


Abstract
Background/Aim: Due to the increasing number of immunocompromised patients and widely used autologous stem cell transplantation procedures, clinicians have to face with the emergence of infectious diseases. In this setting, we mainly focus our interest on cytomegalovirus (CMV) testing and only in some cases on other herpesviruses (HHV). Herein, we present monitoring of HHV-6 virus re-activation and infection in patients after autologous stem cell transplantation. Materials and Methods: One hundred and twenty-one blood and 2 cerebrospinal fluid specimens from 35 patients were tested for the presence of HHV-6 DNA. Results: In 4 patients, a positive HHV-6 signal was detected. In 1 patient, simultaneous detection of CMV and HHV-6 could be observed; however, a low copy number result during CMV testing was obtained. Delayed engraftment or other clinical signs of infection could not be detected in patients with a positive HHV-6 result, except in the case of patient 4 who had limbic encephalitis due to HHV-6 reactivation. Conclusion: Because of the possible severe manifestations of HHV-6 infection in immunocompromised patients, screening of HHV-6 infection or reactivation is recommended as part of the routine laboratory procedure.
Human herpesvirus 6 (HHV-6) is a member of Herpesviridae family, isolated, at first, from patients with AIDS and lymphoproliferative disease (1, 2). A large proportion of the population is infected with HHV-6 causing primary infection, as roseola, mainly in early childhood (3). Most cases of primary infection are asymptomatic and benign; however, sometimes febrile convulsive events may occur. Thereafter, the virus is present in its latent form in the host and can be re-activated due to immunosuppressive circumstances, such as after intensive chemotherapeutic treatment, solid-organ transplantation and bone marrow and stem cell transplantation. The first case of fatal encephalitis after bone marrow transplantation was described by Drobyski et al., in 1994 (4). The risk of HHV-6 re-activation is associated with allogeneic, mainly cord blood, transplantation and rarely with autologous stem cell transplantation. In this case, symptoms range from asymptomatic infection to severe manifestations (encephalitis, pneumonitis, hepatitis and myelosuppression), prolonged haematopoietic recovery and graft rejection. Encephalitis is one of the most frequent and life-threatening clinical complication of reactivation (3). Reactivation could be documented by molecular techniques in 40-60% from peripheral blood and in 1-2% from cerebrospinal fluid associated with neurological signs (5-7). In addition to this, diagnosis may be possible based on the detection of viral antigens or antibodies from various clinical specimens; however, the interpretation of results is complicated because of the high seroprevalence, immunosuppression and latent form of the virus (3).
There are several studies evaluating risk factors for viral re-activation mainly in the case of cytomegalovirus (CMV), while other herpesviruses are not frequently monitored in auto-trasplanted patients. Herein, we retrospectively analyzed HHV-6 DNA by the polymerase chain reaction (PCR) method from plasma and cerebrospinal fluid samples (CSFs) in patients who underwent autologous stem cell transplantation.
Materials and Methods
Between 2010 and 2012, 35 consecutive patients with autologous peripheral stem cell transplantation were observed in our institution (19 female and 16 male with a median age of 60 years; range, 22-71 years). Underlying diseases were multiple myeloma (MM), Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL) in 29, 2 and 4 cases, respectively. One hundred and twenty-one anticoagulated (EDTA) blood and 2 CSF samples of 35 patients were collected; at least 2 blood samples from each patient (in 7 cases, only 1 specimen). All patients received antiviral prophylaxis against herpes simplex virus-1/2, (HSV-1/2) and varicella-zoster virus (VZV) (acyclovir 400 mg twice daily), antibacterial (levofloxacin 500 mg once a day) and antifungal drugs (fluconazole 150 mg once a day) for prevention. Engraftment was defined if the neutrophil and platelet count was more than 0.5 and 20×109/l on 2 consecutive days without any support, respectively.
Characteristics of patients with HHV-6 positivities.
