.86%, p<0.001). In addition, complications related to the stoma occurred in eight patients, including stoma bleeding, peristomal dermatitis, peristomal abscess, stoma inverse and dehydration due to diarrhea in patients with DS.

Kaplan–Meier survival curves depicting outcomes between leakage and no leakage groups in LAR.
The demographics and clinical data of leakage patients undergoing LAR are presented in Table III. Anastomotic leakage was observed in 11.43% of patients without a DS and in 10.18% of patients with a DS. However, a significant difference was not observed in the incidence of anastomotic leakage between the two groups. There was also no significant difference in gender, age, preoperative diabetes, cerebrovascular disease, hypertension and ischemic heart disease. But the tumor location was relatively low in the DS group (Rb: 70.59% vs. 6.25%, p=0.003), and the tumor diameter for most such patients was greater than 5 cm (64.71% vs. 18.75%, p=0.007). In addition, the circumferential tumor resection rate (64.71% vs. 93.75%, p=0.04) and radical resection degree (Cur A & B: 76.47% vs. 100%, p=0.038) were significantly decreased. Although the DS group had many high-risk factors, anastomotic leakage did not increase, but actually slightly decreased in terms of a percentage. Therefore, a DS did not appear to reduce the incidence of anastomotic leakage in the high-risk group.
Surgical details are shown in Table IV. In the LAR + DS group, the postoperative discharge time was relatively long (11.4±1.2 vs. 15.4±1.5 p=0.04; Table I). However, no significant difference was observed in operating time, blood loss and food intake time between the leakage groups. The LAR group, however, had cases of reoperation related to anastomotic leakage and death.