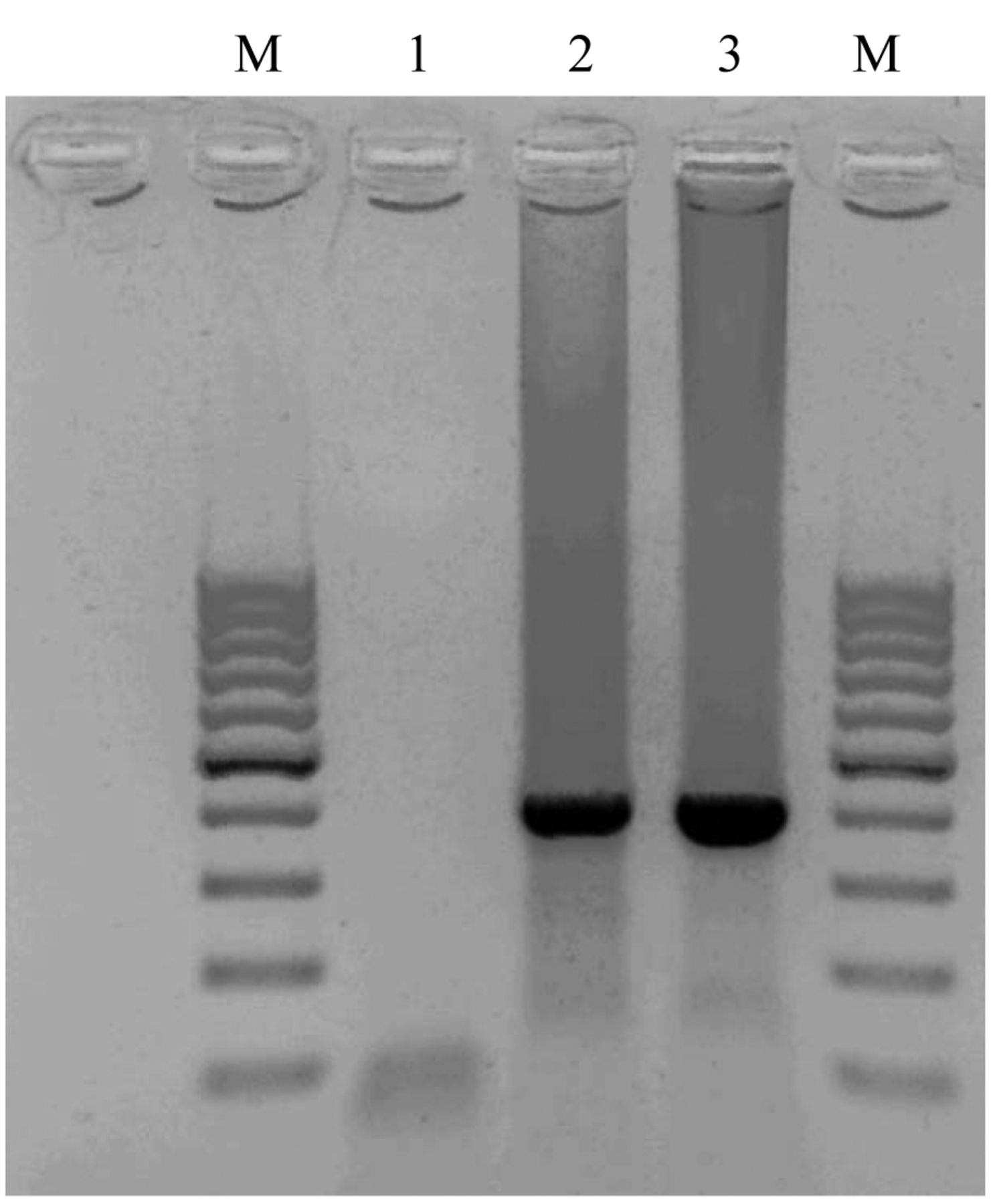
Plasma specimens and, in the case of neurological manifestations, CFSs were tested for the presence of CMV, HSV-1/2, EBV DNA using real-time PCR (artus CMV LC PCR Kit; Qiagen, Hilden, Germany, artus HSV-1/2 LC PCR Kit; Qiagen and artus EBV LC PCR Kit; Qiagen). HHV-6 nested PCR was performed with the use of DreamTaq Green PCR Mastermix (2×) (ThermoScientific; Waltham, MA, USA) containing 2× DreamTaq Green buffer, 0.4 mM dNTP, 4 mM MgCl2. The primers derived from the immediate early gene locus of two variants of the HHV-6 strain (U1102) (8). Ten microliters of 1× DreamTaq Green PCR Mastermix, 0.4 μl 25 mM MgCl2, 0.3 μl 25 pmol HHV6-F out primer (5’-TTC TCC AGA TGT GCC AGG GAA ATC C-3’), 0.3 μl 25 pmol HHV6-R out primer (5’-CAT CAT TGT TAT CGC TTT CAC TCT C-3’), 4 μl H2O, and 5 μl purified DNA template were used for PCR. For the next PCR, 10 μl 1× DreamTaq Green PCR Mastermix, 0.4 μl 25 mM MgCl2, 0.3 μl 25 pmol HHV6-F in primer (5’-AGT GAC AGA TCT GGG CGG GCC CTA ATA ACT T-3’), 0.3 μl 25 pmol HHV6-R in primer (5’-AGG TGC TGA GTG ATC AGT TTC ATA ACC AAA-3’), 4 μl H2O and 5 μl template (from the samples amplified in the course of the previous PCR) were set-up. The amplified PCR product was detected using gel electrophoresis and two variants of HHV-6 were identified on the basis of the size of the amplified products (variant A showed 195 bp, while variant B gave 423 bp of PCR products).