In multivariate analysis, operating time was associated with a higher rate of leakage in LAR [odds ratio (OR) 8.772, 95% confidence interval (CI)=1.002-1.012, p=0.027]. The gender, Rb, DS, and preservation of the left colonic artery were not independent risk factors for anastomotic leakage (Table V).
Clinicopathological parameters LAR & LAR plus DS.
Next, we matched the Ra-LAR group with the Ra-LAR+DS group, and removed patients with obvious tumor remnants (Cure C), signet-ring cell and mucinous carcinoma in the Ra-LAR+DS group. No significant differences were observed in basic clinicopathological parameters except that the proportion of male patients was significantly higher (80% vs. 42.22%, p=0.0002) in the Ra-LAR+DS group. Bowel obstruction occurred more frequently in patients with DS (13.33% vs. 2.22%, p=0.049). A significant difference was not observed in the incidence of anastomotic leakage between the two groups [11.11% vs. 6.67%, not significant (N.S.)] (Table VI).
Morbidity after laparoscopic LAR with or without diverting stoma.
Demographics and clinical data of leakage patients undergoing LAR.

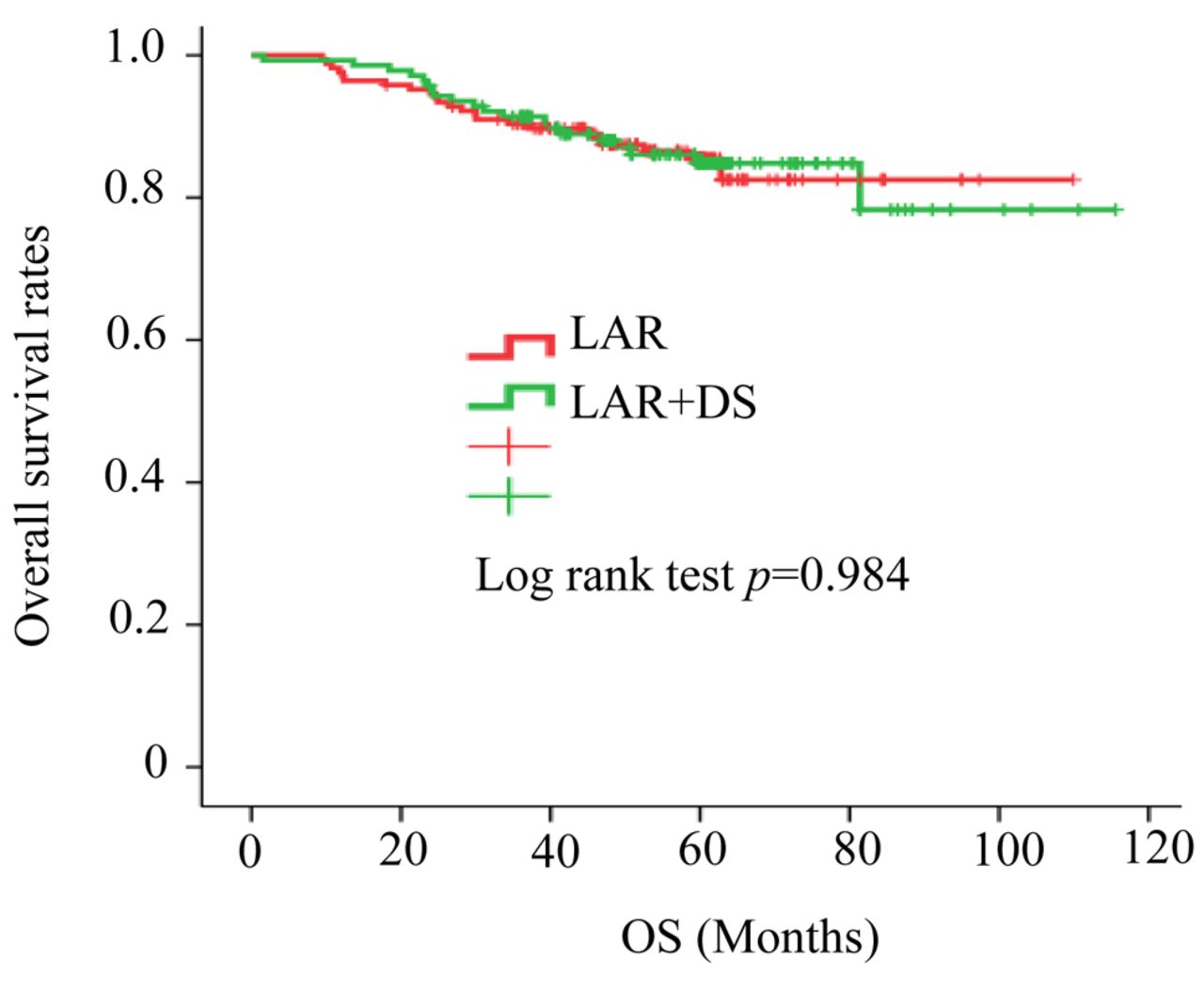
Kaplan–Meier survival curves depicting outcomes between LAR and LAR + DS groups.
Clinical outcomes of LAR in leakage patients with/without diverting stoma.
When the groups, with or without a DS, were compared for long-term survival, a significant difference was not found in LAR vs. LAR+DS (Figure 2) or in Ra-LAR vs. Ra-LAR+DS (Figure 3).
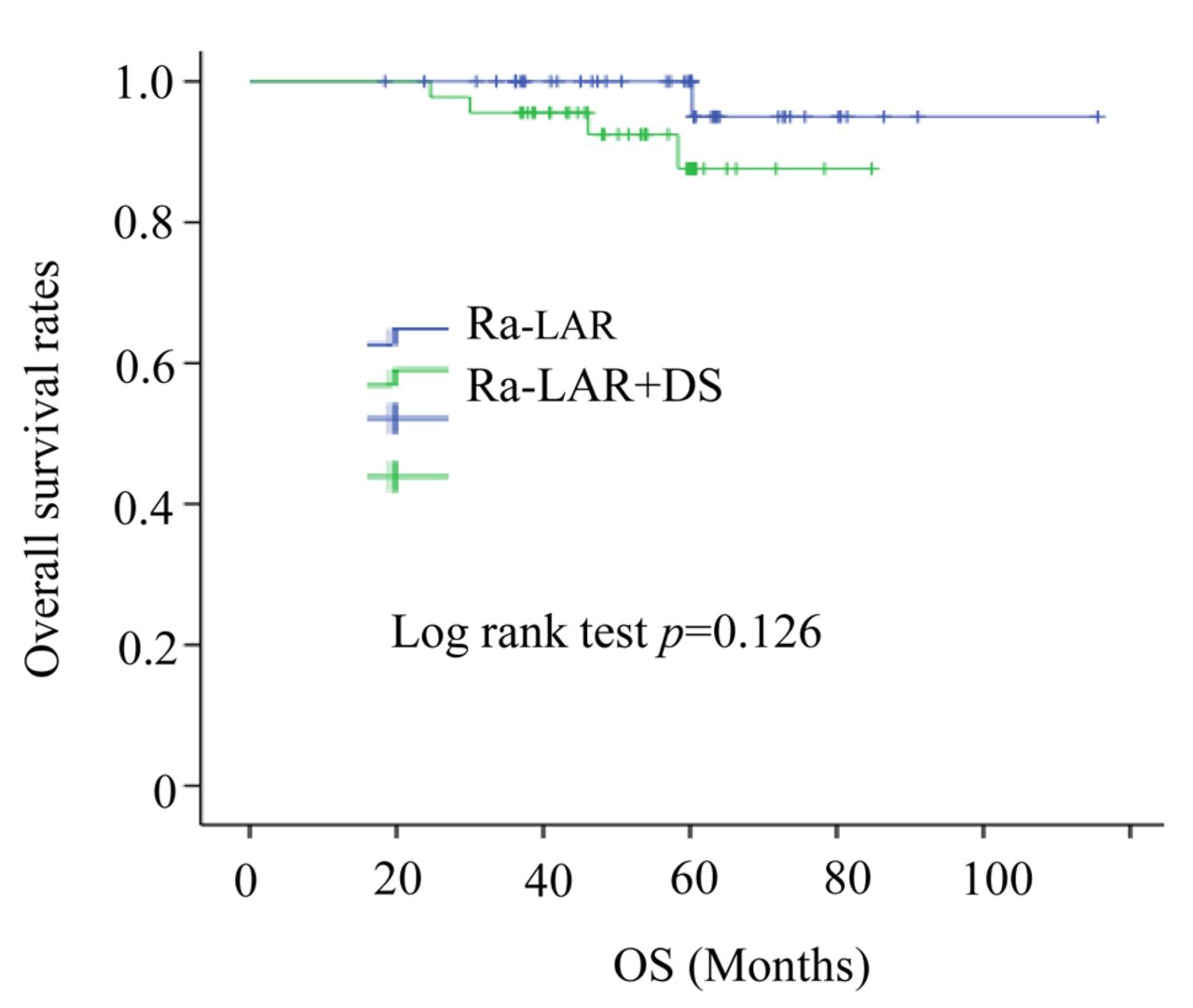
Kaplan–Meier survival curves depicting outcomes between Ra-LAR and Ra- LAR + DS groups.