Results
Four out of 35 (11.4%) observed patients after transplantation had HHV-6 positivity in the peripheral blood or CSF by PCR method. Two patients had HL, while two patients suffered from MM. Patients with MM had been given a combination of thalidomide (Thal) and dexamethasone (Dex); in HL patients, a combination treatment of ABVD (Adriamycin, Bleomycin, Vinblastine and Dacarbazine) and DHAP (Dexamethasone, Cisplatin, Cytarabine and Q3-4w) was applied. The HHV-6 variant A was detected only from MM patients, while the HHV-6 variant B was amplified from HL. In the case of 1 MM patient with HHV-6 variant A, CMV DNA was also detected with a low copy number (273 copies/mL) from the plasma specimen using real-time PCR. The patients' characteristics are summarized in Table I. Three of 4 patients did not show clinical signs of infection at the time of sample collection, while patient 4 had limbic encephalitis.
Patient 4, a 32-year-old man with stage II/A Hodgkin lymphoma, nodular sclerosis subtype, EBV-negative), was admitted to our haematology department in 2011. The patient had been treated with six cycles of chemotherapy according to ABVD protocol that conferred complete remission (9). Four month later, the positron emission computer tomography (PET CT) showed early relapse in his right supraclavicular and upper mediastinal lymph nodes, thus, treatment with the DHAP regimen was started. After receiving a second course of DHAP, peripheral blood stem cell harvest was performed (5.56×106/body weight; CD34-positive cells). The patient was conditioned according to BEAM (Carmustine (BiCNU), Etoposide, Arabinoside and Melphalan) protocol followed by autologous stem cell infusion. On post-transplant day 17, the patient was referred to a neurologist because of confusion. Elevated liver enzymes and differences in the kidney enzyme levels were observed, while fever appeared and disappeared periodically. The first neurological examination could not reveal any focal neurological signs. The patient was vigil, disoriented in time and space but oriented in own data; however, he was psychomotorically slow. No signs of neck-stiffness and meningeal irritation could be observed. Cranial nerves without abnormalities, normal muscle tonus and strength and distally decreased vibration sensation in both legs could be registered. Minimal symmetrical hyporeflexia in the Achilles and plantar deep tendon reflexes and insecurity at Romberg test could be noticed. Otherwise, tendon reflexes, coordination and cerebellar tests proved to be normal. The neurological examination pointed to a polyneuropathy (most probably drug-induced) and there was a suspicion of hepatorenal insufficiency and metabolic encephalopathy.
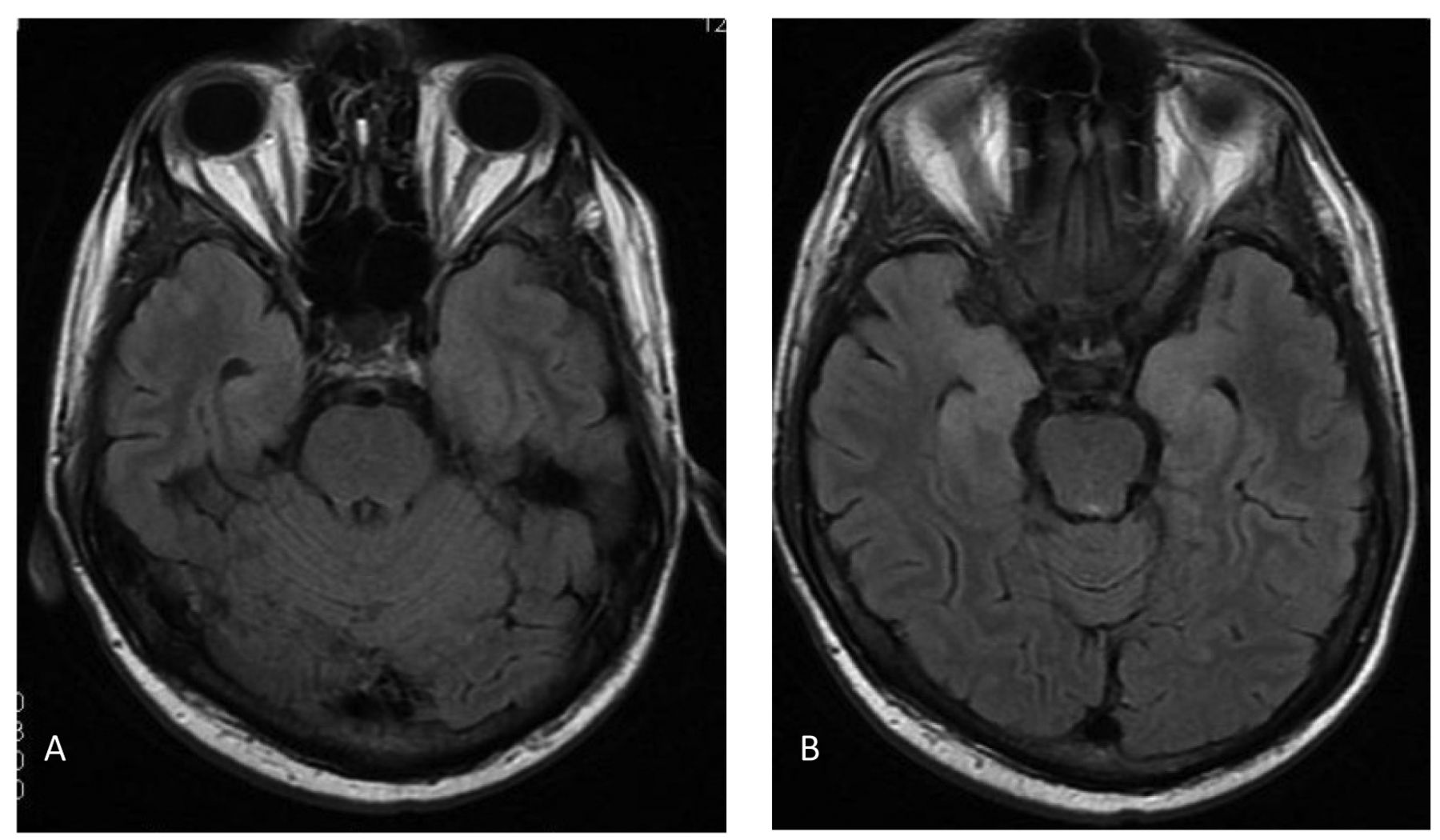
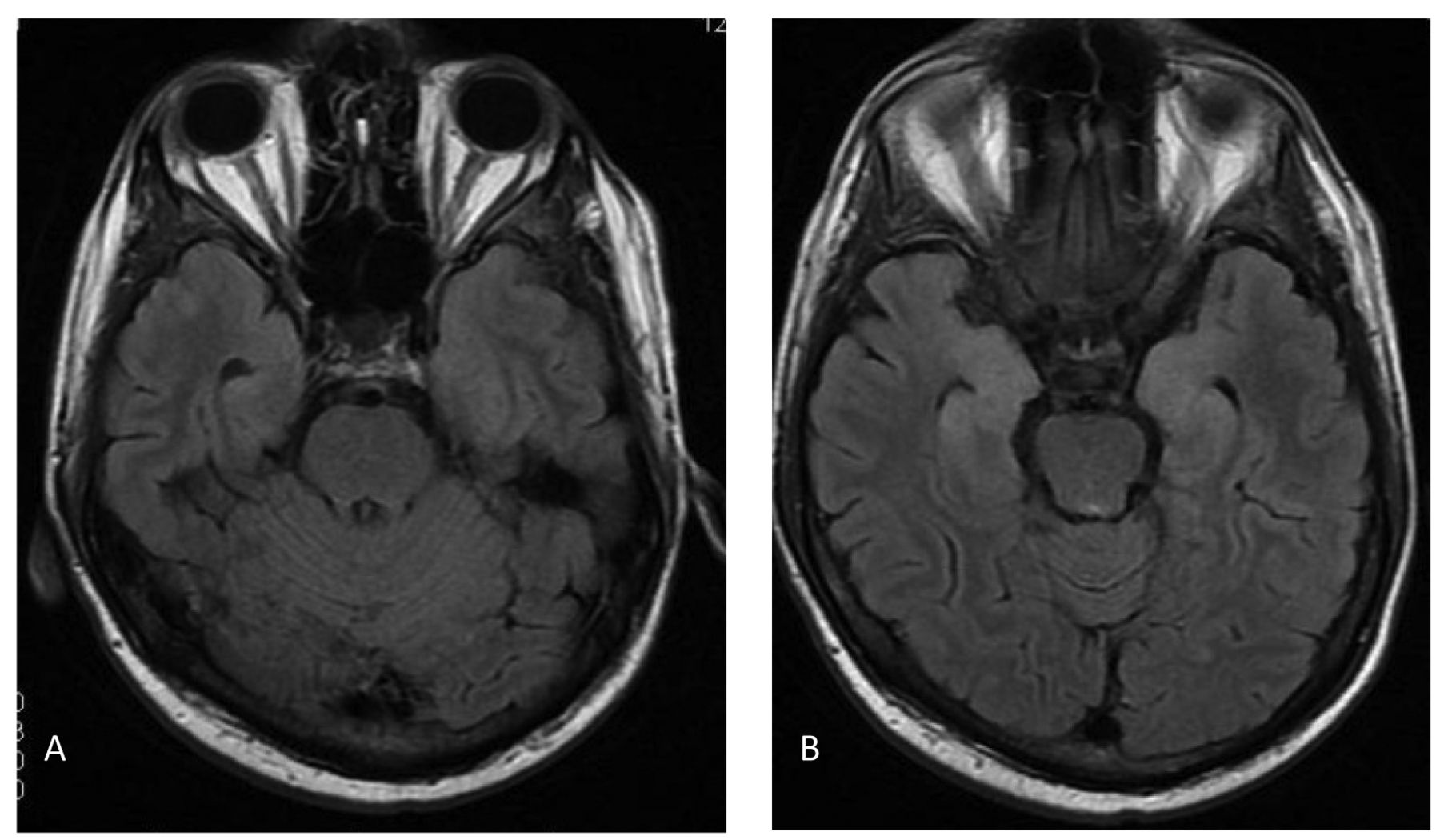
Magnetic resonance imaging (MRI) of the brain on 19th post-transplant day: fluid attenuated inversion recovery (FLAIR) showing bilateral encephalitis in the temporal lobe, mainly in the region of the hyppocampus (A). Diffusion weighted images with signal hyperintensities (B).
In November, 2012, because of deterioration in the patient's orientation and his febrile state, a suspicion of infectious origin of this condition arose. After some unsuccessful lumbar punctures, on the basis of findings during the MRI scan of the brain, the possibility of viral encephalitis, most probably herpes-encephalitis caused by HHV-6, in the temporal lobes had been assumed (Figure 1A-B). The patient was treated with gancyclovir, steroid and dexamethasone therapy intravenously. The patient's condition was improving after the introduction of the therapy. His status was vigil and partially disoriented; he had slow psychomotorium. Pupil dilatations on both sides were reactive for light. His muscles were hypotonic over all extremities. No pathological reflexes and focal neurological signs could be observed. Lumbar puncture was performed with minimal artificial bleeding (24.661 M/l of red blood cells (RBCs), 20 M/l of white blood cells (WBCs) and 1.22 g/l of total protein). Cytology in CSF revealed excessive amount of RBCs with mixed cell count of WBCs dominated by segmented neutrophils. Real-time PCR tests were negative for HSV-1/2, CMV, EBV and enteroviruses (Enterovirus RNA Kit, DiaPro; Milan, Italy) from plasma and cerebrospinal fluid samples. HHV-6 nested PCR was done and HHV-6-specific nested PCR gave positive results for the HHV-6 B variant from both sample types (Figure 2). Three days later, deterioration in the patient's condition could be observed due to epileptic seizures. Partial seizures with oral and manual automatisms, confusion, repetitive jerking movements in both extremities could be registered. Levetiracetam (500 mg twice daily intravenously) was started and 2 days later the dose was increased to 1,000 mg twice daily and clobazam (10 mg orally 3 times a day) was introduced.