Multivariate logistic regression analysis evaluating possible risk factors associated with leakage in LAR.
Discussion
Anastomotic leakage is the most dreaded complication in patients undergoing surgery for rectal cancer. It is not only related to postoperative morbidity and mortality but also with local recurrence and the survival of patients (4, 15-17). In this study, we found that a patient group with anastomotic leakage showed significantly lower long-term survival. Many reports exist on how anastomotic leakage, age, gender, intraoperative bleeding, BMI, preoperative radiotherapy and chemotherapy, pelvic drainage, tumor size, tumor location, degree of anastomosis and other risk factors are considered as high-risk factors in anastomotic leakage (2, 7, 18-21). Therefore, in our practice, we used a DS in male patients with a low tumor location and large tumor diameter.
Surgeons have used a myriad of techniques in order to avoid anastomotic leakage. After a colorectal DST anastomosis, performing a mechanical leak test, including an air leak test, and methylene blue leak test will highlight any leaks, but will not pinpoint the specific leak site. In comparison, an intraoperative endoscopic examination of the anastomotic site allows the surgeon a direct luminal visual evaluation and, if necessary, therapeutic intervention (22-24). Although an anastomotic leakage by DST technique usually occurs at the junction of DST cutter nails, it has been reported that side-to-side anastomosis may be a useful method in laparoscopic surgery (14). In this study, surgeons in all cases routinely used a side-to-end anastomosis to avoid a leak at the overlap of anastomotic staples. Even so, there is no way to completely prevent an anastomotic leak.
Clinicopathological parameters for Ra-LAR & Ra-LAR + DS.
Debate exists on whether to create a DS for patients undergoing surgery for rectal cancer. Some studies have shown that DS does not reduce the incidence of anastomotic leakage (25, 26). However, other studies have shown the opposite. Further, such studies suggest that DS aid in avoiding serious complications (2, 27). Stoma site complications, such as outlet obstructions, dermatitis and abscesses, are not to be ignored (28). In our study, we found that postoperative stoma complications may directly affect the number of days spent in hospital. Pertinently, this may delay the commencement of adjuvant chemotherapy.
In this study, although a significant difference in anastomotic leakage between two LAR groups, with and without DS, was not found, it was observed that patients in the DS group had more high-risk factors, such as being male, and having a lower tumor location. No deaths occurred in the DS group, and the reoperation rate decreased when anastomotic leakage occurred, although this was not statistically significant. It is generally believed that a DS may reduce the clinically adverse effects of anastomotic leakage, such as peritonitis and sepsis, rather than prevent leakage (29).
Our study suggests that operating time is associated with a higher rate of leakage in LAR. This, in turn, suggests that it is critical for young surgeons to rapidly improve their learning curve for surgery for LAR. For rectal cancer above the peritoneum, a DS did not reduce the incidence of postoperative anastomosis but may increase postoperative intestinal obstruction. It has also been reported that avoiding placement of DS may prevent postoperative intestinal obstruction (30), therefore, it is necessary to reconsider the current strategy of DS. In addition, there was no significant difference in postoperative long-term survival rates between LAR groups with and without a DS.
Although these data are novel, because of the limited number of patients investigated, it is difficult to draw reliable conclusions. Further studies, including a large multi-institutional randomized controlled prospective study, to evaluate the advantages and disadvantages of DS are required.
Conclusion
Operating time was associated with a higher rate of leakage in laparoscopic LAR in patients with rectal cancer. A DS did not reduce anastomotic leakage but increased the risk of postoperative intestinal obstruction in laparoscopic LAR. This suggests that DS may not be necessary for a low rectal resection if the tumor is located above the peritoneum.
Acknowledgements
The Authors thank experts of BioMed Proofreading for English copyediting.
Footnotes
Authors' Contributions
LMW and YH drafted the manuscript and provided the original pictures. TI, HK, KH, SI, TO, NO, and SY reviewed the manuscript. All Authors read and approved the final manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no competing interests regarding this study.
- Received August 1, 2019.
- Revision received August 20, 2019.
- Accepted August 28, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}