In December, 2012, lumbar puncture was performed; CSF was water clear with 1 M/l of RBCs, 1M/l of WBCs and 0.62 g/l of total protein. Cytology testing showed 1-2 RBCs, 18 lymphocytes and 2 macrophages. HHV-6-nested PCR gave a positive result but the CSF was negative for HSV-1/2, CMV, EBV, and enteroviruses. Parenteral gancyclovir (500 mg twice daily) therapy was taken for 21 days and followed by oral valgancyclovir (450 mg twice daily) for four weeks. His mental and neurological state recovered and could be discharged from the transplant unit on 58 post-transplant day (Figure 3).
Discussion
Autologous peripheral stem cell transplantation is a widely used procedure in the treatment of multiple myeloma, Hodgkin's and non-Hodgkin's lymphoma (10). In this patient group, viral infection is one of the most important causes of post-transplant morbidity and mortality. In this setting, HHV-6 infection represents a very rare and severe life-threatening complication in autologous recipients. Pagter et al. summarised several studies in which they analysed HHV-6 re-activation during haematopoietic stem cell transplantation. Eighteen studies were examined and, in the case of 12 of these, 1 month after haematopoietic stem cell transplantation, HHV-6 re-activation occurred. The incidence of HHV-6 re-activation ranged from 28% to 78% in allogeneic and autologous patients. Delayed platelet engraftment showed a significant association with the presence of HHV-6 DNA (11). Imbert-Marcille et al. studied 846 peripheral blood samples of 92 consecutive patients (526 from autologous and 320 from allogeneic transplant recipients) for HHV-6 DNA; 18.3% of these samples gave positive results. Similarly to other studies, the incidence of active HHV-6 infection was 42.5 % after both autologous (27/64) and allogeneic (12/28) transplantation (5). Ljungman et al. also confirmed that high HHV-6 viral load was associated with the development of HHV-6 disease, myelosuppression and prolonged engraftment, mainly in megakaryocytic and erythroid cell lineages (12). In addition to this, only patient 4 showed clinical signs of infection due to HHV-6 re-activation. In our study, the number of HHV-6-positive samples was lower than in previous studies; however, the number of patients analyzed was also lower. Delayed engraftment could not be detected in our study. In immunocompromised patients with signs of encephalopathy, change in mental status and loss of short-term memory may differentiate several causes not only intra-cerebral bleeding from thrombocytopaenia, direct toxicity of drugs, electrolite and other metabolic disturbances but also infectious complications. Bommer et al. described encephalitis and pneumonitis caused by HHV-6 in a young patient with relapsed Hodgkin's lymphoma who underwent autologous stem cell transplantation. In that case, mental disturbances and convulsion were developed without abnormality in the first MRI image of the brain on the 12th post-transplant day, while CT scan of the chest showed diffuse interstitial pneumonia on both sides of the lung. Bronchoalveolar lavage and CSF were positive for HHV-6 DNA. The patient was successfully treated with foscarnet followed by oral valgancyclovir for another 6 weeks (13). We also showed a patient with encephalitis due to HHV-6 re-activation shortly after transplantation. Multiple EDTA blood and two CSF specimens from this patient gave positive HHV-6 PCR results, while no viral or bacterial pathogens could be detected as a cause of encephalitis. Because of confirmed HHV-6 encephalitis, parenteral gancyclovir was started followed by oral valgancyclovir. During this treatment, the neurological signs resolved successfully with minimal short-term memory dysfunction; his haematological disease is now in complete remission. Similarly to our findings, Imbert-Marcille et al. also confirmed that active HHV-6 infection frequently occurred 3 or 4 weeks after transplantation (5). However, lacking randomised clinical trials, treatment with gancyclovir, foscarnet or cidofovir has been recommended for patients with HHV-6 encephalitis (14). In our case, gancyclovir treatment resolved the neurological signs with minimal sequelae.
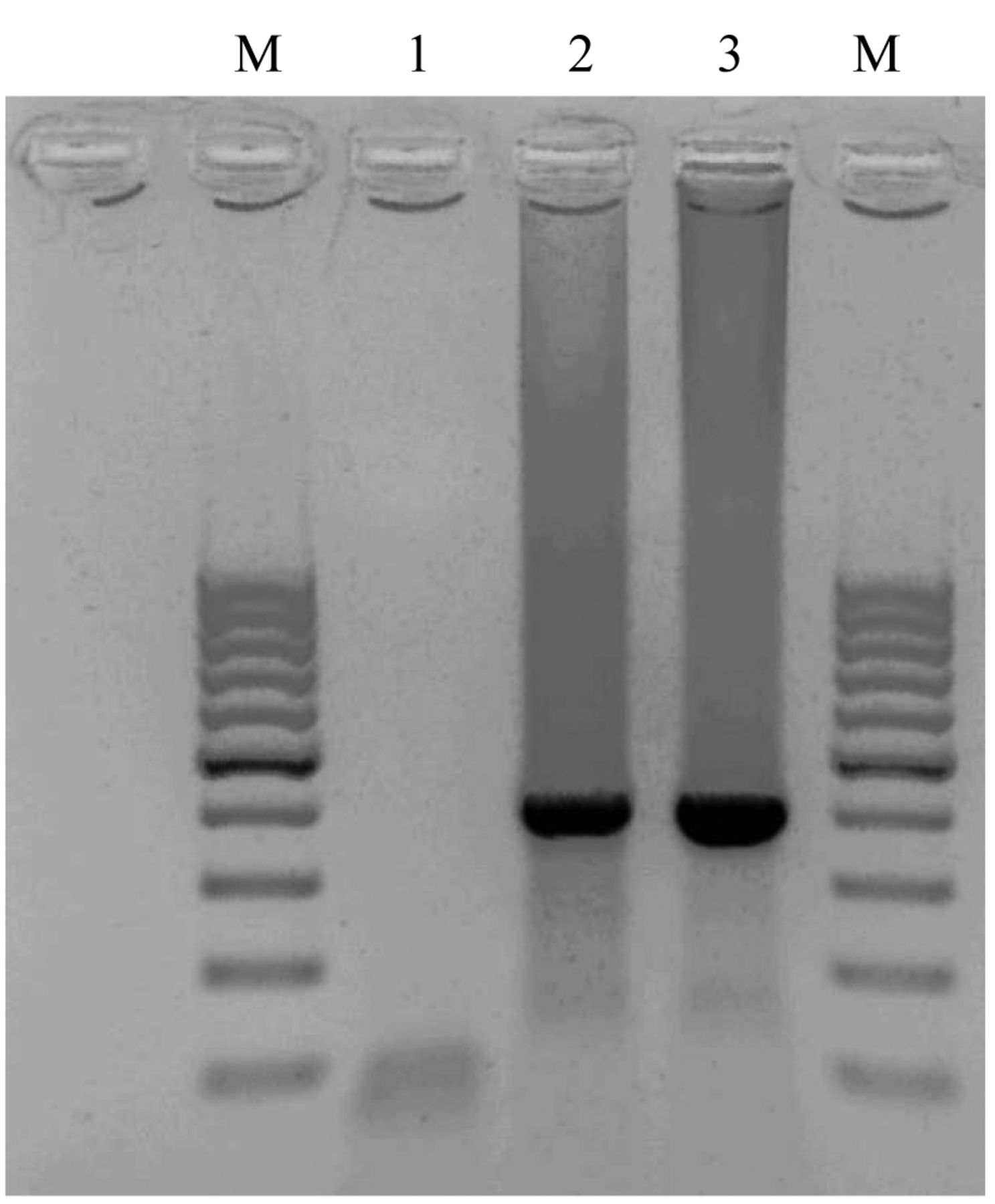
Detection of HHV-6-specific PCR product by agarose gel electrophoresis (M-Gene Ruler 100 bp DNA ladder; 1, negative control; 2, positive control (HHV-6 B); 3, HHV6 B PCR product from cerebrospinal fluid sample).

Signal hyperintesities resolved on both sides of temporal lobe, consequent atrophia with dilatation of sulcus and chambers.
Because of the increasing number in immunocompromised patients and the widely used autologous stem cell transplantation procedure, the clinicians need to monitor not only CMV viral load but also the detection of other herpesviruses, including HHV-6 virus infection or reactivation, an important trait for achieving more reliable data about their impact for the management of these infections as it is crucial to determine the optimal regimen and duration of antiviral therapy.
Footnotes
-
Funding
None.
-
Conflicts of Interest
The Authors have no conflict of interest to declare.
-
Ethical approval
Not required.
- Received July 30, 2014.
- Revision received September 22, 2014.
- Accepted September 29, 2014.
- Copyright © 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.